Comprehensive Introduction and Patho-Epidemiology
Congenital contracture, angulation, or subluxation of the fifth toe—frequently referred to in the orthopedic literature as an overriding fifth toe, digitus quintus varus, or congenital crossover toe—represents a fairly common familial deformity that challenges both the pediatric and adult foot and ankle surgeon. Characterized by a triplanar deformity consisting of dorsiflexion at the metatarsophalangeal (MTP) joint, adduction, and varus rotation of the fifth digit, the condition is often bilateral and is invariably present at birth. The precise genetic inheritance pattern is generally considered to be autosomal dominant with variable penetrance, leading to a wide spectrum of phenotypic presentations ranging from a mild, flexible aesthetic anomaly to a rigidly contracted, non-functional digit.
While the anomaly is rarely disabling in early childhood due to the inherent flexibility of the pediatric foot and the lack of constrictive shoe wear, the natural history of the condition is one of progressive rigidity. The soft tissues—including the skin, joint capsule, and tendinous structures—undergo adaptive shortening in response to the sustained abnormal posture. Simultaneously, altered foot biomechanics and the repetitive microtrauma associated with ambulation exacerbate the structural imbalance. By the time the patient reaches adolescence or early adulthood, the once-flexible deformity typically transitions into a rigid structural pathology, leading to significant symptomatic complaints that prompt surgical consultation.
Conservative management strategies, encompassing taping, dynamic splinting, and toe spacers, are occasionally attempted in the neonatal period with variable and often transient success. However, these non-operative modalities are universally ineffective for established, rigid deformities in older children and adults. The primary indication for surgical intervention is the alleviation of pain, which most commonly arises from shoewear friction leading to the formation of a painful dorsal heloma durum (hard corn) over the proximal interphalangeal (PIP) joint, or from impingement of the fifth toe against the adjacent fourth toe. Additionally, surgery is indicated to restore a functional, plantigrade alignment of the forefoot and to address profound cosmetic concerns that cause psychological distress to the patient.
The direction, severity, and rigidity of the angulation dictate the appropriate operative procedure. The surgical armamentarium for the correction of an angulated overriding fifth toe encompasses a broad spectrum of techniques. These range from isolated soft-tissue corrections (such as tenotomies and capsulotomies) to complex cutaneous realignments (Z-plasty), comprehensive periarticular releases (Butler arthroplasty), osseous interventions (proximal phalangectomy or metatarsal osteotomies), and, in severe, recurrent, or highly dysvascular cases, terminal amputation. A profound understanding of the underlying pathoanatomy is paramount for the surgeon to select the optimal procedure that will yield a durable, functional, and aesthetically pleasing outcome.
Detailed Surgical Anatomy and Biomechanics
The biomechanical foundation of the overriding fifth toe deformity is primarily driven by a dynamic and structural imbalance of the extensor mechanism, specifically a profound contracture of the extensor digitorum longus (EDL) tendon. In the normal foot, the EDL acts synergistically with the intrinsic musculature to dorsiflex the toes and stabilize the MTP joints during the swing phase of gait. However, in the congenital crossover toe, the EDL tendon becomes aberrantly shortened and hyperactive, exerting an unyielding dorsiflexion force on the proximal phalanx. Because the fifth toe lacks the robust stabilizing influence of a dedicated extensor digitorum brevis (EDB) tendon in many individuals, this unopposed EDL traction leads to rapid and sustained MTP joint subluxation.
Accompanying the tendinous contracture are severe secondary contractures of the capsuloligamentous structures. The dorsal and medial aspects of the MTP joint capsule become thickened and fibrotic, acting as a primary restraint to plantarflexion and abduction. The collateral ligaments, particularly the medial collateral ligament, undergo adaptive shortening, locking the toe into its characteristic varus and adducted posture. Furthermore, the plantar plate—the primary static stabilizer against dorsal MTP subluxation—becomes attenuated and structurally compromised. In long-standing, rigid deformities, the plantar capsule and the plantar plate become densely adherent to the dorsal aspect of the metatarsal head, creating a physical block that prevents the proximal phalanx from reducing anatomically into the joint space.
A critical, yet frequently underestimated, component of the pathoanatomy is the cutaneous tethering. Over time, the skin overlying the dorsal aspect of the fourth web space becomes profoundly contracted, forming a restrictive dermal and epidermal band. This skin contracture acts as a bowstring across the MTP joint; any attempt to manually plantarflex and abduct the toe places severe tension on this cutaneous tether. If a surgical correction addresses only the deep tendinous and capsular structures without adequately lengthening this dorsal skin envelope, the resultant tension will inevitably lead to wound dehiscence, vascular compromise, or rapid recurrence of the deformity.
The neurovascular anatomy of the fifth digit demands meticulous attention during any corrective procedure. The plantar digital arteries and nerves course intimately along the plantar-medial and plantar-lateral aspects of the digit. In the setting of a chronic overriding toe, these neurovascular bundles adapt to the shortened, dorsiflexed, and rotated position. When the toe is surgically derotated and plantarflexed into a corrected anatomical alignment, these structures are suddenly subjected to acute longitudinal traction. The fifth toe is notoriously unforgiving of vascular tension, and excessive stretch on the digital arteries can precipitate intense vasospasm or intimal injury, leading to the dreaded "white toe" complication and subsequent ischemic necrosis.
Exhaustive Indications and Contraindications
The decision to proceed with operative management of a fifth toe contracture must be based on a thorough clinical evaluation, a clear understanding of the patient's symptoms, and the failure of appropriate conservative measures. Surgery is rarely indicated for purely cosmetic reasons in the absence of pain or functional impairment, though the psychological impact of severe deformities should not be entirely discounted. The primary indication is the presence of a rigid deformity accompanied by intractable pain, typically localized to a dorsal heloma durum over the PIP joint or the lateral aspect of the fifth metatarsal head, which prevents the patient from wearing standard, commercially available footwear.
Furthermore, surgical intervention is indicated when the overriding toe causes secondary pathology in the adjacent digits. The constant pressure of the fifth toe resting upon the dorsal aspect of the fourth toe can lead to interdigital maceration, ulceration, and the formation of heloma molle (soft corns) within the web space. In patients with compromised healing potential, such as those with mild to moderate peripheral neuropathy or well-controlled diabetes mellitus, prophylactic correction of a severe deformity may be indicated to prevent impending ulceration and subsequent deep space infection, provided their vascular status is adequate to support wound healing.
Contraindications to surgical correction must be rigorously respected to avoid catastrophic complications, including digit loss. Absolute contraindications include severe peripheral arterial disease with absent pedal pulses and inadequate capillary refill, as the tenuous vascular supply will not tolerate the trauma of surgery or the tension of realignment. Active local or systemic infection is also an absolute contraindication until definitively eradicated. Relative contraindications include poorly controlled diabetes mellitus (HbA1c > 8.0%), severe sensory neuropathy (where the patient cannot perceive post-operative pressure or ischemic pain), and unrealistic patient expectations regarding the final cosmetic appearance or functional capacity of the toe.
To assist the surgeon in clinical decision-making, the following table outlines the primary indications and contraindications for the operative management of fifth toe contractures:
| Category | Specific Clinical Scenarios | Surgical Considerations |
|---|---|---|
| Primary Indications | Rigid deformity with intractable pain; Failure of conservative care (taping, wide toe-box shoes); Recurrent dorsal heloma durum; Interdigital ulceration. | Surgery aims to restore plantigrade alignment, alleviate focal pressure points, and allow for normal footwear. |
| Secondary Indications | Impending ulceration in at-risk patients (e.g., controlled diabetics); Severe functional impairment during ambulation; Progressive deformity altering forefoot biomechanics. | Prophylactic correction requires rigorous pre-operative vascular assessment to ensure healing capacity. |
| Absolute Contraindications | Severe peripheral vascular disease (ABI < 0.5, absent pulses); Active local soft tissue or bone infection; Gangrenous changes. | Surgical intervention will likely precipitate complete ischemic necrosis or systemic sepsis. Amputation may be the only surgical option. |
| Relative Contraindications | Profound peripheral neuropathy; Poorly controlled diabetes (HbA1c > 8.0%); Heavy tobacco use; Unrealistic cosmetic expectations. | High risk of post-operative Charcot arthropathy, non-healing wounds, or patient dissatisfaction. Requires extensive pre-operative counseling. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning begins with a meticulous clinical examination to assess the flexibility of the deformity and the integrity of the soft-tissue envelope. The surgeon must perform a dynamic assessment, similar to a Kelikian push-up test, by applying pressure to the plantar aspect of the fifth metatarsal head while attempting to manually plantarflex and derotate the toe. If the toe can be passively corrected to a neutral position, a soft-tissue procedure alone (such as a Z-plasty and tenotomy) may suffice. If the deformity is rigidly fixed and the MTP joint cannot be reduced, a more extensive periarticular release, such as the Butler arthroplasty, or osseous shortening will be required.
Radiographic evaluation is a mandatory component of the pre-operative workup. Standard weight-bearing anteroposterior (AP), lateral, and oblique radiographs of the foot must be obtained. The AP view is critical for assessing the degree of varus and adduction, the presence of MTP joint subluxation or frank dislocation, and the relative length of the fifth metatarsal compared to the fourth. The lateral and oblique views help delineate the extent of dorsal MTP subluxation and any concurrent PIP joint contractures (hammer toe deformity). While formal templating is more commonly associated with arthroplasty or complex osteotomies, the surgeon must mentally template the required soft-tissue transpositions and anticipate whether a concurrent proximal phalanx hemi-resection might be necessary to decompress the joint.
Anesthesia and hemostasis are critical elements of the pre-operative setup. The procedure is typically performed under a comprehensive regional ankle block, utilizing a long-acting local anesthetic (such as bupivacaine or ropivacaine) combined with monitored anesthesia care (MAC) or light sedation. The ankle block ensures complete regional anesthesia without distorting the local anatomy of the forefoot, which can occur if local infiltration is used directly at the surgical site. To provide a bloodless surgical field—which is absolutely essential for identifying and protecting the delicate digital neurovascular bundles—the foot is exsanguinated using an Esmarch bandage, and a sterile ankle or calf tourniquet is inflated to an appropriate pressure (typically 250 mm Hg).
Patient positioning is designed to maximize exposure of the lateral forefoot. The patient is placed in the supine position on the operating table. A gel bump or sandbag is placed under the ipsilateral hip to internally rotate the lower extremity. This maneuver brings the lateral aspect of the foot, specifically the fifth MTP joint and the fourth web space, directly into the surgeon's line of sight, preventing the need for awkward leaning or excessive retraction by the surgical assistant. The foot is prepped and draped in a standard sterile fashion, ensuring that the entire forefoot and ankle are exposed to allow for intraoperative assessment of toe alignment relative to the entire foot cascade.
Step-by-Step Surgical Approach and Fixation Technique
The surgical correction of the overriding fifth toe requires a nuanced approach tailored to the severity of the contracture. The surgeon must be adept at various techniques, ranging from skin lengthening procedures to complex capsular realignments. The ultimate goal is to achieve a tension-free, plantigrade digit that rests harmoniously adjacent to the fourth toe without compromising vascular perfusion.
Soft-Tissue Release and Cutaneous Z-Plasty (Thordarson Technique)
Thordarson described a highly effective soft-tissue release combined with a cutaneous Z-plasty for the correction of the congenital overriding fifth toe. In his series, patients reported high satisfaction with the appearance of their foot, with no recurrent deformities, no activity or shoewear limitations, and crucially, no shortening of the toe. This technique is particularly advantageous as it preserves the skeletal integrity of the digit while providing robust soft-tissue lengthening. The success of the Z-plasty relies on precise geometric design. A 60-degree angle for the Z-plasty limbs theoretically provides a 73% increase in length along the central axis, which is optimal for releasing the dorsal skin contracture without compromising the vascularity of the flaps.
- Incision Design: Approach the fifth MTP joint through a meticulously planned Z-plasty incision. With the toe held manually in the fully corrected (plantarflexed and abducted) position, draw the central limb of the Z-plasty directly along the band of contracted skin extending from the dorsum of the fifth toe down into the fourth web space.
- Flap Creation: Create the proximal and distal limbs of the Z-plasty so they are of equal lengths to the central limb. Construct the angle of the Z-plasty at exactly 60 degrees. This specific angulation allows maximal elongation along the longitudinal axis of the Z-plasty when the limbs are transposed. Carefully incise the skin and elevate the full-thickness flaps, preserving the subdermal vascular plexus.
- Tendon Release: Deepen the incision through the subcutaneous tissue, taking care to retract and protect the dorsal cutaneous nerve branches. Identify the contracted extensor digitorum longus (EDL) tendon of the fifth toe. Release the EDL tendon in a long, oblique fashion (fractional lengthening) or via a Z-lengthening technique to allow for controlled elongation while maintaining continuity.
- Capsulotomy: Expose the MTP joint. Perform a thorough release of the dorsal and medial capsule. Once released, place the toe in the corrected position. Assess for any residual plantar capsular adhesions; if the toe does not rest naturally in the corrected position, further capsular release using a McGlamry elevator or a sharp blade is required to free the plantar plate from the metatarsal head.
- Flap Transposition and Closure: Transpose the two triangular limbs of the Z-plasty. The transposition will reorient the central limb transversely, effectively lengthening the dorsal skin and obliterating the cutaneous tether. Suture the flaps with interrupted 4-0 or 5-0 non-absorbable sutures (e.g., nylon or Prolene), ensuring minimal tension on the apical tips to prevent marginal necrosis.
Butler Arthroplasty
For more rigid or severe dorsally overriding fifth toes, particularly those with profound capsular fibrosis that do not respond to simple Z-plasty, the Butler arthroplasty provides a comprehensive release and realignment. Black et al. reported good to excellent results in 34 of 36 (94%) Butler arthroplasties performed for this specific deformity. The procedure utilizes a double racquet incision that acts as a V-Y advancement flap, combined with extensive capsular and tendinous releases. A primary complication of the Butler arthroplasty is the potential for vascular damage caused by excessive tension on the neurovascular bundle during derotation and plantarflexion of the toe.
- Incision and Exposure: After preparing and draping the foot and applying a tourniquet, make a double racquet incision. The dorsal handle of the racquet should follow the course of the extensor longus tendon, extending proximally over the metatarsal. The plantar handle is inclined laterally to provide a circumferential incision around the base of the fifth toe, effectively separating the digit from its restrictive soft-tissue envelope.
- Flap Elevation: To expose the contracted extensor tendon and the joint capsule, elevate the skin flaps by careful blunt dissection. It is imperative to identify and protect the digital neurovascular bundles, which lie in close proximity to the plantar aspect of the incision. Retract these structures gently using vessel loops.
- Deep Dissection: Transect the extensor tendon to the fifth toe. Proceed to divide the dorsal aspect of the metatarsophalangeal joint capsule completely. Extend the capsulotomy medially and laterally, completely freeing the proximal phalanx from the metatarsal head dorsally.
- Derotation and Plantar Release: Following the dorsal release, the toe should partially rotate downward and laterally into the correct position. However, in long-standing deformities, the plantar aspect of the capsule becomes highly adherent and prevents full reduction of the proximal phalanx onto the metatarsal head during derotation.
- Plantar Capsulotomy: If necessary, separate the adherent plantar capsule from the metatarsal head by blunt dissection using a small periosteal elevator. Divide it transversely to allow the toe to lie freely in a fully corrected, neutral position without any springing back or residual tension.
- Closure: The design of the double racquet incision allows the dorsal skin defect to close in a V-Y fashion, accommodating the new plantarflexed position of the toe. Close the skin with multiple interrupted non-absorbable sutures. The plantar incision usually requires minimal suturing, acting as a release.
- Dressing: Apply a light, non-constricting dressing to the suture line. No rigid splint or cast is necessary, and circumferential wraps must be strictly avoided to prevent venous congestion or arterial occlusion.
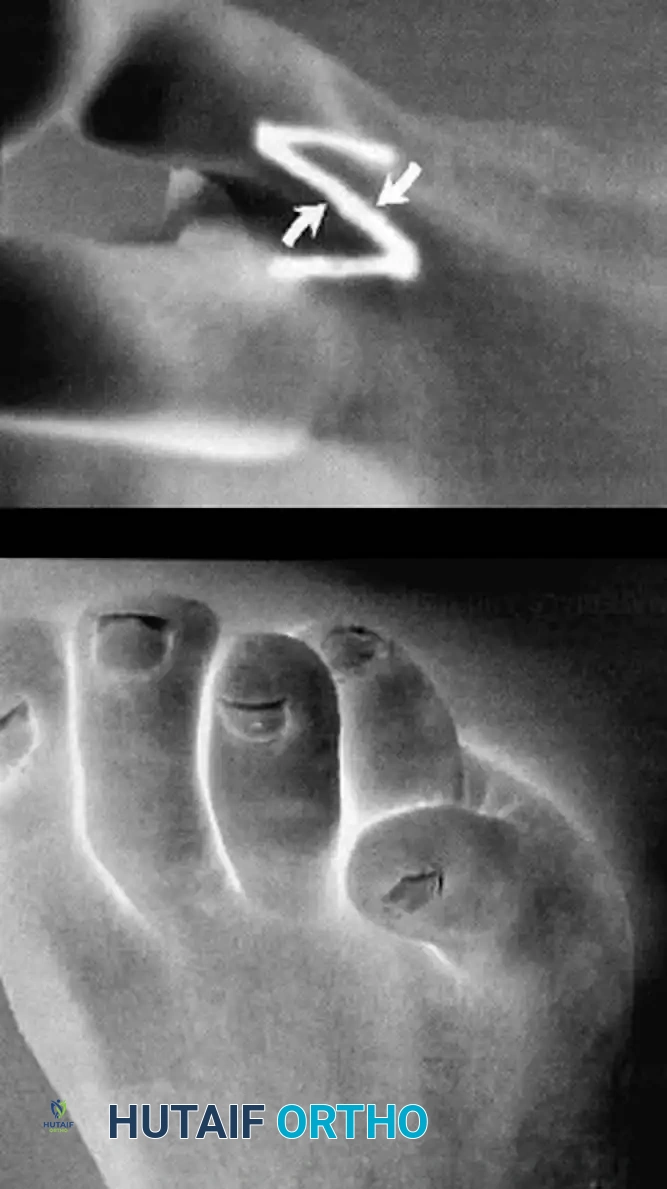
Complex Congenital Deformities: Cleft Foot Closure
While contractures of the fifth toe represent a common isolated anomaly, orthopedic surgeons must also be prepared to manage complex syndromic or structural forefoot deformities, such as the cleft foot (ectrodactyly). Cleft foot is a rare congenital anomaly characterized by the absence of one or more central rays, resulting in a deep V-shaped cleft that severely impairs both foot biomechanics and aesthetics. Wood, Peppers, and Shook described a simplified, highly effective technique for cleft foot closure that restores the transverse metatarsal arch and creates a functional, cosmetically acceptable web space.
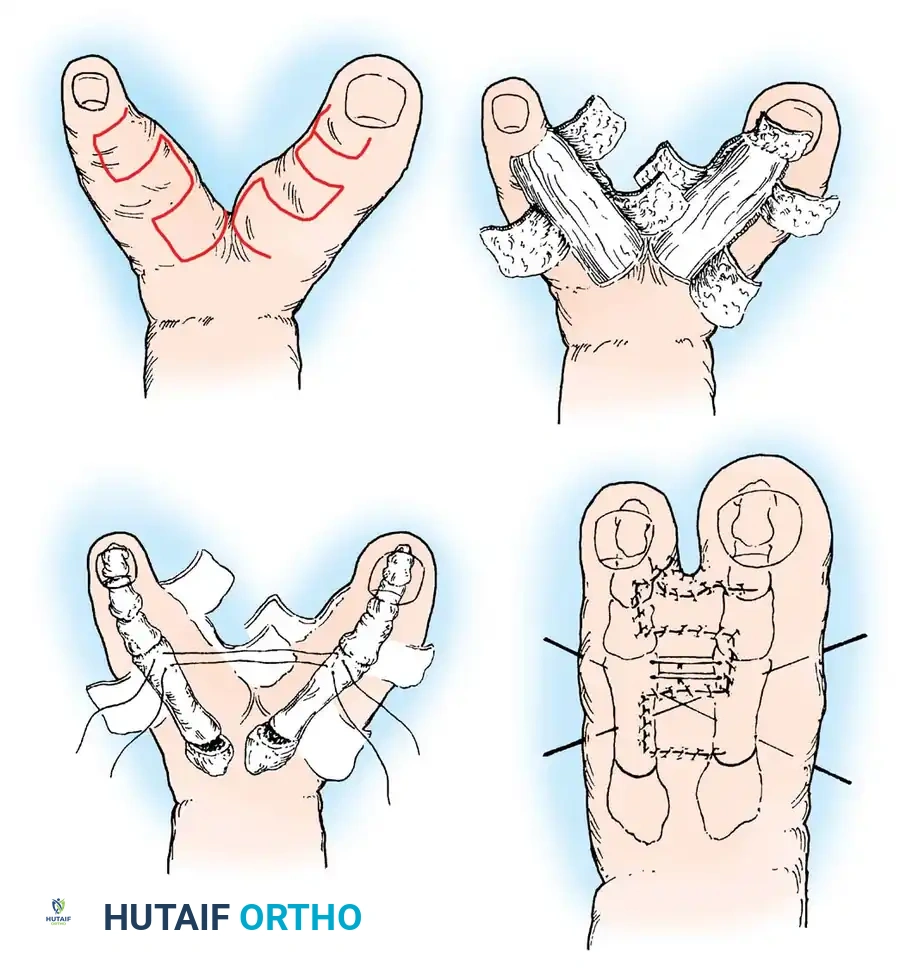
- Flap Design: Rectangular flaps are meticulously raised on the opposing surfaces of the rays bordering the cleft. The design must account for the final web space depth to prevent distal migration of the commissure (syndactylization), which can lead to functional impairment and poor cosmesis.
- Cleft Excision: The flaps are raised proximally until the skin of the entire cleft is completely removed. Care is taken to excise any rudimentary anlagen or fibrous bands within the cleft that may impede closure. At the distal tip of the longer toe bordering the cleft, a specialized flap is raised to suture to the adjacent toe, ensuring the creation of a wide, natural-appearing toe web.
- Osseous Realignment: Soft-tissue closure alone is often insufficient due to the divergent vector forces of the remaining metatarsals. If the toes spring apart upon attempted closure, a closing wedge osteotomy is made at the base of each bordering metatarsal. This centralizes the bones and narrows the forefoot. Ensure the plantar cortices of the metatarsals remain intact to act as a hinge, enhancing stability and promoting rapid primary bone healing.
- Fixation: Smooth Kirschner wires (K-wires), typically 0.045 or 0.062 inches, are inserted longitudinally across the osteotomy sites and transversely across the metatarsal heads to maintain the centralized position during osseous union and soft-tissue healing.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the operative management of fifth toe deformities carries a distinct profile of potential complications. The most feared and immediate complication is vascular compromise, colloquially known as the "white toe" phenomenon. This occurs when the digital arteries are subjected to acute longitudinal traction or vasospasm following the derotation and plantarflexion of a chronically contracted toe. The incidence of transient ischemia is relatively high, but true ischemic necrosis leading to digit loss is rare if recognized and managed promptly.
If a "white toe" is identified immediately upon tourniquet deflation, the surgeon must act decisively. The initial step is to ensure that the foot is dependent and that no constrictive dressings are present. Warm saline sponges can be applied to the forefoot to induce vasodilation, and topical papaverine or lidocaine without epinephrine may be applied directly to the neurovascular bundles if they are exposed. If the toe remains ischemic, the surgeon must systematically reverse the surgical steps: remove any K-wires that may be distracting the joint, loosen or remove the skin sutures, and allow the toe to drift back into a slightly deformed position. It is far preferable to accept a mild recurrent deformity than to suffer complete gangrene of the digit.
Recurrence of the deformity is another significant complication, particularly in pediatric patients who undergo surgery before skeletal maturity, or in adults where the capsular release was inadequate. Recurrence rates vary in the literature but can approach 10-15% in complex cases. Recurrence is typically driven by incomplete release of the plantar plate adhesions or failure to adequately lengthen the cutaneous tether in the fourth web space. Salvage management for a stiff, painful, recurrent deformity often involves a revision arthroplasty with proximal phalanx base resection (hemi-phalangectomy) or, in recalcitrant cases, syndactylization of the fifth toe to the fourth toe to provide dynamic stability.
Infection and wound dehiscence are less common but require vigilant post-operative care. Marginal flap necrosis can occur at the apical tips of a Z-plasty if the flaps are handled roughly with forceps or sutured under excessive tension. These minor wound complications generally heal by secondary intention with local wound care. Deep space infections or osteomyelitis are exceedingly rare but mandate immediate surgical debridement and targeted intravenous antibiotic therapy.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management Protocol |
|---|---|---|---|
| Vascular Compromise ("White Toe") | 2% - 5% | Avoid over-lengthening; meticulous soft-tissue handling; avoid circumferential dressings. | Remove dressings; apply warm saline/papaverine; remove K-wires; remove sutures and allow toe to relax. |
| Recurrence of Deformity | 10% - 15% | Ensure complete release of plantar plate and adequate skin lengthening (Z-plasty). | Revision capsulotomy; proximal phalangectomy; 4th-5th digit syndactylization. |
| Flap Tip Necrosis / Dehiscence | 5% - 8% | Handle skin edges with skin hooks, not toothed forceps; ensure 60-degree Z-plasty angles. | Local wound care; allow healing by secondary intention; avoid premature suture removal. |
| Nerve Injury / Neuroma | < 2% | Careful blunt dissection; use of loupe magnification during initial exposure. | Gabapentinoids; local corticosteroid injections; surgical excision of neuroma if recalcitrant. |
| Nonunion (in Cleft Foot Osteotomies) | < 5% | Maintain plantar cortical hinge; rigid K-wire fixation; strict non-weight-bearing protocol. | Prolonged immobilization; bone stimulator; revision osteotomy with bone grafting. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following the surgical correction of fifth toe contractures is meticulously designed to protect the fragile soft-tissue reconstruction, maintain the newly acquired alignment, and prevent any extrinsic forces that could compromise digital perfusion. The rehabilitation process is generally divided into three distinct phases: immediate post-operative, intermediate healing, and long-term maintenance.
Phase 1: Immediate Post-Operative Care (Weeks 0-2)
Immediately following the procedure, the foot is placed in a bulky, non-constrictive soft dressing. A short leg cast or a rigid post-operative surgical shoe is applied to protect the forefoot from accidental trauma. For isolated fifth toe procedures, such as the Z-plasty or Butler arthroplasty, it is absolutely critical that only a light, non-adherent dressing (such as Adaptic or Xeroform) is placed over the digit itself. Circumferential taping or rigid toe splints are strictly forbidden during this initial phase, as post-operative edema combined with a rigid splint will inevitably lead to venous congestion and potential arterial occlusion. The patient is instructed to maintain strict elevation of the extremity above the level of the heart for the first 48 to 72 hours to minimize swelling. Weight-bearing status is generally restricted to heel-weight-bearing only, utilizing crutches or a walker.
Phase 2: Intermediate Healing and Suture Removal (Weeks 2-6)
At the 10 to 14-day mark, the patient returns to the clinic for the first post-operative wound check. Capillary refill, toe turgor, and the integrity of the skin flaps are assessed. If the incisions are entirely healed and there is no tension across the wound edges, the non-absorbable skin sutures are removed. In cases of Z-plasty where the apical tips appear tenuous, suture removal may be delayed until 21 days. Once the sutures are removed, the patient is transitioned to protected weight-bearing as tolerated in a hard-soled surgical shoe. At this stage, gentle buddy taping of the fifth toe to the fourth toe may be initiated to maintain the corrected alignment and prevent the toe from drifting back into varus and dorsiflexion. For patients who underwent complex cleft foot closure with metatarsal osteotomies, strict non-weight-bearing status must be maintained for a minimum of 4 to 6 weeks, and K-wires are typically removed in the clinic between weeks 4 and 6 once radiographic evidence of early bone healing is observed.
Phase 3: Long-Term Maintenance and Return to Activity (Weeks 6 and beyond)
As the soft tissues mature and post-operative edema completely resolves—a process that can take up to 3 to 6 months—the patient is gradually transitioned out of the surgical shoe and into standard footwear. The most critical long-term instruction is the mandatory use of wide-toe-box footwear. Shoes with narrow, constricting toe boxes will place extrinsic pressure on the lateral aspect of the fifth toe, risking not only recurrent pain and heloma formation but also actual structural recurrence of the deformity. Patients are educated on scar massage techniques to prevent hypertrophic scarring, particularly over the dorsal aspect of the Z-plasty. Routine follow-up at 3 months, 6 months, and 1 year is recommended to monitor for any signs of residual rotational malalignment or stiffness at the MTP joint.
Summary of Landmark Literature and Clinical Guidelines
The evolution of operative techniques for the overriding fifth toe is well-documented in the orthopedic literature, with several landmark studies forming the basis of current clinical guidelines. The shift from aggressive osseous resections to joint-preserving soft-tissue realignments has been driven by a better understanding of the condition's pathoanatomy.
Thordarson's seminal
