Comprehensive Diagnosis of Wrist Conditions: An Evidence-Based Orthopaedic Guide
Key Takeaway
Accurately diagnosing wrist conditions requires a profound understanding of carpal kinematics, a systematic physical examination, and targeted imaging. This comprehensive guide details the biomechanical foundations of carpal instability, including Mayfield’s perilunar stages and Lichtman’s ring concept. Orthopedic surgeons will learn to synthesize patient history, provocative clinical testing, and advanced modalities—such as fluoroscopic arthrography and MRI—to formulate precise diagnoses and optimize surgical planning for complex wrist pathologies.
INTRODUCTION TO WRIST PATHOLOGY
The human wrist is an intricate biomechanical marvel, comprising eight carpal bones, multiple articulating surfaces, and a complex network of intrinsic and extrinsic ligaments. Diagnosing wrist conditions demands a rigorous, systematic approach that synthesizes a detailed patient history, a meticulous physical examination, and advanced imaging modalities. For the orthopaedic surgeon, mastering the diagnostic algorithm is paramount, as missed or delayed diagnoses of carpal instability or occult fractures frequently lead to rapid degenerative changes, such as Scapholunate Advanced Collapse (SLAC) or Scaphoid Nonunion Advanced Collapse (SNAC).
BIOMECHANICS AND CARPAL KINEMATICS
To accurately diagnose wrist pathology, the surgeon must first possess a profound understanding of normal carpal kinematics and the pathomechanics of injury. The carpus does not function as a single hinge but rather as a highly coordinated, multi-articulated system.
Columnar and Ring Theories of the Carpus
Two primary conceptual models dominate the understanding of carpal mechanics: Taleisnik’s columnar theory and Lichtman’s ring concept.
Taleisnik proposed that the wrist operates in three distinct columns:
1. The Central (Flexion-Extension) Column: Comprising the entire distal carpal row and the lunate.
2. The Lateral (Mobile) Column: Consisting solely of the scaphoid, which bridges the proximal and distal rows.
3. The Medial (Rotary) Column: Comprising the triquetrum, acting as a pivot point.
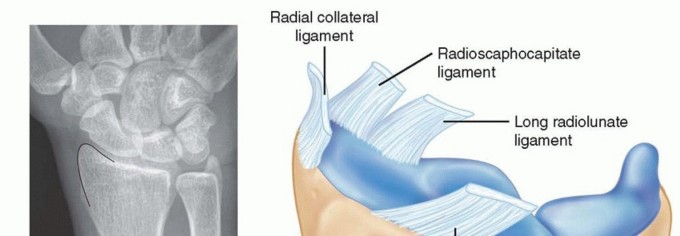
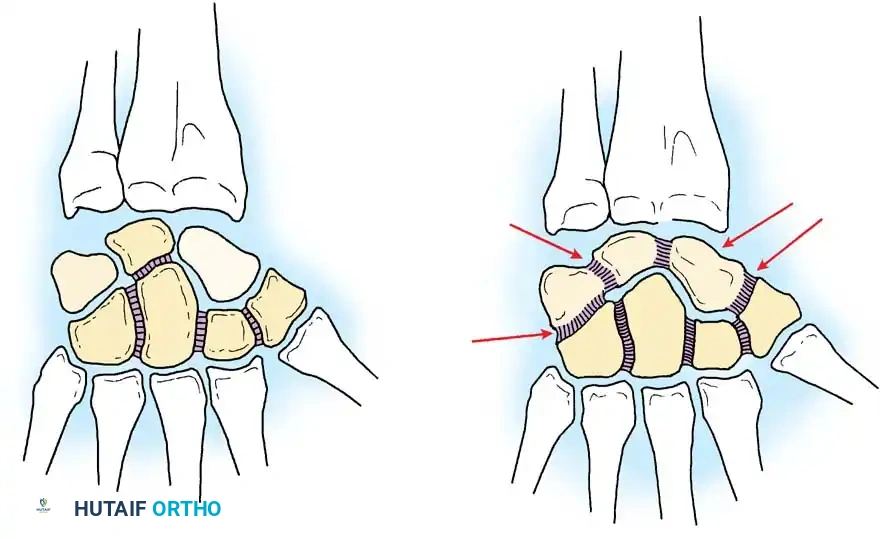
Conversely, Lichtman’s ring concept models the proximal and distal carpal rows as semirigid posts stabilized by interosseous ligaments. Normal, controlled mobility occurs at the scaphotrapezial and triquetrohamate joints. Any disruption in this ring—whether bony (e.g., scaphoid fracture) or ligamentous (e.g., scapholunate dissociation)—destabilizes the system.
Clinical Pearl: A break in Lichtman’s ring predictably alters carpal alignment. A scapholunate ligament tear uncouples the scaphoid and lunate, allowing the scaphoid to flex while the lunate extends, producing a Dorsal Intercalated Segmental Instability (DISI). Conversely, a lunotriquetral ligament tear allows the lunate to flex with the scaphoid, resulting in a Volar Intercalated Segmental Instability (VISI).
The Spectrum of Perilunar Instability
When obtaining a history of traumatic wrist conditions, the exact mechanism of injury is frequently unknown to the patient. However, Mayfield, Johnson, and Kilcoyne demonstrated that carpal injuries represent a predictable, sequential spectrum of failure. The extent of tissue disruption depends on three-dimensional loading, the duration and magnitude of forces, the hand's position at impact, and the intrinsic mechanical properties of the ligaments and bones.
Typically, carpal dislocations result from ulnar deviation combined with intercarpal supination. Scaphoid fractures frequently occur from extreme wrist extension, where the dorsal articular margin of the radius acts as a rigid fulcrum against the scaphoid waist. Conversely, flexion and pronation injuries disproportionately load the ulnar side of the wrist, frequently compromising the lunotriquetral ligament.
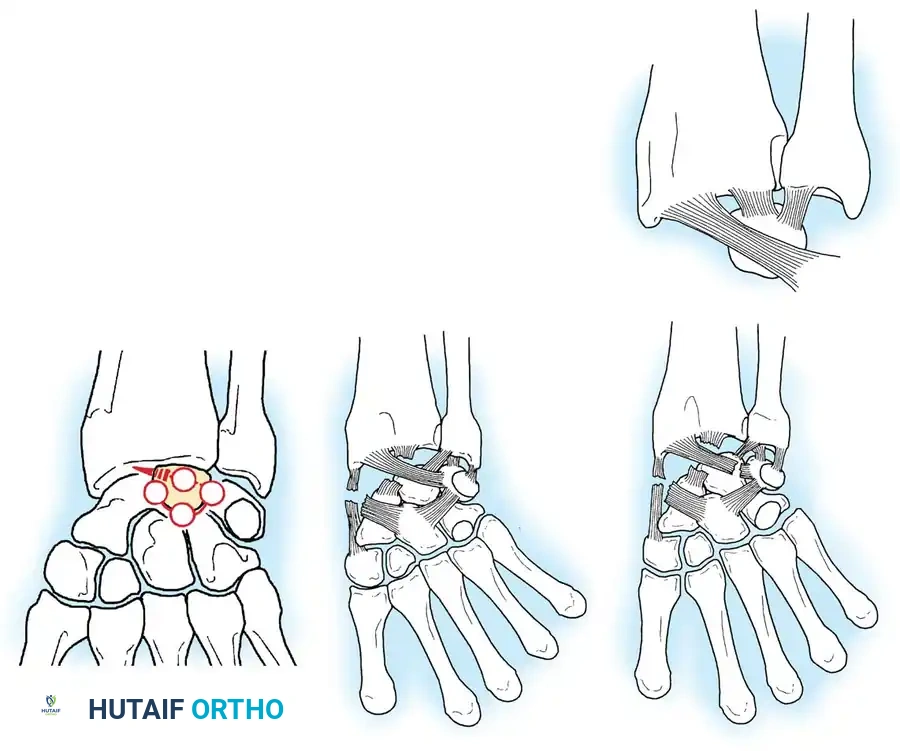
Mayfield’s stages of perilunar instability describe a progressive uncoupling of the carpus around the lunate:
* Stage I: Scapholunate dissociation (disruption of the scapholunate interosseous ligament).
* Stage II: Capitolunate dislocation (force propagates distally, disrupting the space of Poirier).
* Stage III: Lunotriquetral dissociation (the triquetrum separates from the lunate, resulting in a perilunate dislocation).
* Stage IV: Lunate dislocation (the dorsal radiocarpal ligaments fail, and the lunate is extruded volarly into the carpal tunnel).
COMPREHENSIVE CLINICAL EVALUATION
The Orthopaedic History
A meticulous history is the cornerstone of wrist diagnosis. The surgeon must document patient age, hand dominance, occupation, and specific hobbies. The chronicity of symptoms (acute trauma vs. insidious onset) dictates the diagnostic algorithm.
Crucial historical elements include:
* Mechanism of Injury: Determine if the injury involved a fall on an outstretched hand (FOOSH), rotational torque, or direct axial loading.
* Symptom Correlation: Identify activities that exacerbate or alleviate symptoms. Mechanical symptoms such as clicking, popping, snapping, or grating strongly suggest dynamic carpal instability or triangular fibrocartilage complex (TFCC) pathology.
* Medicolegal and Occupational Factors: Current work status, workers' compensation claims, and pending litigation must be documented, as they provide context for the patient's overall situation and rehabilitation potential.
* Systemic Factors: Inquire about a personal or family history of inflammatory arthritides (e.g., Rheumatoid Arthritis, Psoriatic Arthritis), which can present with spontaneous ligamentous attenuation or tenosynovitis.
Systematic Physical Examination
The physical examination must be conducted with the patient's forearm and hand fully supported, ensuring muscular relaxation. The examination proceeds systematically through inspection, palpation, range of motion (ROM) assessment, neurological evaluation, and provocative testing.
Inspection and Palpation:
Compare the injured wrist to the contralateral uninjured side. Document swelling, ecchymosis, muscle atrophy, and surgical scars. Palpation must be precise, utilizing known anatomical landmarks to isolate pathology:
* Radial Styloid & First Dorsal Compartment: Tenderness here, exacerbated by Finkelstein's test, indicates de Quervain tenosynovitis.
* Anatomic Snuffbox & Scaphoid Tuberosity: Point tenderness is highly suspicious for an occult scaphoid fracture.
* Lister’s Tubercle: Serves as a pulley for the Extensor Pollicis Longus (EPL). Tenderness may indicate EPL tenosynovitis or an impending rupture following a distal radius fracture.
* Dorsal Scapholunate Axis: Tenderness just distal to Lister's tubercle suggests scapholunate ligament injury.
* Ulnar Styloid, TFCC, and Pisiform: Ulnar-sided pain requires careful differentiation between DRUJ instability, TFCC tears, Extensor Carpi Ulnaris (ECU) subluxation, and pisotriquetral arthritis.
Surgical Warning: Do not confuse superficial tenosynovitis with deep intra-articular pathology. A thorough examination must differentiate between first dorsal compartment tenosynovitis, thumb carpometacarpal (CMC) osteoarthritis, and scaphoid pathology, as their surgical management pathways are entirely distinct.
Provocative Testing:
* Watson Scaphoid Shift Test: Assesses scapholunate instability. Pressure is applied to the volar scaphoid tuberosity as the wrist is moved from ulnar to radial deviation. A palpable "clunk" indicates subluxation of the scaphoid over the dorsal rim of the radius.
* Lunotriquetral Ballotment (Shuck) Test: Stabilize the lunate and translate the triquetrum volarly and dorsally. Pain or excessive laxity indicates LT ligament disruption.
* TFCC Grind Test: Axial loading with ulnar deviation and rotation to compress the TFCC between the ulnar head and the carpus.
ADVANCED RADIOGRAPHIC EVALUATION
Following the clinical examination, radiographic evaluation is essential for determining the diagnosis, prognosis, and surgical management of wrist conditions. Gilula et al. proposed a highly effective algorithm for the radiographic assessment of the painful wrist, emphasizing a stepwise progression from plain films to advanced cross-sectional imaging.
Standard Radiographic Series
The initial evaluation must include a routine radiographic series consisting of at least four high-quality views:
1. Posteroanterior (PA) View: Evaluates Gilula’s three carpal arcs. Disruption of these arcs indicates carpal instability or fracture.
2. Lateral View: Essential for assessing carpal alignment (collinearity of the radius, lunate, and capitate) and identifying DISI or VISI deformities.
3. Oblique View: Highlights the scaphotrapezial joint and the dorsal aspect of the triquetrum.
4. Ulnar-Deviated PA (Scaphoid) View: Elongates the scaphoid, removing its normal volar tilt to better visualize the waist and proximal pole for fractures.
Instability Series and Dynamic Imaging
If standard radiographs are normal but ligamentous instability is clinically suspected, an instability series is mandatory. This includes:
* Anteroposterior clenched-fist views (to dynamically widen the scapholunate interval, >3mm indicates a Terry Thomas sign).
* PA views in maximum radial and ulnar deviation.
* Lateral views in full flexion and extension.
Specialized Spot Views
Standard views frequently obscure complex three-dimensional carpal anatomy. Spot views are critical for isolating specific structures. The Carpal Tunnel View is an axial projection utilized to evaluate the volar bony prominences of the carpus. It is the gold standard plain radiograph for identifying avulsion fractures of the hamate hook and the volar ridge of the trapezium.

Fluoroscopy and Angled Views
When static radiographs fail to reveal the source of mechanical symptoms (e.g., popping or snapping), cine or video fluoroscopy is invaluable. The abnormal motion must be reproduced by the patient and observed fluoroscopically in real-time. Furthermore, angled fluoroscopic spot views can uncover occult fractures, such as those of the capitate waist, which may be entirely invisible on a standard PA projection due to bony overlap.

CROSS-SECTIONAL IMAGING AND ARTHROGRAPHY
Magnetic Resonance Imaging (MRI) and CT
MRI: A dedicated wrist coil is mandatory to provide the enhanced resolution required for small wrist structures. MRI is the modality of choice for evaluating:
* The Triangular Fibrocartilage Complex (TFCC).
* The Distal Radioulnar Joint (DRUJ) soft tissue stabilizers.
* Vascularity of the carpal bones (e.g., assessing for Kienböck's disease of the lunate or Preiser's disease of the scaphoid).
* Integrity of the intrinsic (SL, LT) and extrinsic carpal ligaments.
Computed Tomography (CT): CT scanning, particularly with 3D reconstruction, is the gold standard for evaluating complex intra-articular fracture geometry (e.g., distal radius fractures, complex carpal dislocations) and assessing the progression of fracture union or nonunion.
Wrist Arthrography
While largely supplanted by MR Arthrography, traditional triple-injection wrist arthrography remains a powerful dynamic tool. Contrast is injected sequentially into the radiocarpal, midcarpal, and distal radioulnar joints under fluoroscopic guidance.
During the procedure, the flow of contrast is monitored. For example, if contrast injected into the radiocarpal joint passes into the midcarpal joint between the lunate and triquetrum during ulnar deviation, it definitively indicates a full-thickness lunotriquetral ligament tear.
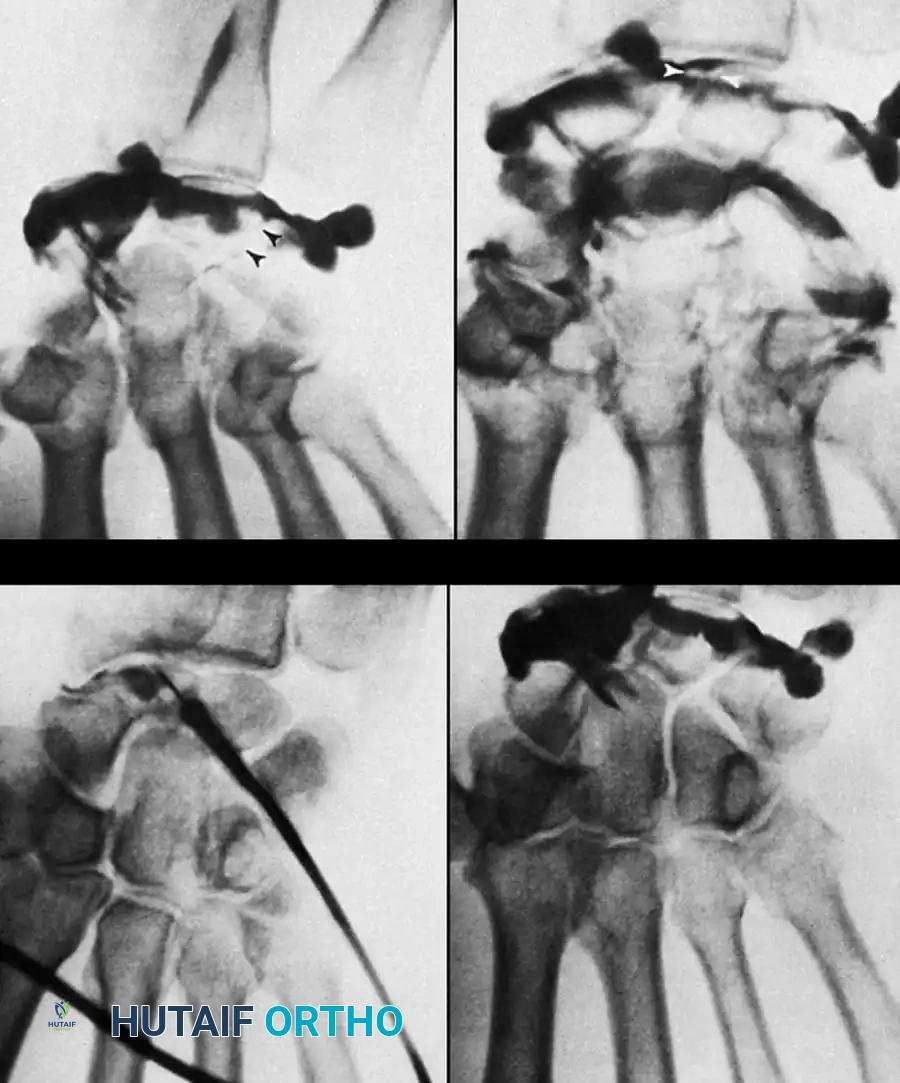
Pitfall: Contrast material can rapidly fill the midcarpal joints, making it difficult to distinguish whether the scapholunate or lunotriquetral ligament is the primary source of the leak. Fluoroscopic spot viewing during the active injection phase is critical to identify the exact site of contrast extravasation before the entire joint space is obscured.
INVASIVE DIAGNOSTIC TECHNIQUES
When non-invasive imaging is equivocal, invasive diagnostic techniques are employed to pinpoint the exact anatomical generator of pain.
Differential Local Anesthetic Injections
If the specific structure causing pain cannot be precisely identified clinically (e.g., differentiating between Extensor Carpi Ulnaris tendinopathy and underlying ulnocarpal joint impaction), a differential local anesthetic injection is highly effective.
Technique:
1. Utilize strict aseptic technique (chlorhexidine prep, sterile drapes).
2. Use a small gauge needle (25G or 27G) and a minimal volume of local anesthetic (e.g., 1-2 mL of 1% Lidocaine without epinephrine).
3. Inject precisely into the suspected structure (e.g., the ECU tendon sheath).
4. Re-examine the patient after 5 minutes. Complete resolution of pain during provocative testing confirms the anatomical source.
Note: The patient must always be advised of the benefits and risks, including infection, bleeding, and iatrogenic tendon injury.
Diagnostic Wrist Arthroscopy: Surgical Technique
Wrist arthroscopy is the ultimate gold standard for diagnosing intra-articular wrist pathology. It allows for direct, magnified visualization of the articular cartilage, intrinsic ligaments, and TFCC, while simultaneously permitting dynamic probing of these structures.
Indications:
* Unexplained chronic wrist pain unresponsive to conservative management.
* Suspected TFCC tears, SL/LT ligament tears, or chondral lesions not definitively characterized by MRI.
* Staging of SLAC/SNAC wrists prior to salvage procedures.
Positioning and Setup:
1. The patient is placed supine with the operative arm on a radiolucent hand table.
2. A regional axillary block or general anesthesia is administered.
3. A well-padded pneumatic tourniquet is applied to the proximal arm (inflated to 250 mmHg after exsanguination).
4. The hand is placed in a sterile traction tower using Chinese finger traps applied to the index and middle fingers.
5. Apply 10 to 15 pounds of longitudinal traction to distract the radiocarpal and midcarpal joints. The wrist should be in neutral rotation and slight flexion.
Surgical Approaches (Portals):
A 2.7-mm or 1.9-mm arthroscope with a 30-degree angle is utilized.
* 3-4 Portal: The primary viewing portal. Located between the 3rd compartment (EPL) and 4th compartment (EDC), just distal to Lister's tubercle. The trocar is directed 10-15 degrees proximally to match the volar tilt of the radius.
* 4-5 Portal: The primary working portal. Located between the EDC and EDM. Used for probing the TFCC and intrinsic ligaments.
* 6R Portal: Located radial to the ECU tendon. Excellent for viewing the ulnar insertion of the TFCC.
* Midcarpal Portals (Radial and Ulnar): Located 1 cm distal to the radiocarpal portals. Essential for evaluating the articular surfaces of the midcarpal joint and assessing the dynamic stability of the scapholunate and lunotriquetral intervals.
Postoperative Protocol:
Following purely diagnostic arthroscopy, the portals are closed with simple sutures or adhesive strips. A bulky soft dressing and a volar resting splint are applied. The splint is removed at 5-7 days, and immediate active range of motion is initiated to prevent arthrofibrosis. If a therapeutic intervention (e.g., TFCC repair or ligament debridement) is performed concurrently, the immobilization protocol is strictly tailored to protect the specific repair.
By meticulously integrating advanced biomechanical knowledge, systematic clinical evaluation, targeted radiographic imaging, and precise arthroscopic techniques, the orthopaedic surgeon can confidently diagnose and subsequently manage the full spectrum of complex wrist conditions.
You Might Also Like