Comprehensive Introduction and Patho-Epidemiology
Phalangeal fractures and proximal interphalangeal (PIP) joint dislocations represent a substantial proportion of upper extremity trauma evaluated by orthopedic surgeons, hand specialists, and emergency physicians. These injuries, often dismissed by the lay public as "just a jammed finger," possess a profound potential for devastating long-term functional impairment if mismanaged. The delicate, highly constrained anatomical environment of the hand means that even minor degrees of malunion, rotational deformity, or articular incongruity can cascade into severe biomechanical deficits, stiffness, and post-traumatic osteoarthritis. Consequently, mastering the nuances of surgical intervention—specifically Open Reduction and Internal Fixation (ORIF) and Closed Reduction Percutaneous Pinning (CRPP)—is an absolute prerequisite for any surgeon treating hand trauma.
Epidemiologically, phalangeal fractures account for approximately 10% of all human skeletal fractures and represent the most common fractures of the upper extremity. The incidence peaks in two distinct demographic cohorts: young males (aged 15 to 30 years) primarily due to sports injuries, occupational hazards, and interpersonal violence, and an older population (over 65 years) where falls from a standing height result in low-energy osteoporotic fractures. The proximal phalanx is the most frequently fractured bone in the hand, followed closely by the middle phalanx and the metacarpals. Industrial accidents, particularly crush injuries and high-energy axial loads, frequently result in complex, comminuted, or open fracture patterns that challenge even the most experienced microsurgeon.

Figure 67-45A: Crush injury to the small finger resulting in a middle phalangeal fracture.
The pathophysiology of these injuries is intrinsically linked to the mechanism of trauma. Direct blunt trauma typically yields transverse or comminuted fracture patterns with significant associated soft tissue envelopes crushing. Conversely, indirect trauma, such as torsional forces applied to a fixed digit, classically generates spiral or long oblique fractures. Axial loading, particularly when the digit is in slight flexion, frequently results in intra-articular fractures at the base of the middle phalanx, leading to the dreaded PIP joint fracture-dislocation. Understanding these mechanisms is not merely an academic exercise; it directly informs the surgeon’s anticipation of inherent instability, soft tissue compromise, and the optimal trajectory for surgical fixation.

Figure 67-45B: AP radiograph demonstrating the inherently unstable nature of the fracture.
Furthermore, the socioeconomic impact of phalangeal fractures is staggering. Because the hand is the primary tool for human interaction with the environment and the workplace, prolonged immobilization or permanent stiffness translates to significant lost wages, decreased productivity, and diminished quality of life. The overarching goal of surgical management must therefore transcend mere radiographic alignment; it must aggressively pursue the restoration of a stable, congruent skeletal architecture that permits the earliest possible mobilization of the gliding soft tissue structures.
Detailed Surgical Anatomy and Biomechanics
The management of phalangeal fractures requires a profound, almost intuitive understanding of hand biomechanics and the delicate interplay between the intrinsic and extrinsic musculotendinous units. The phalanges are not isolated osseous struts; they are dynamic levers completely enveloped by a complex, unforgiving soft tissue apparatus. The extrinsic tendons (flexor digitorum superficialis [FDS], flexor digitorum profundus [FDP], and extensor digitorum communis [EDC]) and the intrinsic muscles (interossei and lumbricals) exert continuous, predictable deforming forces on any fracture fragment.
In fractures of the proximal phalanx, the characteristic deformity is apex volar angulation. This predictable displacement is driven by the proximal fragment being flexed by the interossei, which insert onto the base of the proximal phalanx and the lateral bands. Simultaneously, the distal fragment is extended by the pull of the central slip of the extensor mechanism inserting on the dorsal base of the middle phalanx. These opposing forces create a volar apex that, if left unreduced, alters the moment arms of both the flexor and extensor tendons, resulting in a severe extensor lag at the PIP joint and a compensatory hyperextension at the metacarpophalangeal (MCP) joint.
Fractures of the middle phalanx present a more variable deformity pattern, entirely dependent on the fracture's location relative to the broad volar insertion of the FDS tendon. If the fracture occurs proximal to the FDS insertion, the proximal fragment is extended by the central slip, and the distal fragment is flexed by the FDS and FDP, resulting in an apex dorsal deformity. Conversely, if the fracture is distal to the FDS insertion, the proximal fragment is flexed by the FDS, and the distal fragment is extended by the terminal extensor tendon, yielding an apex volar deformity. Recognizing these biomechanical rules is critical for achieving and maintaining closed reduction, as well as planning the mechanical advantages of internal fixation.
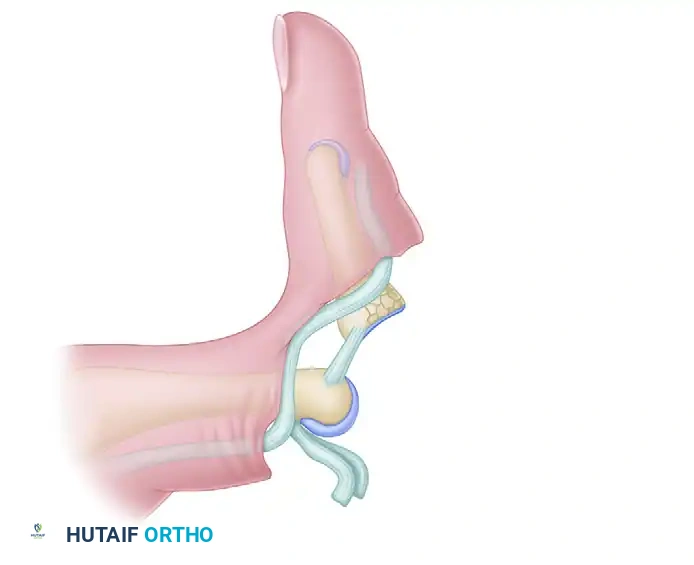
The PIP joint itself is a highly constrained ginglymus (hinge) joint, possessing an arc of motion from 0 to 110 degrees. Its stability is governed by a robust capsuloligamentous box. The collateral ligaments provide primary restraint to coronal plane deviation, while the thick, fibrocartilaginous volar plate prevents dorsal subluxation and resists hyperextension. The volar plate is firmly attached to the base of the middle phalanx but has a more proximal, membranous origin from the proximal phalanx, characterized by the checkrein ligaments. Disruption of this complex, particularly in the setting of an intra-articular fracture of the volar lip of the middle phalanx, obliterates the joint's intrinsic stability, leading to immediate and persistent dorsal subluxation driven by the unopposed pull of the central slip.

Exhaustive Indications and Contraindications
While a vast majority of non-displaced or stable extra-articular phalangeal fractures can be managed non-operatively with buddy taping, aluminum foam splints, or custom thermoplastic orthoses, surgical intervention becomes absolute when the biomechanical integrity of the hand is compromised. The decision to operate must be meticulously calculated, weighing the benefits of anatomical reduction against the iatrogenic trauma inflicted upon the gliding planes of the extensor and flexor mechanisms.
Surgical intervention via ORIF or CRPP is strictly indicated for fractures demonstrating unacceptable angular or rotational deformity. Rotational malalignment is arguably the least tolerated deformity in the hand. A mere 5 degrees of malrotation at the level of the proximal phalanx can translate to 1.5 cm of digital overlap (scissoring) at the fingertips during composite flexion. This scissoring drastically impairs grip strength and fine motor dexterity. Surgeons must always assess rotation clinically by observing the cascade of the digits with the MCP and PIP joints passively flexed prior to final fixation; radiographic evaluation of rotation is notoriously unreliable.

Figure 67-45C: Lateral radiograph confirming displacement requiring stabilization.
Other absolute indications include unstable oblique or spiral fractures that inevitably shorten under the resting compressive forces of the flexor tendons. Intra-articular fractures with step-offs greater than 1 to 2 mm require anatomical restoration to mitigate the rapid onset of post-traumatic arthrosis. Fractures with significant segmental comminution, bone loss, or open injuries requiring extensive debridement also necessitate rigid stabilization, often with external fixation or bridge plating. Complex PIP joint fracture-dislocations, particularly those involving more than 30-40% of the volar articular surface, represent an absolute indication for surgical reconstruction to restore joint congruity and prevent chronic dorsal subluxation.
| Variable | Absolute Indications for Surgery | Relative Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|---|
| Deformity | Rotational malalignment (scissoring) | Angulation > 10-15° in coronal/sagittal plane | None | Mild angulation in non-dominant digit |
| Stability | Unstable spiral/oblique fractures | Failure of closed reduction | Severe medical comorbidities | Advanced age with low functional demand |
| Articular | Step-off > 1-2 mm, PIP fracture-dislocations | Joint subluxation > 30% | Active local soft tissue infection | Pre-existing severe osteoarthritis |
| Soft Tissue | Open fractures, neurovascular compromise | Multiple ipsilateral fractures | Lack of soft tissue coverage | Severe crush injury (delay internal fixation) |
| Bone Loss | Segmental defects requiring grafting | Severe comminution | Non-reconstructible osteoporotic bone | Non-compliant patient |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning is the cornerstone of successful phalangeal osteosynthesis. The margin for error in hand surgery is measured in millimeters, demanding rigorous preparation. High-quality, multi-planar radiographic imaging is mandatory. A true anteroposterior (AP), true lateral, and oblique view of the individual digit must be obtained. The true lateral view is particularly critical and often challenging to acquire due to the superimposition of adjacent digits; it requires the affected finger to be isolated, often using a specialized step-block or having the patient actively flex the uninvolved digits out of the radiographic beam.
For complex intra-articular fractures, particularly PIP joint fracture-dislocations and pilon-type fractures of the phalangeal bases, a fine-cut Computed Tomography (CT) scan with 3D reconstructions is highly recommended. CT imaging precisely delineates the size, number, and spatial orientation of articular fragments, which is invaluable for deciding between percutaneous pinning, lag screw fixation, volar plate arthroplasty, or hemi-hamate autograft reconstruction. Templating should be performed using digital software to select the appropriate implant sizes, typically ranging from 1.0 mm to 1.5 mm minifragment screws, or 0.035-inch to 0.045-inch Kirschner wires.

Figure 67-46A: Markedly unstable proximal phalangeal fracture.
Patient positioning and anesthesia are tailored to the complexity of the procedure and patient comorbidities. While traditional general anesthesia or regional blocks (axillary or supraclavicular) with an upper arm tourniquet remain standard, the advent of Wide Awake Local Anesthesia No Tourniquet (WALANT) has revolutionized hand fracture surgery. Utilizing a mixture of lidocaine and epinephrine allows the surgeon to perform the procedure without a tourniquet, minimizing ischemic pain. More importantly, WALANT permits intra-operative active movement testing. The surgeon can ask the patient to actively flex and extend the digit after provisional fixation to directly observe the fracture stability, the presence of impingement, and the absolute correction of rotational deformities prior to definitive closure.

Figure 67-46B: Belsky-Eaton pinning technique. The fracture is treated by percutaneous pinning across the MCP joint. Note the MCP joint is flexed at least 60 to 70 degrees, and the PIP joint is intentionally not crossed.
If a tourniquet is utilized, a forearm tourniquet is often preferred over an upper arm tourniquet for isolated digit procedures, as it is better tolerated by the patient under monitored anesthesia care. The arm is placed on a radiolucent hand table. A sterile mini-C-arm fluoroscopy unit is positioned perpendicular to the table, allowing the surgeon to seamlessly transition between AP and lateral views without manipulating the delicate fracture reduction. Meticulous skin preparation and draping must allow visualization of the entire hand and wrist to continuously assess the digital cascade.
Step-by-Step Surgical Approach and Fixation Technique
The Pratt Technique Open Reduction and Retrograde Pinning
For transverse or short oblique fractures of the proximal or middle phalanx that prove refractory to closed reduction, the Pratt technique provides a robust, direct method of visualization and stabilization. This technique is particularly useful when soft tissue interposition (such as periosteum or extensor mechanism) blocks anatomical reduction.
Surgical Steps:
1. Exposure: A dorsal longitudinal or slightly curved (lazy-S) incision is made over the fractured phalanx to prevent scar contracture. The skin and subcutaneous tissues are elevated as a full-thickness flap to preserve the delicate venous and lymphatic drainage, exposing the extensor tendon mechanism.
2. Tendon Incision: The extensor tendon is incised longitudinally, precisely in its midline. The tendon is carefully retracted radially and ulnarly to reveal the underlying periosteum and fracture site. Extreme care must be taken to minimize periosteal stripping, preserving the tenuous blood supply to the cortical bone.
3. Retrograde Drilling: Under direct visualization, the fracture is debrided of hematoma. A 0.035-inch or 0.045-inch K-wire is loaded onto a wire driver. The wire is drilled retrograde from the fracture surface into the medullary canal of the distal fragment, exiting the distal cortex and skin.
4. Reduction and Fixation: The fracture is now anatomically reduced using pointed reduction forceps. Once absolute interdigitation of the fracture ends is confirmed, the K-wire is driven antegrade (retrograde to the initial trajectory) across the fracture site and seated firmly into the subchondral bone of the proximal fragment. A second crossed K-wire can be added for rotational stability.
5. Deformity Correction: The digital cascade is rigorously inspected. While minor shortening (1-2 mm) may be biomechanically tolerated, rotational malalignment is strictly forbidden.
6. Closure: The extensor tendon is meticulously repaired using a running or figure-of-eight 4-0 or 5-0 non-absorbable or slowly absorbable suture. The skin is closed with interrupted nylon sutures.

Figure 67-45D: Postoperative AP radiograph showing the Pratt technique of crossed Kirschner wire fixation providing excellent alignment.

Figure 67-45E: Postoperative lateral radiograph confirming concentric reduction and stability.
Closed Reduction and Percutaneous Pinning CRPP
Unstable oblique or spiral fractures of the middle or proximal phalanx can frequently be managed via CRPP, avoiding the morbidity of a dorsal surgical approach and minimizing extensor tendon adhesions.
The technique relies on closed reduction utilizing longitudinal traction and manipulation, followed by percutaneous stabilization. The trajectory of the K-wires is of paramount importance. The K-wire should be inserted strictly midlaterally. Inserting pins directly dorsally tethers the extensor hood, while volar insertion risks impaling the flexor tendon apparatus, both of which will severely compromise postoperative digital excursion. Fluoroscopy is utilized to ensure the pins cross the fracture site perpendicularly to provide maximal mechanical advantage and compression. Pins are typically cut outside the skin and bent to facilitate removal in the clinic setting at 3 to 4 weeks.
The Belsky-Eaton Intramedullary Pinning Technique
Belsky and Eaton described a highly elegant, minimally invasive intramedullary pinning technique ideal for transverse or short oblique fractures of the proximal phalanx. This technique leverages the principles of ligamentotaxis and avoids violating the PIP joint.
Surgical Steps:
1. Positioning: The fractured proximal phalanx is manually reduced. The MCP joint is then acutely flexed to 90 degrees. This maneuver is critical: it tightens the collateral ligaments, pulling the fracture out to length via ligamentotaxis, and translates the extensor hood distally, moving it safely out of the pin's trajectory.
2. Pin Insertion: A single robust K-wire (0.045 or 0.062 inch) is introduced percutaneously at the dorsal aspect of the metacarpal head. It is driven across the flexed MCP joint and directed into the medullary canal of the proximal phalanx.
3. Intramedullary Passage: The wire acts as an intramedullary strut, crossing the fracture site and providing excellent coronal and sagittal alignment. Multiple passes must be avoided to prevent widening the entry portal and losing purchase.
4. Joint Protection: The advancing wire must not cross or violate the PIP joint articular surface. The proximal end of the pin is bent and cut outside the skin over the metacarpal head, allowing for simple outpatient removal once clinical callus forms.
Intra-Articular Phalangeal Base Fractures
Intra-articular fractures of the phalangeal bases demand anatomical perfection. The articular surface must be rigidly restored to prevent the rapid onset of post-traumatic osteoarthritis, joint subluxation, and devastating stiffness.
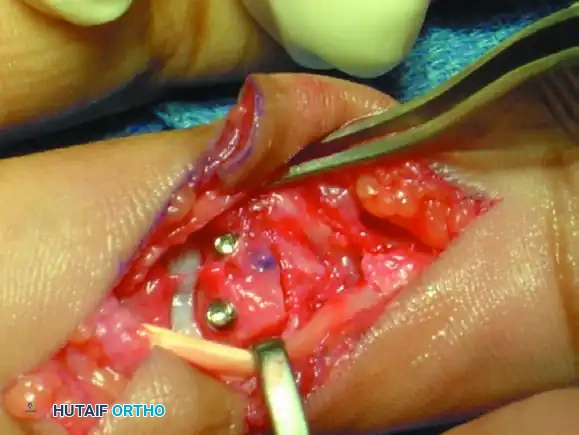
When the fracture pattern consists of large, reconstructible fragments, open reduction and internal fixation utilizing minifragment lag screws (1.0 mm, 1.3 mm, or 1.5 mm) is the gold standard. The surgical approach (dorsal or volar) is dictated by the location of the primary fragment. The fracture is exposed, hematoma evacuated, and the fragment anatomically reduced using a dental pick or small reduction forceps. A gliding hole is drilled in the near cortex, followed by a thread hole in the far cortex. The near cortex is countersunk to prevent the screw head from prominent impingement on gliding soft tissues. The lag screw is then inserted, providing absolute interfragmentary compression and permitting immediate postoperative active range of motion.

Figure 67-47A: Comminuted intra-articular fracture in the middle finger proximal phalanx base of an avid tennis player.

Figure 67-47B: Successful treatment achieved via precise lag screw fixation, restoring the articular congruity.
In cases of severe comminution (pilon-type fractures) where internal fixation risks devascularizing the tiny osteochondral fragments, a mini external fixator or dynamic traction device (e.g., Suzuki frame) is employed. This utilizes the principles of ligamentotaxis to maintain joint space, length, and alignment while allowing early passive motion to mold the healing articular surface.
Proximal Interphalangeal PIP Joint Fracture-Dislocations
A PIP joint fracture-dislocation is a catastrophic event characterized by the avulsion of the volar plate with an attached fragment of the volar base of the middle phalanx, resulting in dorsal subluxation of the remaining middle phalanx driven by the central slip.
The treatment algorithm is strictly dictated by the percentage of articular surface involved:
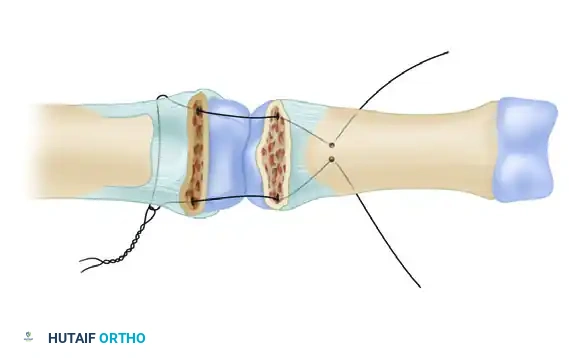
1. Large Single Fragment (>50% Articular Surface): These injuries are highly unstable. ORIF is mandatory. Fixation is achieved via a volar approach (Bruner incision), utilizing minifragment screws or a cerclage wire pullout technique if the fragment is too small for a screw but large enough to cause instability.
2. Small Fragments (<50% Articular Surface): If the joint can be concentrically reduced in flexion, the extension block splinting technique described by McElfresh, Dobyns, and O’Brien is highly effective. A dorsal block splint prevents the terminal 20-30 degrees of extension (the unstable zone) while permitting active flexion, encouraging remodeling and preventing stiffness.
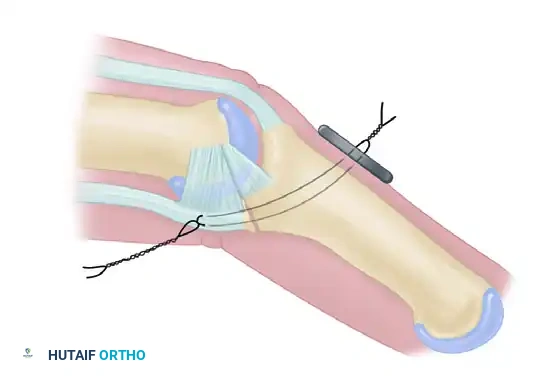
3. Chronic/Persistent Subluxation (≤40% Articular Surface): For delayed presentations or failures of conservative management, the volar plate arthroplasty (Eaton-Malerich technique) is utilized. The volar plate is advanced into the articular defect and secured into a trough at the base of the middle phalanx with pullout sutures, effectively resurfacing the defect and providing a robust volar restraint.
Advanced Reconstruction The Hemi-Hamate Osteoarticular Autograft
For severe, comminuted volar lip fractures involving >50% of the articular surface, or in cases of chronic, un-reconstructible dorsal fracture-dislocations where volar plate arthroplasty is insufficient, the hemi-hamate osteoarticular autograft represents the pinnacle of advanced reconstructive hand surgery.
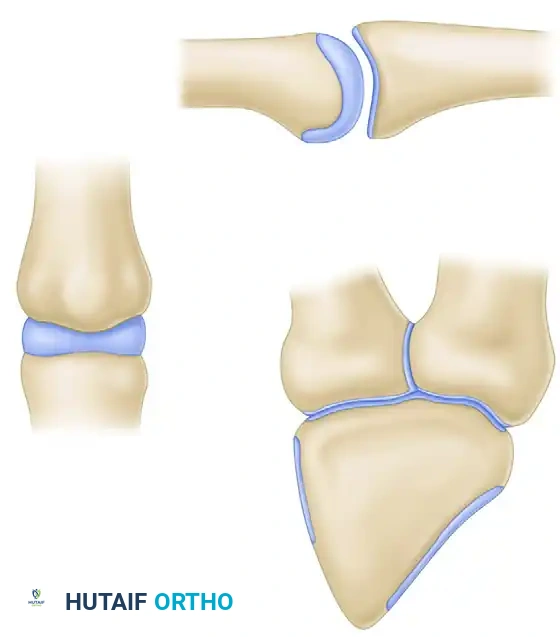
Biomechanical Rationale: The distal articular surface of the hamate (which articulates with the 4th and 5th metacarpal bases) features a central longitudinal ridge. This ridge perfectly mimics the median ridge of the volar base of the middle phalanx. By harvesting a size-matched graft from the hamate, the surgeon restores not only the volar buttress to prevent dorsal subluxation but also the crucial coronal plane stability provided by the median ridge.

Figure 67-49A: Persistent dorsal PIP joint subluxation with a nonreconstructible middle phalangeal volar lip fracture.
Step-by-Step Hemi-Hamate Surgical Technique:
1. Volar Approach: A volar Bruner zigzag incision exposes the PIP joint. The flexor tendon sheath is incised, and the A3 pulley is released to retract the flexor tendons laterally, protecting the neurovascular bundles.
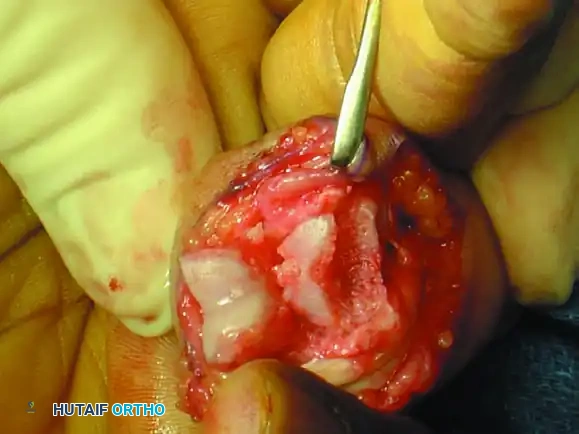
2. Joint Exposure ("Shotgunning"): The volar plate is sharply detached distally. The collateral ligaments are released from their proximal origins on the proximal phalanx. This allows the PIP joint to be hyperextended or "shotgunned," providing a 180-degree panoramic view of the articular defect.
3. Defect Preparation: The comminuted volar lip fragments are excised. The defect on the middle phalanx is squared off using a micro-oscillating saw or high-speed burr to create a geometrically precise recipient bed.
4. Graft Harvest: A separate dorsal longitudinal incision is made over the 4th/5th carpometacarpal (CMC) joints. The distal hamate is exposed. Using the dimensions measured from the recipient bed, a corresponding osteoarticular graft is harvested from the dorsal half of the distal hamate articular surface.
5. Graft Contouring and Fixation: The graft is meticulously contoured to fit the recipient bed perfectly. It is then press-fit into the middle phalanx and rigidly secured using two 1.0 mm or 1.3 mm minifragment lag screws inserted from volar to dorsal.
6. Closure and Assessment: The joint is reduced, and fluoroscopy confirms concentric reduction throughout a full arc of motion. The collateral ligaments and volar plate are repaired, and the incisions are closed.

Figure 67-49B: Volar exposure of the middle phalangeal base and geometrical preparation of the defect to receive the graft.

Figure 67-49C: Intraoperative fluoroscopic view of the distal hamate donor site.

Figure 67-49D: Fixation of the hemi-hamate graft with two minifragment screws to replicate the middle phalangeal base concavity.

Figure 67-49E: Radiograph demonstrating a concentric joint without collapse or dorsal subluxation at 2 years after surgery.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications following the operative management of phalangeal fractures remain frustratingly common, primarily due to the unforgiving anatomy of the hand. The most ubiquitous complication is postoperative stiffness. The close proximity of the fracture hematoma, periosteal stripping, and surgical implants to the delicate gliding planes of the extensor and flexor mechanisms invariably leads to dense fibrotic adhesions.
Stiffness occurs in up to 30-50% of operatively treated phalangeal fractures, particularly those requiring extensive dorsal exposures. Prevention is paramount, emphasizing rigid internal fixation that permits immediate, aggressive early active motion. When stiffness becomes refractory to specialized hand therapy, salvage management involves surgical tenolysis (freeing the tendons from scar tissue) and capsulotomy, typically performed 6 to 9 months post-injury once the fracture is solidly united and the soft tissue envelope has reached maximal medical improvement.
Infection and hardware failure are less common but devastating when they occur. Pin tract infections in CRPP are seen in approximately 5-10% of cases and usually resolve with oral antibiotics and early pin removal. Deep infections following ORIF
Clinical & Radiographic Imaging Archive