Metatarsophalangeal Joint Synovitis and Instability: Surgical Guide
Key Takeaway
Metatarsophalangeal (MTP) joint synovitis and instability present as progressive metatarsalgia, often exacerbated by high-heeled footwear or acute hyperextension injuries. Accurate diagnosis is critical, as symptoms frequently mimic interdigital neuromas. Treatment ranges from conservative offloading and orthotics to advanced surgical interventions, including plantar plate repair, flexor-to-extensor tendon transfers, and metatarsal osteotomies. Preoperative counseling is mandatory to manage patient expectations regarding toe stiffness and alignment.
Comprehensive Introduction and Patho-Epidemiology
Instability of the lesser metatarsophalangeal (MTP) joints, frequently preceded by chronic synovitis, represents a highly complex, progressive, and often debilitating forefoot pathology. The condition is fundamentally characterized by the gradual attenuation, degeneration, and eventual catastrophic rupture of the primary static stabilizers of the joint, most notably the plantar plate and the collateral ligament complex. Historically mischaracterized as a simple "hammer toe" or isolated capsulitis, contemporary orthopedic understanding recognizes this as a multi-planar instability cascade that fundamentally alters forefoot biomechanics. As the static restraints fail, the dynamic musculotendinous forces acting across the joint become deforming vectors, driving the digit into dorsal subluxation and eventual multi-axial deviation, culminating in the classic crossover toe deformity.
The epidemiology of lesser MTP joint instability reveals a strong predilection for the second MTP joint, closely followed by the third. It predominantly affects females in their fifth to seventh decades of life. The disproportionate involvement of the second MTP joint is largely attributed to its unique anatomical configuration; it is typically the longest metatarsal, subjecting it to the highest peak plantar pressures during the terminal stance and pre-swing phases of the gait cycle. Furthermore, the presence of a concomitant hallux valgus deformity exponentially increases the risk of second MTP joint instability. As the first ray becomes mechanically incompetent and deviates laterally, load is transferred to the lesser metatarsals (transfer metatarsalgia), and the hallux physically impinges upon the second digit, exacerbating the medial-to-lateral deforming forces.
Patients with synovitis and instability of the metatarsophalangeal joint usually present with an insidious, slowly progressive course of metatarsalgia. Symptoms are characteristically aggravated by weight-bearing activities and are especially pronounced when wearing high-heeled shoes or narrow toe-box footwear, which force the MTP joints into sustained, non-physiologic hyperextension. While the onset is typically chronic and attritional, a distinct subset of patients—especially high-performance athletes—may recall an acute hyperextension injury. This acute presentation is essentially a variant of "turf toe" affecting the lesser digits, where a sudden axial load applied to a plantarflexed foot drives the MTP joint into violent dorsiflexion, acutely tearing the plantar plate from its phalangeal insertion.
Occasionally, severe neuritic symptoms may be present in the second web space, with radiation into the second and third toes. This presentation creates a significant diagnostic dilemma for the evaluating surgeon, as the clinical picture can closely mimic a compressive interdigital neuropathy.
🚨 CLINICAL PEARL: The Neuroma Trap
It must be emphatically stressed that pain in the second web space is far more likely to originate from MTP joint pathology (synovitis/plantar plate tear) than from an associated interdigital (Morton's) neuroma. Coughlin reported that previous neuroma excision had failed to relieve pain in up to 14% of patients presenting with this specific problem. Misdiagnosis leads to unnecessary nerve resections, creation of painful stump neuromas, and delayed treatment of the true mechanical instability.

Clinical presentation demonstrating localized swelling, effusion, and early hammer toe deformity indicative of underlying MTP joint synovitis and instability.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the intricate surgical anatomy of the lesser MTP joint is the absolute prerequisite for successful reconstruction. The MTP joint is a condylar joint, inherently lacking intrinsic bony stability. Its stability is almost entirely reliant on a complex capsuloligamentous network, at the center of which lies the plantar plate. The plantar plate is a robust, fibrocartilaginous, trapezoidal structure composed primarily of densely packed type I collagen. It originates from the plantar aspect of the metatarsal neck, just proximal to the articular cartilage, via a relatively thin and compliant synovial attachment. In stark contrast, its distal insertion into the plantar base of the proximal phalanx is exceptionally thick, rigid, and structurally formidable.
The collateral ligament complex works in intimate synergy with the plantar plate to provide multi-planar stability. This complex consists of the proper collateral ligament (PCL) and the accessory collateral ligament (ACL). The PCL originates from the dorsal-lateral and dorsal-medial aspects of the metatarsal head and courses obliquely to insert onto the plantar-lateral and plantar-medial base of the proximal phalanx. The ACL originates slightly more plantarly and inserts directly into the margins of the plantar plate itself. This anatomical arrangement ensures that as the proximal phalanx dorsiflexes, the plantar plate is drawn distally and dorsally over the metatarsal head, functioning as a vital load-bearing surface that protects the metatarsal articular cartilage.
Biomechanically, the plantar plate serves to resist extreme hyperextension forces during the terminal stance phase of gait. Through the windlass mechanism, as the heel rises and the digits dorsiflex, the plantar fascia (which has distal slips inserting into the plantar plate) tightens, elevating the longitudinal arch and locking the midfoot. When subjected to repetitive microtrauma—often exacerbated by restrictive footwear, a long second metatarsal, or altered forefoot biomechanics from hallux valgus—the plantar plate undergoes profound degenerative changes. Histological analysis of these failing plates reveals mucoid degeneration, disorganized collagen architecture, and hypervascularity consistent with chronic tendinosis. This degeneration leads to capsular distension (synovitis), progressive subluxation, and ultimately, a complete attritional rupture, typically at the distal phalangeal footprint.
Once the static restraints fail, the intrinsic and extrinsic musculature exacerbates the deformity. The lumbricals, which normally flex the MTP joint, shift their mechanical axis dorsal to the center of rotation, paradoxically becoming MTP joint extensors. The interossei, losing their stabilizing tether to the deep transverse metatarsal ligament (DTML), fail to resist the dorsal migration of the proximal phalanx. This unopposed dorsal pull by the extensor digitorum longus (EDL) and extensor digitorum brevis (EDB) results in the classic, rigid dorsal subluxation and crossover deformity seen in advanced disease stages.
Exhaustive Indications and Contraindications
Surgical intervention for lesser MTP joint synovitis and instability is indicated when a meticulously executed, prolonged course of conservative management fails to provide symptomatic relief, or when the patient presents with progressive, functionally limiting deformity. The specific surgical algorithm is dictated by the precise anatomical structures that have failed, the flexibility or rigidity of the deformity, and the presence of concurrent forefoot pathology (e.g., hallux valgus, profound metatarsus adductus).
Absolute contraindications to reconstructive forefoot surgery include severe peripheral vascular disease with inadequate distal perfusion, active soft tissue or bone infection, and uncontrolled medical comorbidities that preclude safe anesthesia. Relative contraindications encompass severe, poorly controlled diabetes mellitus with profound peripheral neuropathy (Charcot neuroarthropathy risk), heavy tobacco use (due to unacceptably high rates of non-union and wound dehiscence), and patients with unrealistic postoperative expectations regarding cosmesis and joint mobility.
| Pathology Stage / Clinical Finding | Primary Surgical Indications | Contraindications / Relative Contraindications |
|---|---|---|
| Stage 1: Chronic Synovitis, No Instability (Negative Drawer) | Joint-preserving synovectomy, EDL lengthening, conservative orthotic management. | Frank subluxation >50%, complete plantar plate tear on MRI. |
| Stage 2: Mild Instability, Reducible Deformity | Plantar plate repair (dorsal or plantar approach), possible Weil osteotomy if metatarsal is excessively long. | Rigid, fixed deformity requiring extensive bony resection. |
| Stage 3: Severe Instability, Subluxation/Dislocation | Weil osteotomy, formal plantar plate reconstruction, FDL/EDB tendon transfers, collateral ligament repair. | Active infection, severe vascular compromise (ABI < 0.5). |
| Stage 4: Rigid Crossover Toe, Advanced Arthrosis | PIP joint arthroplasty/fusion, Weil osteotomy, FDL transfer, possible MTP resection arthroplasty. | Patient expectation of a perfectly mobile, anatomically normal digit. |
| Concomitant Interdigital Pain | Rule out MTP instability first. If true neuroma coexists, resect only if mechanically distinct. | Primary neuroma excision without addressing underlying MTP instability. |
The decision to proceed with surgery must be accompanied by a frank discussion regarding the salvage nature of advanced reconstructions. As the deformity progresses from a flexible subluxation to a rigid dislocation, the surgical focus shifts from anatomical restoration to functional salvage. In cases of severe, long-standing dislocation with secondary degenerative joint disease of the MTP joint, soft tissue reconstruction alone is doomed to fail, necessitating aggressive bony decompression and dynamic tendon transfers.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative clinical evaluation and radiographic templating are the cornerstones of successful MTP joint reconstruction. Clinical evaluation should begin with an inspection of the patient's standing posture. Look for splaying of the digits, loss of ground purchase by the affected toe (the "floating toe" sign), or a frank crossover toe deformity, which most commonly manifests as the second toe crossing dorsally and medially over the hallux. Palpation will often reveal a localized effusion and exquisite tenderness directly over the MTP joint capsule, rather than in the intermetatarsal space.
The Lachman test of the MTP joint (dorsal-plantar drawer test) is the absolute gold standard for assessing instability. The examiner stabilizes the metatarsal head with one hand while grasping the base of the proximal phalanx with the other, applying a dorsal translation force. A positive test is indicated by abnormal dorsal translation of the proximal phalanx on the metatarsal head, often accompanied by a palpable "clunk" or exact reproduction of the patient's mechanical pain. This instability is graded from 0 (stable) to 4 (dislocatable).
Standard weight-bearing radiographs of the foot (anteroposterior, lateral, and oblique views) are mandatory. Early in the disease process, radiographs may appear entirely normal, belying the significant soft tissue pathology present. As instability progresses, the AP view may show widening of the intermetatarsal space, medial or lateral deviation of the digit, and a long second metatarsal extending past the first metatarsal (a positive metatarsal protrusion distance).
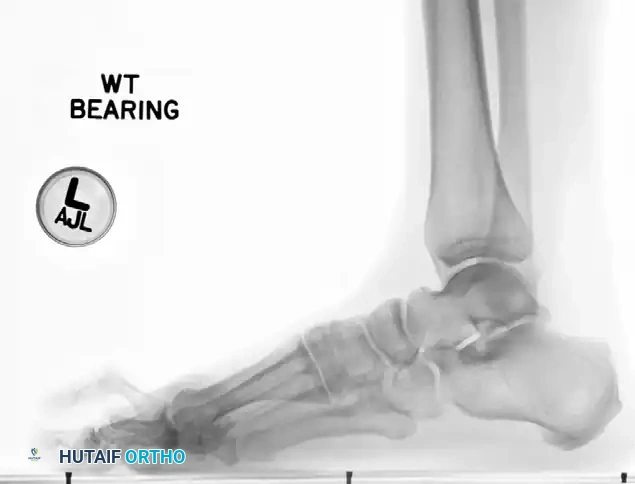
Weight-bearing lateral radiograph of the foot. Note the dorsal subluxation of the proximal phalanx relative to the metatarsal head, a hallmark of advanced plantar plate insufficiency.
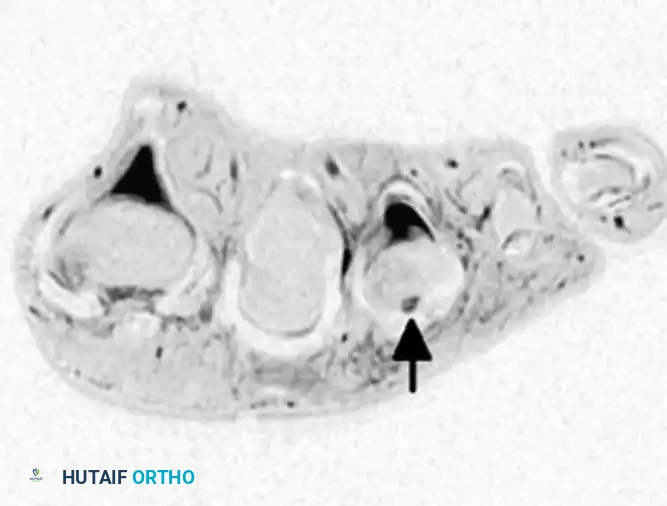
When clinical suspicion remains high despite normal radiographs, Magnetic Resonance Imaging (MRI) is the modality of choice. High-resolution MRI, utilizing a dedicated small receiver surface coil, provides excellent visualization of the plantar plate, collateral ligaments, and joint effusion. Standard sequences must include T2-weighted fat-suppressed and proton density images in the axial, coronal, and sagittal planes.
Axial/Coronal MRI utilizing a small receiver coil. The arrow indicates a localized joint effusion and disruption of the lateral collateral ligament complex.
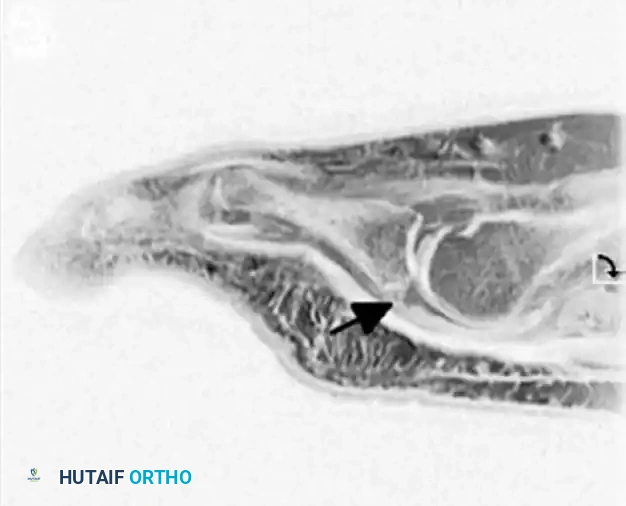
Sagittal MRI demonstrating a high-signal intensity defect at the insertion of the plantar plate into the base of the proximal phalanx, confirming an attritional rupture.
Preoperative templating focuses on assessing the metatarsal cascade. If a Weil osteotomy is planned, the surgeon must calculate the exact amount of proximal translation required to restore a harmonious metatarsal parabola (typically the second metatarsal should be 1-2mm longer than the first, and progressively shorter laterally). The patient is positioned supine on the operating table with a bump placed under the ipsilateral hip to internally rotate the leg to a neutral position. A well-padded thigh or calf tourniquet is applied to ensure a bloodless surgical field, which is critical for identifying the attenuated remnants of the plantar plate.
Step-by-Step Surgical Approach and Fixation Technique
Surgical decision-making is dictated by the degree of instability, the presence of fixed deformities, and the specific anatomical structures that have failed. The surgical approach must be systematic, addressing the soft tissue contractures, the bony architecture, and the dynamic muscle imbalances in a sequential manner.
Soft Tissue Balancing and Synovectomy (Mild Disease)
For chronic synovitis of the joint that is unresponsive to conservative treatment, but where no significant instability is present (negative dorsal drawer test, Stage 1 disease), a joint-preserving soft tissue procedure is indicated.
The procedure begins with a dorsal longitudinal incision centered over the affected MTP joint, carefully preserving the dorsal cutaneous nerves. The extensor hood is identified, and the extensor digitorum longus (EDL) tendon is isolated. To relieve the dorsal deforming force, the EDL is lengthened, typically via a Z-lengthening technique, allowing for 10-15 mm of excursion. A longitudinal dorsal capsulotomy is then performed, entering the joint space. A meticulous, aggressive synovectomy is carried out using a combination of sharp dissection and a small motorized shaver, removing all hypertrophic, inflamed synovial tissue to relieve capsular distension. The collateral ligaments are inspected; if intact, the joint is irrigated, and the capsule is closed in a pants-over-vest fashion to provide slight dorsal reefing. Very occasionally, a true second web space neuroma is present concurrently. It should be resected only if preoperative symptoms strongly suggest neuritic pain that is completely distinct from the mechanical joint pain.
Plantar Plate Repair Techniques (Moderate to Severe Instability)
If the joint subluxates more than 50% on clinical examination (Stage 2 or 3), a stabilizing procedure must be added to the synovectomy. Attritional rupture of the plantar plate has been reported to occur almost exclusively at its distal attachment into the plantar aspect of the proximal phalanx.
Direct repair of the plantar plate to the base of the proximal phalanx using a plantar approach provides excellent direct visualization of the pathology. However, it carries significant risks of painful plantar scar formation, intractable keratosis, and potential injury to the plantar digital neurovascular bundles. Consequently, the dorsal approach is currently the favored option in the definitive management strategy of this condition, despite being technically tedious.
The dorsal approach typically requires a concurrent Weil osteotomy of the metatarsal to decompress the joint and allow sufficient visualization of the plantar structures. Once the metatarsal head is mobilized, a McGlamry elevator is used to release the plantar plate from any plantar adhesions. A specialized suture passing device (e.g., a Viper or similar pigtail lasso) is used to weave two highly robust, non-absorbable sutures (such as #0 or 2-0 FiberWire) through the viable proximal stump of the torn plantar plate using a mattress or Krackow configuration. Two parallel drill holes are then made from dorsal to plantar through the base of the proximal phalanx. The suture limbs are passed through these osseous tunnels and tied dorsally over a bone bridge while the toe is held in 10 to 15 degrees of plantarflexion.
🔪 SURGICAL WARNING: Plantar Condylectomy
Care should be taken to remove any adherent plantar plate from the plantar surface of the metatarsal head. We have found that, especially if a plantar intractable plantar keratosis (callosity) is present, a plantar condylectomy of the metatarsal head provides a bleeding, cancellous surface for the attachment and healing of the plantar plate. This step provides critical additional static stability to the joint and stimulates a robust fibrovascular healing response.
Metatarsal Osteotomies
Addressing the bony architecture is often necessary to decompress the joint, reduce tension on the soft tissue repairs, and correct abnormal metatarsal cascade lengths. The traditional Weil osteotomy is an intra-articular, oblique osteotomy performed parallel to the weight-bearing surface of the foot. It allows for controlled proximal translation of the metatarsal head without altering its plantar elevation, effectively shortening the ray and relaxing the intrinsic musculature.
Garg et al. described a modification of the traditional Weil osteotomy—a “segmental” osteotomy—that effectively shortens the metatarsal and reduces the plantar load under the metatarsal head while avoiding the intra-articular nature of the Weil cut.

Diagram A: The segmental osteotomy technique. Two parallel, oblique dorsal-to-plantar cuts are made in the distal metatarsal metaphysis to remove a precise segment of bone, allowing for controlled shortening.

Diagram B: Following the removal of the bone segment, the capital fragment is translated proximally and secured with a single dorsal-to-plantar compression screw.
While technically easier to perform than the standard Weil osteotomy and theoretically preserving the articular surface, the segmental osteotomy has been associated with frequent complications. These include transfer metatarsalgia (due to unpredictable elevation of the metatarsal head), floating toe deformity, infection, and delayed wound healing. Consequently, the traditional Weil osteotomy, secured with a single snap-off twist-off screw or a small fragment cortical screw, remains the gold standard for most reconstructive forefoot surgeons.
Dynamic Stabilization and Tendon Transfers
When static repairs are insufficient, the plantar plate tissue is too friable to hold a suture, or the deformity is rigid, dynamic stabilization is required. Transfer of the flexor tendon to the extensor tendon (the Girdlestone-Taylor procedure) has been highly effective in stabilizing the joint and producing satisfactory long-term results.
In this procedure, the flexor digitorum longus (FDL) is harvested at the level of the distal interphalangeal joint, split longitudinally, and routed dorsally around the proximal phalanx to be sutured into the extensor expansion. Although originally described as a treatment for flexible hammer toes, this procedure is arguably best used for providing dynamic plantarflexion stability to an unstable MTP joint, effectively replacing the function of the failed plantar plate.
Alternatively, transfer or rerouting of the extensor digitorum brevis (EDB) tendon underneath the deep transverse intermetatarsal ligament has been reported to be highly effective in the treatment of crossover second toe deformities. This technique creates a dynamic lateral and plantar tether, counteracting the medial and dorsal deforming forces.
Complications, Incidence Rates, and Salvage Management
Reconstructive surgery of the lesser MTP joints is fraught with potential complications, even in the hands of highly experienced forefoot surgeons. The delicate balance of soft tissue tension and bony alignment is easily disrupted, leading to recurrent deformity or profound stiffness. Thorough preoperative counseling regarding these risks is mandatory.
| Complication | Estimated Incidence | Prevention and Salvage Management Strategies |
|---|---|---|
| MTP Joint Stiffness | 30% - 60% | Prevention: Aggressive early passive plantarflexion ROM; precise soft tissue tensioning. Salvage: Often well-tolerated if the toe is plantigrade. May require manipulation under anesthesia or dorsal capsulotomy if severe extension contracture occurs. |
| Floating Toe Deformity | 15% - 30% | Prevention: Avoid excessive shortening during Weil osteotomy; ensure secure plantar plate repair; consider concurrent FDL transfer. Salvage: FDL to extensor hood transfer; revision plantar plate repair. |
| Recurrent Subluxation/Deviation | 10% - 20% | Prevention: Address concomitant hallux valgus; ensure complete release of contracted structures; robust fixation of osteotomies. Salvage: Proximal interphalangeal (PIP) fusion; revision osteotomy; eventual syndactylization or amputation in extreme, painful cases. |
| Transfer Metatarsalgia | 5% - 15% | Prevention: Meticulous preoperative templating to restore the metatarsal cascade; avoid dorsal elevation of the metatarsal head during osteotomy fixation. Salvage: Custom orthotics with metatarsal offloading; corrective osteotomy of the newly overloaded adjacent metatarsal. |
| Non-union / Hardware Failure | < 5% | Prevention: Rigid internal fixation; strict adherence to post-operative weight-bearing protocols; smoking cessation. Salvage: Revision open reduction internal fixation with bone grafting; hardware removal if symptomatic and union is achieved. |
In cases of severe, rigid crossover toe deformity, a multi-level approach is required. Myerson and Jung reported combining flexor digitorum longus (FDL) tendon transfer with proximal interphalangeal (PIP) resection arthroplasty, PIP fusion, and/or Weil osteotomy of the metatarsal. While this comprehensive approach addresses all components of the deformity, the complication profile is not insignificant. Frequent complications were noted, such as residual extension contractures at the MTP joint, recurrent medial or lateral deviation of the joint, and severe stiffness of the toe (loss of physiological flexion). These complications resulted in up to 14% of patients being dissatisfied with the procedure.
🗣️ CLINICAL PEARL: Managing Expectations
It cannot be emphasized enough that with lesser toe surgery, preoperative counseling regarding patient expectations is absolutely mandatory. Patients must be explicitly informed that the primary goal of surgery is pain relief, the elimination of severe plantar keratoses, and the restoration of a plantigrade foot that fits into standard, comfortable footwear. The goal is not the restoration of a perfectly straight, highly mobile, or cosmetically flawless toe. Postoperative stiffness is an expected, and often necessary, outcome of joint stabilization, not a complication.
Phased Post-Operative Rehabilitation Protocols
The success of lesser MTP joint reconstruction is as dependent on strict adherence to postoperative rehabilitation protocols as it is on surgical execution. The rehabilitation phases are designed to protect the delicate soft tissue repairs while preventing the dreaded complication of severe, function-limiting stiffness.
Weeks 0-2: The Protection Phase
Immediately postoperatively, the patient is placed in a bulky, compressive forefoot dressing and a rigid postoperative shoe or controlled ankle motion (CAM) boot. Weight-bearing is strictly restricted to the heel to protect the soft tissue repair and osteotomy sites from axial loading and shear forces. The toe is explicitly taped or splinted in a slightly plantarflexed position (10 to 15 degrees) to remove all tension from the dorsal incision and, more importantly, to protect the plantar plate repair from extension forces. Elevation and strict icing protocols are instituted to manage edema.
Weeks 2-6: The Early Mobilization Phase
At the 14-day mark, the initial dressings are taken down, and sutures are removed, provided wound healing is adequate. The toe is continuously taped in plantarflexion (using crossover taping techniques or specialized toe alignment splints) to protect the plantar plate repair or tendon transfer. Progressive weight-bearing in a stiff-soled shoe is initiated, allowing the patient to transition from heel-touch to flat-foot walking, provided the rigid sole prevents MTP joint dorsiflexion. Gentle, passive plantarflexion exercises are initiated by the patient or physical therapist, but active dorsiflexion is strictly prohibited.
Weeks 6-12: The Strengthening and Maturation Phase
Radiographs are obtained at 6 weeks to confirm osseous union of any metatarsal osteotomies. Once union is confirmed, taping is gradually discontinued. Aggressive active and passive range of motion exercises are initiated, focusing heavily on plantarflexion to prevent dorsal contracture and restore intrinsic muscle function. Strengthening of the intrinsic foot musculature (e.g., towel scrunches, marble pickups) is emphasized. Return to standard, supportive footwear is allowed as swelling permits, though wide-toe-box shoes with a rigid shank are recommended indefinitely. High-impact activities, running, and the use of high-heeled shoes are strictly prohibited until at least 4 to 6 months postoperatively, and often discouraged permanently to prevent late recurrence.
Summary of Landmark Literature and Clinical Guidelines
The evolution of surgical management for lesser MTP joint instability is well-documented in orthopedic literature, transitioning from simple excisional arthroplasties to complex, anatomically based reconstructions.
Coughlin's seminal work on the "crossover second toe deformity" fundamentally shifted the paradigm by identifying the plantar plate and collateral ligaments as the primary pathological lesions. His long-term outcome studies highlighted the high failure rates of isolated soft-tissue procedures in the presence of bony malalignment, cementing the role of the Weil osteotomy in modern treatment algorithms. Furthermore, Coughlin's identification of the "Neuroma Trap"—where MTP instability is misdiagnosed as a Morton's neuroma—remains a critical diagnostic axiom for all practicing foot and ankle surgeons.
Haddad et al. provided a widely utilized clinical grading system for lesser MTP joint instability, categorizing the pathology from mild synovitis to frank dislocation. This classification system remains instrumental in guiding step-wise surgical decision-making.
Myerson's extensive research on dynamic stabilization, particularly the integration of the FDL tendon transfer in severe crossover toe deformities, demonstrated that while static repairs (plantar plate reconstruction) are ideal for early-stage disease, dynamic tendon transfers are essential salvage procedures for rigid, long-standing dislocations where native tissue is non-viable. Current clinical guidelines advocate for a tailored, multi-modal approach: addressing the soft tissue defect directly (dorsal plantar plate repair), decompressing the joint (Weil osteotomy), and managing patient expectations regarding postoperative stiffness and functional outcomes.
📚 Medical References
