Comprehensive Introduction and Patho-Epidemiology
Neglected, or chronic, ruptures of the Achilles tendon present one of the most formidable reconstructive challenges in foot and ankle surgery. While acute ruptures are typically diagnosed and managed within the first few weeks of injury, neglected ruptures are universally defined in the orthopedic literature as those presenting more than four to six weeks post-injury. The true incidence of missed acute Achilles tendon ruptures is alarmingly high, with estimates suggesting that up to 20% to 25% of all acute ruptures are initially misdiagnosed by primary care physicians or emergency department personnel. This diagnostic failure often stems from the masking effect of profound localized edema, the preservation of weak plantarflexion through accessory flexors (e.g., tibialis posterior, flexor hallucis longus, flexor digitorum longus, and peroneals), and the absence of a distinct, palpable gap due to hematoma accumulation.
The pathomechanics of a neglected rupture are fundamentally distinct from those of an acute injury, characterized by a progressive, deleterious cascade of anatomical and histological alterations. Following the initial rupture, the unopposed proximal gastrocnemius-soleus complex undergoes significant proximal retraction. Over a period of weeks to months, this retracted muscle belly experiences disuse atrophy and irreversible fatty infiltration, severely compromising its contractile excursion and force-generating capacity. Concurrently, the void between the retracted proximal stump and the distal calcaneal insertion becomes occupied by an organized hematoma that gradually fibroses into a non-functional, disorganized scar tissue bridge, universally referred to as the "pseudotendon."
Histologically, the native Achilles tendon is composed predominantly of highly organized, parallel bundles of type I collagen, which confer exceptional tensile strength and elasticity. In stark contrast, the pseudotendon is composed primarily of type III collagen, characterized by a haphazard, multidirectional fiber orientation, hypercellularity, and an abundance of ground substance. This disorganized fibrovascular scar lacks the biomechanical integrity necessary to transmit the massive forces generated by the triceps surae during the push-off phase of the gait cycle. Consequently, the pseudotendon elongates under physiological loads, leading to a functional lengthening of the musculotendinous unit.
Clinically, this elongation manifests as a profound mechanical disadvantage. Patients invariably present with significant weakness in terminal plantarflexion, an absolute inability to perform a single-leg heel raise, a noticeable limp, and an energy-inefficient, calcaneal gait pattern. The primary surgical objective in managing these complex injuries is not merely to bridge the anatomical defect, but to meticulously restore the physiological resting length and tension of the musculotendinous unit. By re-establishing this critical length-tension relationship, the surgeon restores the biomechanical advantage of the triceps surae, thereby enabling a return to functional ambulation and, in selected cases, athletic participation.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy of the posterior leg and hindfoot is an absolute prerequisite for executing complex Achilles tendon reconstructions. The Achilles tendon, the largest and strongest tendon in the human body, represents the confluent tendinous insertion of the gastrocnemius and soleus muscles. The gastrocnemius, a biarticular muscle originating from the posterior femoral condyles, is primarily responsible for explosive plantarflexion and is highly active during knee extension. The soleus, a monoarticular muscle originating from the posterior tibia and fibula, serves as the primary postural stabilizer and generates sustained plantarflexion force independent of knee position. As these tendinous aponeuroses merge to form the Achilles tendon, the fibers undergo a distinct 90-degree internal rotation, such that the gastrocnemius fibers insert on the posterolateral aspect of the calcaneal tuberosity, while the soleus fibers insert on the posteromedial aspect.
The vascular supply to the Achilles tendon is notoriously tenuous and represents a critical consideration in both the pathogenesis of ruptures and the planning of surgical incisions. The tendon lacks a true synovial sheath; instead, it is enveloped by a highly vascularized paratenon composed of visceral and parietal layers. The blood supply is derived from three primary sources: the musculotendinous junction proximally, the osseotendinous junction distally, and the extrinsic segmental vessels traversing the paratenon via the mesotenon anteriorly. Microangiographic studies have consistently identified a relative watershed area of hypovascularity located approximately 2 to 6 centimeters proximal to the calcaneal insertion. This zone correlates precisely with the most common site of both acute ruptures and degenerative tendinopathy, and it demands meticulous preservation of the anterior paratenon and Kager's fat pad during surgical dissection.
The sural nerve, a purely sensory branch formed by the confluence of the medial sural cutaneous nerve and the sural communicating branch, is the most vulnerable neurovascular structure during Achilles tendon surgery. The nerve courses distally along the posterolateral aspect of the calf, intimately associated with the small saphenous vein. It typically crosses the lateral border of the Achilles tendon at an average distance of 9.8 centimeters (range, 7 to 12 cm) proximal to the calcaneal insertion. From this crossing point, it descends along the lateral border of the tendon to provide sensation to the lateral hindfoot and midfoot. Surgical approaches, particularly posterolateral incisions or percutaneous suturing techniques, must be meticulously planned and executed with direct visualization to avoid iatrogenic injury, which can result in debilitating neuromas or profound lateral foot numbness.
Biomechanically, the triceps surae is responsible for generating up to 80% of the total plantarflexion torque required for normal ambulation. During the terminal stance phase of the gait cycle, the Achilles tendon must withstand forces equivalent to 3 to 4 times body weight during walking, and up to 10 to 12 times body weight during running or jumping. In the setting of a neglected rupture, the interposition of the compliant pseudotendon alters the lever arm of the ankle joint. The functional lengthening of the tendon shifts the muscle's operating range to the descending limb of the Blix length-tension curve, drastically reducing its force output. Tendon transfer techniques, such as the peroneus brevis or flexor hallucis longus (FHL) transfer, aim to bypass this compromised unit by introducing a healthy, vascularized, in-phase (or phase-convertible) muscle to restore active plantarflexion and reinforce the deficient posterior soft-tissue envelope.
Exhaustive Indications and Contraindications
The decision-making process for the operative management of neglected Achilles tendon ruptures is highly nuanced and must be individualized based on patient age, functional demands, medical comorbidities, and the precise anatomical characteristics of the defect. Operative intervention is universally indicated for physiologically active patients who present with symptomatic weakness, an inability to perform a single-leg heel raise, and an altered gait pattern that interferes with their activities of daily living or occupational requirements. The ultimate surgical strategy is dictated by a strict algorithmic approach based on the intraoperative gap measured with the ankle in neutral dorsiflexion (0 degrees) after the complete excision of the fibrotic pseudotendon and maximal mobilization of the proximal muscle belly.
Contraindications to surgical reconstruction must be rigorously evaluated, as the complication profile for neglected ruptures is significantly higher than that of acute repairs. Absolute contraindications include active local or systemic infection, severe peripheral arterial disease (e.g., Ankle-Brachial Index < 0.5 or absent palpable pedal pulses without collateralization), and profound peripheral neuropathy (e.g., advanced Charcot neuroarthropathy or severe diabetic polyneuropathy) where the patient lacks protective sensation. Attempting extensive soft-tissue reconstruction in these environments invariably leads to catastrophic wound breakdown, deep infection, and potential amputation.
Relative contraindications require careful patient counseling and risk stratification. These include advanced physiological age with inherently low functional demands, where conservative management with an articulated Ankle-Foot Orthosis (AFO) may provide sufficient stability for household ambulation. Other relative contraindications include chronic uncontrolled diabetes mellitus (HbA1c > 8.0%), active tobacco use, chronic systemic corticosteroid use, and severe dermatological conditions affecting the posterior leg. In these high-risk populations, if surgery is deemed absolutely necessary, less invasive techniques or isolated tendon transfers without extensive posterior soft-tissue stripping should be considered to minimize wound complications.
Indications and Contraindications Matrix
| Parameter | Operative Reconstruction | Non-Operative Management (AFO / Bracing) |
|---|---|---|
| Patient Profile | Young to middle-aged, physiologically active, high functional demands. | Elderly, low-demand, sedentary lifestyle, or non-ambulatory status. |
| Clinical Presentation | Profound plantarflexion weakness, inability to perform single-leg heel raise, severe gait dysfunction. | Mild to moderate weakness well-tolerated by the patient, minimal gait interference. |
| Gap Size (Intra-op) | < 3 cm: Direct repair + mobilization. 3 - 6 cm: Local tendon transfer (Peroneus Brevis, FHL) or V-Y advancement. > 6 cm: Free tissue transfer, synthetic mesh, or complex local transfers. |
Irrelevant, as anatomical bridging is not surgically attempted. |
| Absolute Contraindications | Active infection, severe PAD (ABI < 0.5), severe peripheral neuropathy, inadequate soft-tissue envelope. | Patient refusal of bracing, skin breakdown over brace contact points. |
| Relative Contraindications | Uncontrolled diabetes (HbA1c > 8.0%), active smoking, systemic corticosteroid use, obesity (BMI > 40). | High athletic demands, occupations requiring climbing or heavy lifting. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative evaluation and precise surgical planning are the cornerstones of successful outcomes in chronic Achilles reconstruction. The clinical examination must systematically assess the resting tension of the Achilles tendon. The patient is evaluated in the prone position with the knees flexed to 90 degrees (the Matles test); in a neglected rupture, the affected foot will fall into neutral or dorsiflexion compared to the resting equinus of the contralateral, uninjured limb. The Thompson squeeze test remains positive, though it may be subtly masked by the presence of a thick pseudotendon. The palpable gap, a hallmark of acute ruptures, is frequently absent in chronic cases due to the dense fibrovascular scar tissue filling the defect.
Advanced imaging is mandatory for surgical templating. While weight-bearing plain radiographs are obtained to rule out calcaneal avulsion fractures, Haglund's deformity, and intratendinous calcifications, Magnetic Resonance Imaging (MRI) remains the gold standard. A dedicated non-contrast MRI of the ankle and lower leg accurately delineates the extent of tendon retraction, the precise length of the pseudotendon, and the quality of the remaining tendon stumps. Crucially, axial T1-weighted sequences must be evaluated to assess the degree of fatty infiltration and muscle atrophy within the gastrocnemius and soleus bellies. Severe fatty infiltration (analogous to high-grade Goutallier classifications in the rotator cuff) portends a poor functional prognosis for direct repair and strongly dictates the necessity of a dynamic tendon transfer (e.g., FHL or Peroneus Brevis) to introduce a new, contractile muscle unit.
Patient positioning and intraoperative setup require meticulous attention to detail. The patient is placed in the prone position on a radiolucent Jackson table or standard operating table with chest and pelvic rolls to ensure adequate pulmonary excursion and prevent abdominal compression. All bony prominences, particularly the ulnar nerves at the elbows and the anterior superior iliac spines, must be heavily padded. A thigh tourniquet is applied over generous padding. Crucially, both lower extremities must be prepped and draped into the sterile field. This bilateral exposure is non-negotiable, as it allows the surgeon to continuously compare the resting equinus tension of the reconstructed limb with that of the contralateral, normal limb during the final tensioning phase of the repair.
Surgical templating involves ensuring the availability of a comprehensive array of fixation devices and allografts. The surgical team must have immediate access to heavy non-absorbable sutures (e.g., #2 or #5 FiberWire, Orthocord, or Ethibond), tendon strippers for plantaris harvest, interference screws (ranging from 5.5 mm to 8.0 mm) for FHL or peroneus brevis calcaneal fixation, and suture anchors for supplementary distal fixation. In cases where preoperative MRI indicates a massive gap (> 6 cm), the surgeon must have Achilles tendon allograft, semitendinosus autograft/allograft, or synthetic acellular dermal matrices available on standby to augment the reconstruction.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution for neglected Achilles ruptures is highly variable and depends entirely on the intraoperative gap measurement after aggressive debridement. The following sections detail the specific techniques for direct repair, peroneus brevis transfer, and plantaris augmentation.
Direct Repair with Proximal Mobilization (Gap < 3 cm)
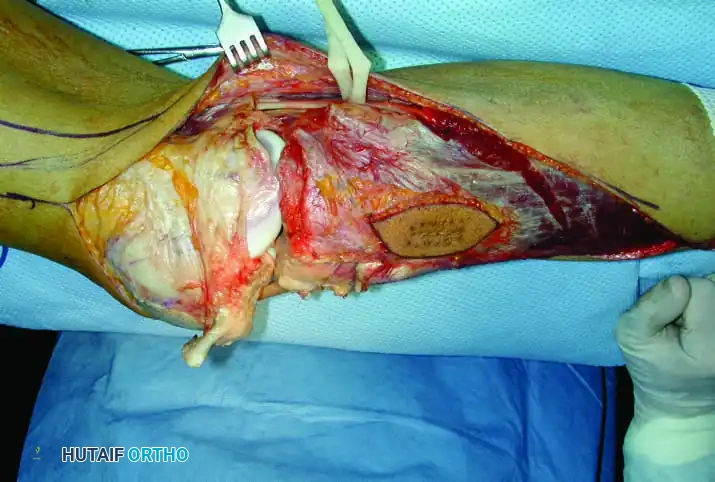
When the defect is relatively small, direct end-to-end repair can be achieved through aggressive proximal mobilization. A curvilinear posteromedial incision is utilized, typically beginning 2 to 3 cm distal to the calcaneal insertion and extending proximally as far as necessary. The posteromedial approach is strongly preferred over a midline incision to avoid creating a painful scar directly over the shoe-counter contact area, and to maximize the distance from the laterally coursing sural nerve. The incision is carried through the skin and subcutaneous tissue down to the paratenon. Meticulous preservation of the paratenon is critical; it must be incised longitudinally and reflected as full-thickness flaps to preserve its delicate vascular network.
The disorganized, grey, amorphous pseudotendon is identified and sharply excised. Debridement must continue proximally and distally until healthy, pearly-white tendon tissue with distinct longitudinal striations is encountered. Once the true gap is established, the ankle is placed in neutral dorsiflexion to assess the defect size. If the gap is under 3 cm, proximal mobilization is initiated. This involves releasing the myofascial adhesions tethering the gastrocnemius and soleus to the deep posterior compartment. Blunt finger dissection and careful sharp release of the soleal fascia can yield 1 to 2 cm of additional excursion. If further length is required, a fractional lengthening of the gastrocnemius aponeurosis (Baumann procedure) or a formal Strayer release can be performed proximally.
Once adequate length is achieved, the tendon stumps are approximated. Heavy, multi-strand, non-absorbable sutures (#2 or #5) are passed through the proximal and distal stumps utilizing a locked, grasping configuration, such as the Krackow or Giftbox technique. Typically, two to three locking loops are placed on each side of the repair. The ankle is then positioned in 20 to 30 degrees of plantarflexion (equinus) to match the resting tension of the contralateral limb, and the sutures are tied securely. The repair is visually inspected to ensure no gapping occurs during passive dorsiflexion to neutral.
Peroneus Brevis Transfer (White and Kraynick; Teuffer Modification)
For defects ranging from 3 to 6 cm, or in cases of severe triceps surae fatty infiltration, a local tendon transfer is indicated. The peroneus brevis transfer, originally described by White and Kraynick and later modified by Teuffer, provides a robust, vascularized, and dynamic reconstruction. A posterolateral longitudinal incision is utilized to expose both the Achilles defect and the lateral peroneal compartment simultaneously. The sural nerve is meticulously identified, neurolysed if necessary, and protected with a vessel loop throughout the procedure.
The peroneus brevis is harvested by making a small, 2 cm longitudinal incision over its insertion at the base of the fifth metatarsal. The tendon is sharply detached from the bone, taking care not to violate the cuboid articulation. Returning to the primary posterolateral incision, the lateral intermuscular septum is incised, and the peroneus brevis tendon is drawn proximally into the wound. It is imperative to ensure that the muscle belly of the peroneus brevis is adequately released from its fascial constraints to allow for maximum distal excursion without tethering.
The Teuffer modification involves creating a dynamic loop through the calcaneus. A transverse drill tunnel (typically 5.5 to 7.0 mm in diameter, depending on the graft size) is created through the calcaneal tuberosity. The tunnel must be placed anterior to the native Achilles insertion and strictly orthogonal to the sagittal plane to avoid violating the subtalar joint superiorly or causing a posterior cortical blowout. The peroneus brevis tendon is passed from lateral to medial through this osseous tunnel. It is then routed superiorly and sutured directly to the proximal stump of the Achilles tendon, as well as back onto itself, using multiple interrupted #2 non-absorbable sutures. This dynamic loop mechanically bridges the defect and directly transfers the contractile force of the peroneal muscle to the calcaneus.
Plantaris Tendon Augmentation (Technique 48-15)
To further reinforce a tenuous direct repair or augment a peroneus brevis transfer, the plantaris tendon can be utilized as a biological scaffold. The plantaris is present in approximately 90% of the population. It is identified medially, lying in the interval between the medial head of the gastrocnemius and the soleus. Its distal insertion on the medial aspect of the calcaneus is preserved. A closed, circular tendon stripper is passed over the proximal end of the tendon and advanced proximally into the calf until the musculotendinous junction is reached, allowing for the harvest of 20 to 30 cm of tendon.
The harvested proximal end of the plantaris is threaded onto a large, curved fascial needle. A figure-of-eight weave is then performed across the primary repair site. The needle is passed transversely through the proximal Achilles stump, crossed over the defect, and passed through the distal stump. This weaving process is repeated multiple times to create a robust biological cage around the primary repair. The remaining tail of the plantaris is fanned out, creating a broad, flat membrane that is tacked down over the repair site with fine absorbable sutures (e.g., 3-0 Vicryl). This not only provides immediate structural reinforcement but also introduces native tenocytes and a biological scaffold to promote rapid cellular ingrowth and revascularization.
Complications, Incidence Rates, and Salvage Management
The operative management of neglected Achilles tendon ruptures is fraught with potential complications, primarily due to the extensive soft-tissue dissection required and the inherently poor vascularity of the posterior ankle envelope. Surgeons must maintain a high index of suspicion and employ rigorous prophylactic measures to mitigate these risks. Wound healing complications are the most frequent and feared adverse events. The skin overlying the Achilles tendon is supplied by distinct angiosomes (primarily the peroneal and posterior tibial arteries), and extensive subcutaneous undermining can easily devascularize the skin flaps, leading to marginal necrosis, dehiscence, and deep space infection.
Sural nerve injury is a significant complication, particularly associated with posterolateral approaches and percutaneous suture passage. The incidence of transient neurapraxia or permanent sensory deficit can range from 3% to 10% in complex reconstructions. Intraoperative identification and protection are paramount. If a neuroma develops postoperatively, management ranges from conservative measures (gabapentinoids, targeted steroid injections) to surgical excision and burying of the nerve stump into the deep muscle belly of the flexor hallucis longus or soleus.
Re-rupture is a catastrophic failure of the reconstruction, occurring in 2% to 5% of cases. It is most frequently the result of patient non-compliance with the strict postoperative weight-bearing protocol, premature return to high-impact activities, or technical failure (e.g., inadequate resection of the pseudotendon, resulting in suturing into non-viable scar tissue). Salvage of a re-rupture is exceptionally difficult and almost universally requires complex, massive reconstructions utilizing free tissue transfers (e.g., gracilis or semitendinosus flaps), synthetic mesh augmentations, or Achilles tendon allografts with calcaneal bone blocks.
Deep Vein Thrombosis (DVT) and subsequent Pulmonary Embolism (PE) are significant risks due to the prolonged periods of postoperative immobilization and non-weight-bearing status. The incidence of asymptomatic DVT following Achilles surgery can be as high as 30%, though symptomatic VTE is much lower. Routine chemical prophylaxis is highly recommended. The specific agent (Low Molecular Weight Heparin, Direct Oral Anticoagulants, or Aspirin) and duration of therapy should be tailored to the individual patient based on validated risk stratification models, such as the Caprini score.
Complications and Salvage Management Matrix
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Superficial Wound Dehiscence | 5% - 15% | Excessive retraction, smoking, diabetes, poor paratenon closure. | Local wound care, oral antibiotics, silver-impregnated dressings. Delay ROM exercises. |
| Deep Infection / Necrosis | 2% - 5% | Ischemic skin flaps, hematoma formation, unrecognized superficial infection. | Urgent surgical I&D, hardware/suture removal if loose, Negative Pressure Wound Therapy (NPWT), potential reverse sural artery flap for coverage. |
| Sural Nerve Injury | 3% - 10% | Posterolateral dissection, blind percutaneous suturing, aggressive retraction. | Gabapentinoids. If recalcitrant neuroma forms: surgical excision and deep muscular implantation of the proximal stump. |
| Re-Rupture | 2% - 5% | Patient non-compliance, premature weight-bearing, inadequate pseudotendon excision. | Revision surgery utilizing Achilles allograft, synthetic mesh (e.g., Artelon), or free hamstring autograft. |
| Symptomatic VTE (DVT/PE) | 1% - 3% | Prolonged immobilization, obesity, oral contraceptives, hypercoagulable states. | Therapeutic anticoagulation (DOACs, LMWH, or Warfarin) for 3 to 6 months. Early mobilization when safe. |
Phased Post-Operative Rehabilitation Protocols
The rehabilitation following the reconstruction of a neglected Achilles tendon rupture is inherently more conservative and prolonged than the protocol utilized for acute repairs. The structural integrity of the repair relies heavily on the biological incorporation of tendon transfers or extensive fascial releases, necessitating a meticulous, phased approach to mechanical loading. The overarching philosophy is to protect the repair from excessive tensile forces during the early phases of collagen synthesis while gradually introducing controlled mechanical stress to promote parallel collagen fiber alignment and restore muscle strength.
Phase I: Maximum Protection (Weeks 0–4)
Immediately following surgery, the patient is placed in a sterile, bulky Jones dressing reinforced with a rigid posterior splint or a short-leg cast. The ankle is strictly immobilized in gravity equinus, typically between 20 to 30 degrees of plantarflexion, to completely eliminate tension across the repair site. The patient is instructed to remain strictly non-weight-bearing (NWB) utilizing crutches, a knee scooter, or a wheelchair. Elevation of the operative limb above the level of the heart is critical during the first 14 days to mitigate edema, reduce hematoma formation, and protect the fragile posterior soft-tissue envelope. Sutures are typically removed at 2 to 3 weeks postoperatively, provided the incision is entirely sealed and dry.
Phase II: Controlled Mobilization (Weeks 4–8)
At the 4-week mark, the cast is removed, and the patient is transitioned into a rigid Controlled Ankle Motion (CAM) boot. The boot is fitted with a series of rigid heel wedges (usually three wedges, totaling approximately 30 degrees of equinus) to maintain the plantarflexed position. During this phase, the patient initiates progressive partial weight-bearing (PWB), slowly advancing to full weight-bearing (FWB) within the boot as tolerated by pain and swelling. Formal physical therapy commences with a focus on active plantarflexion and gentle, gravity-assisted active dorsiflexion only to the angle of the wedges. Passive dorsiflexion stretching by the therapist is strictly contraindicated, as it risks elongating the healing construct. One heel wedge is removed every 10 to 14 days, gradually bringing the foot down to a neutral (0 degrees) position by week 8.
Phase III: Strengthening and Proprioception (Weeks 8–16)
By week 8, assuming the patient can comfortably bear full weight in the CAM boot without wedges, they are transitioned into standard, supportive athletic footwear. A small, 1 cm silicone heel lift is often placed in the shoe for an additional 2 to 4 weeks to prevent sudden over-stretching of the tendon during terminal stance. Physical therapy intensifies, focusing on concentric and eccentric strengthening of the gastrocnemius-soleus complex. Exercises progress from bilateral heel raises to unilateral heel raises. Proprioceptive training is heavily emphasized, utilizing BAPS boards, single-leg stance exercises, and unstable surfaces to restore neuromuscular control. If a peroneus brevis or FHL transfer was utilized, targeted biofeedback and neuromuscular re-education are critical to facilitate "phase conversion," training the transferred muscle to fire synergistically during the push-off phase of the gait cycle.
Phase IV: Return to Activity (Months 4–6+)
The final phase of rehabilitation bridges the gap between basic functional recovery and a return to high-level athletic or occupational activities. This phase introduces plyometric exercises, agility drills, and sport-specific training. Jogging is typically permitted around the 4 to 5-month mark, provided the patient can perform a single-leg heel raise without pain and demonstrates a symmetrical gait pattern. Return to high-impact, cutting, or jumping sports is universally delayed until at least 6 to 9 months postoperatively. Clearance for unrestricted activity is strictly contingent upon the patient demonstrating at least 85% to 90% strength, power, and functional symmetry on isokinetic testing and hop tests compared to the uninjured contralateral limb.
Summary of Landmark Literature and Clinical Guidelines
The operative management of neglected Achilles tendon ruptures is guided by several decades of evolving clinical literature. The shift from purely static fascial repairs to dynamic tendon transfers represents a major paradigm shift in foot and ankle surgery.
The foundational classification and treatment algorithm for chronic ruptures was popularized by Kuwada in 1990. Kuwada's classification categorized ruptures based on defect size (Type I: <3 cm; Type II: 3-6 cm; Type III: >6 cm) and provided the first structured framework for selecting operative interventions, advocating for direct repair in small defects and V-Y advancement or local transfers for larger gaps. This algorithmic approach remains the bedrock of modern surgical decision-making.
The utilization of the peroneus brevis was pioneered by White and Kraynick in 1959, who first described transferring the tendon to bridge massive defects. Teuffer's subsequent modification in 1974 revolutionized the technique by introducing the dynamic calcaneal loop, routing the tendon through a drill hole in the calcaneus rather than relying solely on soft-tissue suturing. Teuffer's long-term outcome studies demonstrated excellent restoration of plantarflexion power and a remarkably low re-rupture rate, establishing the peroneus brevis transfer as a workhorse technique for gaps between 3 and 6 cm.
More recently, the Flexor Hallucis Longus (FHL) transfer has gained immense popularity, largely due to the landmark anatomical and clinical studies by Wapner et al. in the 1990s. Wapner demonstrated that the FHL is anatomically closer to the Achilles, possesses a stronger contractile force than the peroneus brevis, and fires in perfect physiological synchrony with the triceps surae during the gait cycle. While FHL transfer is highly effective, the peroneus brevis remains a vital tool in the surgeon's armamentarium, particularly when midfoot or forefoot pathology precludes the sacrifice of the great toe flexor.
Extensive systematic reviews by Maffulli and colleagues have further refined the clinical guidelines, emphasizing that regardless of the specific transfer chosen, the absolute key to success lies in the meticulous excision of the pseudotendon and the precise restoration of the musculotendinous resting tension. Current evidence-based guidelines strongly advocate for operative reconstruction in active patients, utilizing dynamic local tendon transfers for moderate defects and reserving complex allografts or free tissue transfers for massive, revision scenarios.
