Comprehensive Introduction and Patho-Epidemiology
The management of a neglected or chronic Achilles tendon rupture represents a formidable reconstructive challenge, demanding a high level of surgical acumen and a profound understanding of lower extremity biomechanics. A rupture is classically defined as "neglected" or "chronic" when the presentation or diagnosis is delayed for more than four to six weeks following the initial traumatic event. Unlike acute ruptures, where the tendon ends are highly cellular, compliant, and amenable to primary end-to-end approximation with minimal resting tension, neglected ruptures are defined by a complex cascade of detrimental pathoanatomical changes. These include significant proximal retraction of the triceps surae complex, extensive interposition of disorganized fibrotic scar tissue (the "pseudotendon"), and progressive fatty infiltration with concomitant atrophy of the gastrocnemius-soleus muscle belly.
Epidemiologically, the incidence of missed acute Achilles tendon ruptures is alarmingly high, with literature suggesting that up to 20% to 25% of acute ruptures are misdiagnosed at the initial presentation. This diagnostic failure frequently occurs in primary care or emergency department settings, where the presence of active plantar flexion—facilitated by the intact tibialis posterior, flexor hallucis longus (FHL), flexor digitorum longus (FDL), and peroneals—masks the profound functional deficit of the triceps surae. Patients typically present weeks or months later complaining of intractable weakness, an inability to perform a single-leg heel raise, a noticeable gait asymmetry (calcaneus gait), and chronic fatigue in the affected extremity. The classic demographic profile mirrors that of acute ruptures, predominantly affecting men in their fourth to sixth decades of life, often "weekend warriors" engaging in episodic, high-intensity sports that require explosive acceleration or sudden eccentric loading.
The pathophysiology of the neglected rupture is characterized by a failed healing response. Following the initial mechanical failure, the tendon ends retract, leaving a hematoma within the paratenon sheath. Over time, this hematoma organizes into a dense, fibrovascular scar tissue bridge. While this pseudotendon provides some structural continuity, it is composed predominantly of mechanically inferior Type III collagen, lacking the highly organized, parallel Type I collagen bundles necessary to transmit the immense forces generated during the terminal stance phase of gait. Furthermore, the loss of normal physiological resting tension initiates a rapid process of disuse atrophy within the muscle belly. This is accompanied by irreversible fatty infiltration, analogous to the Goutallier changes observed in chronic rotator cuff tears, which severely compromises the excursion and force-generating capacity of the musculotendinous unit.
Attempting a primary end-to-end repair in the setting of a neglected rupture is frequently impossible and universally ill-advised. Forcing an approximation under excessive tension invariably leads to catastrophic complications, including severe equinus contracture, profound wound breakdown due to skin edge ischemia, and highly probable mechanical failure or re-rupture. Consequently, bridging the defect requires advanced reconstructive techniques, such as fascial turn-down flaps or V-Y tendinous advancements. The primary goals of surgical intervention are to meticulously resect the non-viable pseudotendon, bridge the resulting fibrotic gap with viable autogenous tissue, restore the anatomical length-tension relationship of the musculotendinous unit, and ultimately restore the patient's plantar flexion power to facilitate normal gait biomechanics.
Detailed Surgical Anatomy and Biomechanics
A masterful command of the surgical anatomy of the posterior leg is an absolute prerequisite for executing complex Achilles tendon reconstructions. The Achilles tendon is the largest and strongest tendon in the human body, formed by the confluence of the gastrocnemius and soleus aponeuroses. The gastrocnemius, a biarticular muscle originating from the posterior femoral condyles, merges with the monoarticular soleus, which originates from the posterior tibia and fibula. The tendinous fibers undergo a complex 90-degree lateral rotation as they descend toward their insertion on the posterior calcaneal tuberosity. This spiraling architecture is critical for the tendon's biomechanical properties, allowing for elastic energy storage and dynamic recoil during locomotion. The median raphe of the gastrocnemius aponeurosis, a central longitudinal thickening, serves as the primary donor site for the Bosworth turn-down flap and must be carefully identified during proximal dissection.
The vascular supply to the Achilles tendon is notoriously tenuous, a factor that plays a central role in both its susceptibility to rupture and the high rate of postoperative wound complications. The tendon receives its blood supply from three primary sources: the musculotendinous junction proximally, the osseotendinous junction distally, and the extrinsic vascular network supplied via the paratenon. The paratenon, a thin, highly vascularized sheath of loose areolar connective tissue, functions as a mesotenon, carrying vessels derived primarily from the posterior tibial artery. Angiographic studies have consistently demonstrated a relative hypovascular zone—the "watershed area"—located approximately 2 to 6 centimeters proximal to the calcaneal insertion. This zone correlates precisely with the most frequent site of spontaneous rupture and dictates that surgical dissection must meticulously preserve the anterior paratenon and avoid circumferential stripping of the tendon.
Biomechanically, the triceps surae complex is responsible for generating up to 80% of the total plantar flexion torque required during the push-off phase of the gait cycle. The length-tension relationship of this complex is exquisitely sensitive; even minor alterations in tendon length can result in profound functional deficits. Experimental models have demonstrated that a mere 1-centimeter over-lengthening of the Achilles tendon can result in a disproportionate loss of peak plantar flexion power, leading to a persistent calcaneus gait and the inability to perform a single-leg heel raise. Therefore, intraoperative tensioning is arguably the most critical step of the reconstructive procedure. The surgeon must aim to recreate the physiological resting tension, often assessed by comparing the resting equinus of the operative ankle to the contralateral side while the knee is flexed at 90 degrees (the Matles test position).
The neuroanatomy of the posterior leg is dominated by the sural nerve, which is highly vulnerable during surgical approaches to the Achilles tendon, particularly those involving lateral or extensive proximal extensions. The sural nerve is formed by the confluence of the medial sural cutaneous nerve (a branch of the tibial nerve) and the lateral sural cutaneous nerve (a branch of the common peroneal nerve). It typically courses distally along the posterolateral aspect of the calf, crossing the lateral border of the Achilles tendon approximately 9.8 centimeters proximal to its calcaneal insertion. During a lazy "S" incision or the proximal harvest of a gastrocnemius flap, the nerve must be definitively identified, isolated with a vessel loop, and gently retracted to prevent inadvertent transection or entrapment in scar tissue, which can lead to debilitating chronic regional pain syndrome (CRPS) or painful neuromas.
Exhaustive Indications and Contraindications
The decision to proceed with operative reconstruction of a neglected Achilles tendon rupture requires a nuanced assessment of the patient's physiological status, functional demands, and local tissue quality. Surgical intervention is generally indicated for patients who present with a chronic rupture (greater than 4-6 weeks post-injury) and demonstrate a profound loss of plantar flexion power, inability to perform a single-leg heel raise, and a debilitating gait asymmetry. Preoperative magnetic resonance imaging (MRI) is indispensable in quantifying the exact gap length (measured with the ankle in neutral dorsiflexion), assessing the degree of fatty infiltration in the muscle belly, and determining the viability of the remaining distal stump. The specific reconstructive technique is largely dictated by the size of the defect remaining after meticulous debridement of the pseudotendon.
Contraindications to surgical reconstruction must be rigorously respected, as the posterior ankle is highly unforgiving of complications. Absolute contraindications include active local or systemic infection, severe peripheral arterial disease (PAD) with compromised distal perfusion, and profound medical comorbidities that preclude safe anesthesia. Relative contraindications include poorly controlled diabetes mellitus, chronic systemic corticosteroid use, active tobacco smoking, and severe peripheral neuropathy. In patients with profound fatty infiltration of the triceps surae (Goutallier stage 3 or 4), the muscle's force-generating capacity may be irreversibly lost. In such cases, isolated bridging of the defect will fail to restore function, and a tendon transfer (e.g., FHL transfer) must be performed concomitantly or as the primary procedure to introduce a new, functional motor unit.
Surgical Decision-Making Matrix based on Defect Size
| Defect Size (Post-Debridement) | Recommended Surgical Technique | Rationale / Biomechanical Advantage |
|---|---|---|
| < 1 cm | Primary Repair +/- Augmentation | Rare in chronic cases; possible if minimal retraction. May require fractional lengthening. |
| 1 cm to 3 cm | V-Y Advancement (Abraham & Pankovich) | Maintains broad insertion of aponeurosis; preserves muscle force-generating capacity. |
| 3 cm to 6 cm | Bosworth Turn-Down Flap or FHL Transfer | Bridges large gaps with autogenous scaffold; FHL adds active motor unit if muscle is atrophied. |
| > 6 cm | FHL Transfer + Allograft / Synthetic Mesh | Massive defects require structural allograft (e.g., Achilles with bone block) and motor replacement. |
The patient's functional expectations must be carefully managed during the preoperative consultation. While reconstructive surgery reliably restores anatomical continuity and improves gait mechanics, patients must be counseled that the reconstructed tendon will never regain the precise histological structure or absolute peak biomechanical strength of the native, uninjured tendon. A mild, persistent deficit in peak explosive power is common, and the rehabilitation process is protracted, often requiring 9 to 12 months before maximal medical improvement is achieved. Furthermore, the risk profile for chronic reconstructions is significantly higher than that of acute repairs, necessitating strict adherence to postoperative protocols.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful neglected Achilles tendon reconstruction. The clinical examination must include a comprehensive assessment of the soft tissue envelope. The posterior skin is meticulously inspected for trophic changes, prior surgical scars, and signs of vascular insufficiency. The Thompson test (calf squeeze test) will invariably be positive, though a palpable gap may be obscured by the hypertrophic pseudotendon. A comprehensive neurovascular examination is mandatory, documenting baseline sensation in the sural and tibial nerve distributions, as well as the presence of palpable dorsalis pedis and posterior tibial pulses. If vascular compromise is suspected, formal non-invasive arterial studies (Ankle-Brachial Index, arterial duplex) should be obtained prior to surgical clearance.
Advanced imaging is non-negotiable in the workup of a chronic rupture. High-resolution MRI without contrast is the gold standard. Sagittal T1-weighted sequences are critical for evaluating the degree of fatty infiltration within the soleus and gastrocnemius muscle bellies, which directly influences the decision to perform a concomitant FHL transfer. Sagittal T2-weighted or STIR sequences are utilized to accurately measure the gap between the viable tendon ends. It is imperative that the radiologist measures this gap with the ankle positioned in neutral (0 degrees of dorsiflexion), as plantar flexion will artificially underestimate the defect size. The surgeon must template the anticipated flap dimensions based on these measurements, ensuring that a V-Y advancement will have sufficient proximal aponeurosis for a 1.5x length ratio, or that a Bosworth flap can be harvested with adequate length to traverse the defect and fold back upon itself.
Patient Positioning and Operating Room Setup
The patient is brought to the operating theater and positioned prone on a radiolucent operating table. Meticulous attention to positioning is required to prevent pressure-induced neuropathies and ensure adequate pulmonary excursion. Chest rolls or a specialized prone frame (e.g., Jackson table with chest/pelvic pads) should be utilized to allow the abdomen to hang free, thereby reducing inferior vena cava compression and minimizing epidural venous engorgement. The arms are typically positioned on padded armboards with the shoulders abducted less than 90 degrees to protect the brachial plexus. All bony prominences, particularly the patellae and the anterior superior iliac spines, must be heavily padded.
Crucially, the patient's knees should be positioned just distal to the break in the operating table. This allows the surgeon to flex the knee to 90 degrees intraoperatively, which is an absolute necessity for assessing the resting tension of the musculotendinous unit (the intraoperative Matles test). General anesthesia or regional neuraxial anesthesia (spinal/epidural) is employed based on patient comorbidities and anesthesiologist preference. A well-padded pneumatic tourniquet is applied to the proximal thigh. Prior to tourniquet inflation, exsanguination of the limb is performed using an Esmarch bandage to ensure a completely bloodless surgical field. This avascular field is critical for identifying the delicate sural nerve and distinguishing between viable, glistening tendon tissue and the disorganized, fibrotic pseudotendon. The entire lower extremity, from the mid-thigh to the tips of the toes, is prepped and draped in a standard sterile fashion. The foot must remain completely free within the sterile field to allow the surgeon to manipulate the ankle through a full, unrestricted range of motion.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach for a neglected Achilles tendon rupture demands meticulous soft tissue handling to preserve the tenuous vascularity of the posterior skin flaps. A posterior longitudinal midline incision, or a lazy "S" incision, is utilized depending on the planned reconstructive technique. The lazy "S" incision is often preferred as it avoids placing a straight scar directly over the tendon, thereby reducing the risk of scar contracture and skin adherence. The incision extends from the calcaneal tuberosity distally to the proximal one-third of the calf. The dissection must proceed straight down through the subcutaneous tissue to the deep fascia, creating full-thickness fasciocutaneous flaps. Undermining the skin or creating thin flaps will inevitably lead to ischemic necrosis and catastrophic wound breakdown.
Upon identifying the deep fascia, it is incised longitudinally in line with the skin incision. The paratenon, which is often thickened and adherent to the underlying pseudotendon, must be carefully incised and reflected as a separate layer. Preservation of the paratenon is paramount; it will be required for closure to provide a gliding surface and restore extrinsic vascularity to the healing reconstruction. Once the paratenon is reflected, the pseudotendon is exposed. Using sharp dissection, the surgeon meticulously excises the interposed fibrotic scar tissue. Inadequate resection of this scar tissue is a common pitfall; the surgeon must resect proximally and distally until healthy, organized, glistening parallel tendon fibers are encountered, even if this significantly increases the measured size of the defect.
Direct Repair of Neglected Ruptures: The Bosworth Technique
The Bosworth technique is a highly reliable reconstructive option for defects greater than 3 cm. It utilizes a central strip of the gastrocnemius aponeurosis, left attached proximally, which is turned down and woven through the ruptured tendon ends to provide both a biological scaffold and mechanical strength.
- Flap Harvest: Expose the proximal gastrocnemius aponeurosis and identify the median raphe. Free a central strip of tendon from the median raphe, precisely 1.5 cm wide and 17.5 to 22.5 cm long. Crucially, leave the strip attached just proximal to the site of the rupture to preserve its vascular tether and biomechanical anchor point.
- Proximal Pass: Turn the harvested fascial strip distally.

Pass it transversely through the center of the proximal tendon stump. Anchor it at this entry point with a heavy absorbable suture (e.g., #1 Vicryl or PDS) to prevent proximal propagation of the split under tension.
3. Distal Weave: Pass the strip distally across the defect and then transversely through the distal calcaneal stump.
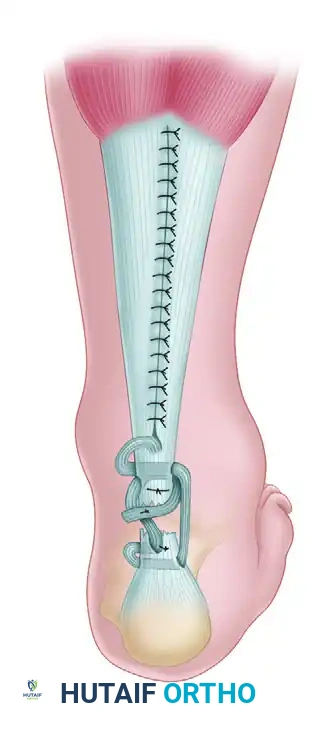
Pass the strip again through the distal stump, directing it from anterior to posterior to create a locking configuration that resists pull-out.
4. Tensioning: While an assistant holds the knee at 90 degrees of flexion and the ankle in 20 degrees of plantar flexion, draw the fascial strip tight. Anchor the strip to the distal stump using heavy nonabsorbable sutures.
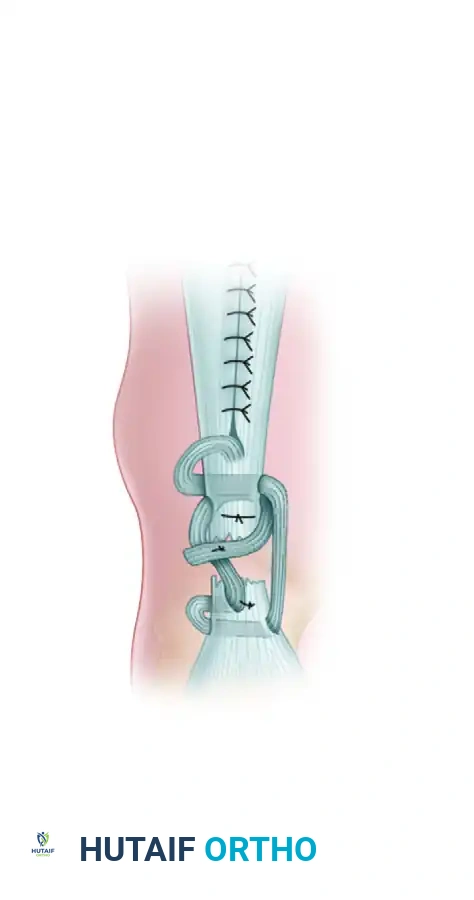
- Final Proximal Pass: Bring the remaining tail of the strip proximally across the defect, pass it transversely through the proximal stump, and suture it securely onto itself, creating a robust, multi-stranded bridge. The proximal harvest defect is closed side-to-side.
Direct Repair of Neglected Ruptures: Abraham and Pankovich (V-Y Advancement)
The Abraham and Pankovich technique is indicated when 1 to 3 cm of tendon must be resected. It relies on the proximal mobilization of the gastrocnemius aponeurosis to bridge the defect without sacrificing structural continuity.
- Measurement and V-Incision: After defect preparation, position the knee in 30 degrees of flexion and the ankle in 20 degrees of plantar flexion. Measure the exact length of the tendon defect. Move proximally to the gastrocnemius aponeurosis and make an inverted-V incision through the aponeurosis. The apex is positioned centrally and proximally. The arms of the V-incision must be at least 1.5 times longer than the measured tendon defect to allow for adequate distal excursion.
- Advancement and Approximation: Pull the mobilized aponeurotic flap distally. Approximate the ends of the ruptured tendon. Secure the repair using a core suture technique, such as a locking Krackow or Kessler stitch, utilizing heavy, interrupted nonabsorbable sutures (e.g., #2 FiberWire or Ethibond). Ensure the tension perfectly mimics the contralateral resting equinus.
- Proximal Y-Closure: Return to the proximal aponeurosis. Close the proximal part of the inverted-V incision in a Y configuration using interrupted sutures. This secures the lengthened aponeurosis in its new, advanced position, maintaining the broad insertion of the muscle fibers.
Regardless of the technique utilized, the closure must be executed with obsessive attention to detail. The paratenon is closed circumferentially over the repair site with fine absorbable sutures (e.g., 3-0 Vicryl) to prevent skin adherence and optimize vascular ingrowth. The deep fascia and subcutaneous tissues are closed in layers. Skin closure should be performed with non-absorbable monofilament (e.g., 3-0 Nylon) using a vertical mattress technique to minimize skin edge ischemia and evert the wound edges.
Complications, Incidence Rates, and Salvage Management
Reconstruction of neglected Achilles tendon ruptures carries a significantly higher complication profile compared to acute repairs. The compromised local biology, extensive surgical dissection, and the inherent tension required to restore biomechanical function create a precarious environment for wound healing and tendon incorporation. Surgeons undertaking these procedures must be hyper-vigilant in their preoperative optimization, intraoperative tissue handling, and postoperative surveillance. The most devastating complications involve the soft tissue envelope, as the posterior ankle has a tenuous blood supply that is easily compromised by excessive tension, aggressive retraction, or underlying microvascular disease.
Wound breakdown and deep surgical site infections (SSIs) are the most feared early complications. Superficial wound dehiscence may be managed with local wound care, oral antibiotics, and temporary cessation of rehabilitation protocols. However, deep infections involving the reconstructed tendon or exposed allograft require aggressive, immediate intervention. This includes formal operative irrigation and debridement, targeted intravenous antibiotic therapy, and often the application of negative pressure wound therapy (NPWT). If the tendon is exposed and the soft tissue defect cannot be closed primarily, local rotational flaps (e.g., reverse sural artery flap) or free tissue transfer (e.g., anterolateral thigh free flap) performed in conjunction with a microvascular plastic surgeon become mandatory to salvage the limb and the reconstruction.
Common Complications in Chronic Achilles Reconstruction
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Wound Dehiscence / Necrosis | 5% - 15% | Thin skin flaps, excessive resting tension, smoking, diabetes. | Local wound care, NPWT, reverse sural artery flap, free tissue transfer. |
| Deep Infection | 2% - 5% | Prolonged operative time, hematoma, compromised host immunity. | Aggressive serial I&D, IV antibiotics, hardware/suture removal if necessary. |
| Sural Nerve Injury | 3% - 10% | Iatrogenic transection or entrapment during lateral dissection. | Gabapentinoids, nerve blocks; surgical exploration and neuroma excision if refractory. |
| Over-lengthening (Weakness) | 10% - 20% | Inadequate intraoperative tensioning, premature weight-bearing. | Orthotic management (AFO); revision surgery with FHL transfer if profoundly debilitating. |
| Re-rupture | 2% - 6% | Patient non-compliance, aggressive early dorsiflexion, poor tissue quality. | Revision reconstruction, often requiring structural allograft augmentation or FHL transfer. |
| VTE (DVT / PE) | 1% - 5% | Prolonged immobilization, prone positioning, tourniquet use. | Chemical prophylaxis (LMWH, DOACs) based on risk stratification; therapeutic anticoagulation if diagnosed. |
Sural nerve injury is a highly morbid complication that can result in chronic lateral foot numbness or debilitating neuropathic pain. As previously detailed, the nerve is at high risk during the lateral limb of a lazy "S" incision and during the proximal harvest of the gastrocnemius aponeurosis. Meticulous blunt dissection and the use of vessel loops for gentle retraction are critical. If a neuroma forms postoperatively, it may require surgical excision and burying of the proximal nerve stump into deep muscle tissue.
Biomechanical failure, specifically over-lengthening, is a silent but profound complication. If the surgeon fails to adequately tension the Bosworth weave or the V-Y advancement, or if the patient is non-compliant with early immobilization, the reconstruction will heal in an elongated position. This results in permanent push-off weakness, a persistent calcaneus gait, and an inability to perform high-demand activities. Salvage of an over-lengthened reconstruction is exceedingly difficult and typically requires a revision procedure utilizing a flexor hallucis longus (FHL) tendon transfer to introduce a new, properly tensioned motor unit to the calcaneus.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a neglected Achilles tendon reconstruction is a delicate balancing act between protecting the fragile biological repair and preventing deleterious joint contractures and profound muscle atrophy. The protocol is inherently more conservative and protracted than that utilized for acute ruptures, reflecting the extensive nature of the reconstruction and the compromised quality of the host tissues. The rehabilitation process is generally divided into four distinct phases: strict immobilization, protected progressive weight-bearing, active strengthening, and return to high-demand function. Communication between the operating surgeon and the physical therapist is paramount to ensure the patient does not advance through the phases prematurely.
Phase I: Strict Immobilization (Weeks 0 to 4-6)
Immediately following surgery, the patient is placed in a well-padded, rigid long-leg cast or a highly reinforced posterior splint. The knee is immobilized in 30 to 45 degrees of flexion, and the ankle is positioned in gravity equinus (approximately 20 to 30 degrees of plantar flexion). This position maximizes the relaxation of the gastrocnemius-soleus complex, completely eliminating tension on the repair site. The patient is strictly non-weight-bearing on the operative extremity and must utilize crutches or a knee scooter. Elevation of the limb above the level of the heart is critical during the first two weeks to mitigate postoperative edema and protect the vascularity of the healing skin flaps.
Phase II: Protected Progressive Weight-Bearing (Weeks 6 to 10)
Once early biological healing is established and the surgical incisions are fully consolidated, the long-leg cast is removed. The patient is transitioned to a short-leg cast or a rigid controlled ankle motion (CAM) walker boot. Crucially, the boot must be fitted with a substantial heel lift (typically 3 to 5 centimeters, or multiple wedge inserts) to maintain the ankle in plantar flexion. The patient is allowed to begin partial, protected weight-bearing with crutches, progressively advancing to full weight-bearing as tolerated within the boot. Over the subsequent 4 weeks, the heel wedges are systematically removed (e.g., one wedge every 1-2 weeks) to gradually bring the ankle toward a neutral position. Active plantar flexion and gentle, active-assisted dorsiflexion to neutral are initiated, but passive stretching into dorsiflexion remains strictly contraindicated.
Phase III: Active Strengthening and Proprioception (Months 2.5 to 4)
At approximately 10 to 12 weeks postoperatively, the CAM boot is discontinued, and the patient transitions to standard supportive footwear, often utilizing a small, 1-centimeter silicone heel lift for an additional month to prevent sudden micro-trauma. Formal physical therapy intensifies, focusing on concentric and eccentric strengthening of the triceps surae. Exercises progress from double-leg heel raises to single-leg heel raises. Proprioceptive training utilizing balance boards and unstable surfaces is critical to restore neuromuscular control. Stationary cycling and aquatic therapy are excellent adjuncts during this phase to improve cardiovascular fitness and joint mobility without subjecting the tendon to excessive impact loading.
Phase IV: Return to Function and Sport (Months 5 to 12+)
The final phase of rehabilitation is highly individualized and depends on the patient's baseline athletic demands. Introduction of low-impact plyometrics, jogging, and sport-specific agility drills begins only when the patient demonstrates symmetrical ankle range of motion, normal gait mechanics without a limp, and the ability to perform repetitive single-leg heel raises without pain or fatigue. Patients must be extensively counseled that maximal medical improvement, particularly regarding explosive push-off power and calf muscle hypertrophy, may not be realized until 12 to 18 months postoperatively.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of neglected Achilles tendon ruptures is supported by a robust body of historical literature and evolving modern clinical guidelines. The foundational techniques utilized today were pioneered in the mid-20th century. David M. Bosworth first described his eponymous technique in 1956, recognizing the necessity of utilizing autogenous tissue to bridge large defects. His original paper eloquently detailed the biomechanical advantages of leaving the fascial strip attached proximally, a principle that remains the gold standard for large-gap reconstructions. Similarly, in 1975, Abraham and Pankovich published their landmark study describing the V-Y tendinous advancement flap. They provided the critical mathematical ratio—that the V-incision must be 1.5 times the length of the defect—which continues to dictate surgical templating for medium-sized gaps.
Modern literature has increasingly focused on the integration of tendon transfers, specifically the flexor hallucis longus (FHL), in the management of chronic ruptures. Wapner et al. (1993) popularized the FHL transfer, demonstrating its utility not only as a structural bridge but, more importantly, as an active, in-phase motor unit capable of compensating for severe triceps surae atrophy. Recent systematic reviews and meta-analyses comparing direct reconstructive techniques (Bosworth, V-Y) to FHL transfers suggest that while V-Y advancement provides excellent outcomes for gaps under 3-4 cm with viable muscle, FHL transfer is superior in patients with massive gaps, profound fatty infiltration (Goutallier 3/4), or revision scenarios.
Clinical guidelines from major orthopaedic societies, including the American Academy of Orthopaedic Surgeons (AAOS), emphasize that the treatment of chronic ruptures must be highly individualized. While there is strong consensus against attempting primary end-to-end repair under tension, the choice between V-Y advancement, turn-down flaps, and tendon transfers remains surgeon-dependent, guided by intraoperative findings and defect measurements. Furthermore, recent literature strongly advocates for the use of preoperative MRI not just for gap measurement, but for qualitative assessment of the muscle belly, moving the paradigm from purely structural reconstruction to functional, motor-unit-preserving surgery. Mastery of these historical principles and modern advancements is essential for the orthopaedic surgeon navigating the complex landscape of neglected Achilles tendon ruptures.
This academic synthesis is based on established protocols from Hutaifortho's Operative Orthopaedics and has been medically reviewed by Prof. Dr. Mohammed Hutaif, Consultant Orthopedic & Spine Surgeon. It is designed to assist orthopedic residents, fellows, and practicing surgeons in surgical preparation and board reviews (AAOS, FRCS, Arab Board).
