Introduction to Shoulder Instability
The successful treatment of shoulder instability is fundamentally predicated upon a thorough, nuanced understanding of the various posttraumatic and developmental lesions that compromise the glenohumeral joint. The shoulder, possessing the greatest range of motion of any joint in the human body, relies on a delicate interplay between static stabilizers (the capsulolabral complex, glenohumeral ligaments, and articular congruity) and dynamic stabilizers (the rotator cuff and periscapular musculature). When this equilibrium is disrupted, instability ensues, ranging from subtle subluxation to catastrophic, recurrent dislocation.
This comprehensive guide delineates the critical classification systems of shoulder instability, explores the biomechanical implications of age and tissue quality, and provides a masterclass on the surgical decision-making and operative techniques required to restore glenohumeral stability.
Pathoanatomy and Biomechanics
Mechanisms of Failure
Instability should be conceptualized along a spectrum of tissue failure. The capsuloligamentous complex can fail via catastrophic avulsion (e.g., a classic Bankart lesion) or through insidious plastic deformation.
Clinical Pearl: Plastic deformation occurs when a ligament is stretched beyond its yield point but before its ultimate failure point. In chronic instability, the capsule is often plastically deformed, necessitating capsular plication or shifting during surgical repair, even if a discrete labral tear is repaired.
Secondary trauma to the rotator cuff and the long head of the biceps tendon may cause asynchronous rotator cuff function, further destabilizing the joint by disrupting concavity compression—the primary dynamic stabilizing mechanism of the glenohumeral joint.
Classification Systems of Shoulder Instability
Etiological Classification: Macrotraumatic, Microtraumatic, and Atraumatic
Macrotraumatic Instability
This category involves a single, identifiable traumatic event of sufficient magnitude to result in a frank dislocation. The classic lesion is the avulsion of the anterior-inferior labrum and capsule from the glenoid rim.
Microtraumatic (Acquired) Instability
Microtraumatic instability arises from repetitive trauma at the extremes of motion, resulting in the gradual plastic deformation of the capsulolabral complex.
* Demographics: These injuries most commonly occur in overhead athletes, including baseball pitchers, batters, gymnasts, weightlifters, tennis players, and swimmers (especially those utilizing the backstroke or butterfly stroke).
* Pathogenesis: The extreme flexibility that allows an athlete to compete at an elite level is often attributed to generalized ligamentous laxity. While advantageous for performance, this laxity predisposes the athlete to injury. Over time, repetitive microtrauma causes decompensation of a previously stable capsuloligamentous complex.
Atraumatic Instability
Atraumatic instability occurs without a discrete traumatic event and is typically associated with generalized ligamentous laxity, connective tissue disorders, or glenohumeral dysplasia.
Matsen’s Classification System
Matsen’s simplified classification system remains a highly useful heuristic for categorizing instability patterns and guiding treatment:
- TUBS: Traumatic etiology, Unidirectional instability, Bankart lesion present, Surgery is typically required.
- AMBRII: Atraumatic etiology, Multidirectional instability, Bilateral findings (often), Rehabilitation is the first line of treatment, Inferior capsular shift is the surgical procedure of choice if conservative measures fail, and Internal closure (repair of the rotator interval) is often necessary.
Surgical Warning: Microtraumatic or developmental lesions frequently fall between the extremes of macrotraumatic (TUBS) and atraumatic (AMBRII) lesions. A rigid adherence to these acronyms without considering the overlapping spectrum of pathology can lead to surgical failure.
Age-Related Pathological Variations
Age is a critical prognosticator in predicting pathological lesions, recurrence rates, and ultimate clinical outcomes.
The Adolescent and Young Adult (<20 Years Old)
Recurrence rates of more than 90% are reported in patients younger than 20 years old following a primary dislocation. In several studies, the recurrence rate for adolescents treated with surgical stabilization was higher than that for patients in other age groups.
* Biomechanical Rationale: These differences are explained by the greater elasticity in adolescent ligaments, which results in greater plastic deformation before the ultimate failure of the system. This profound deformation must be addressed during surgical treatment; simply repairing the labrum without addressing capsular laxity will result in recurrent instability.
The Older Adult (>40 Years Old)
Conversely, the recurrence rate of dislocation is about 10% in patients older than 40 years old. However, the energy of the dislocation is transferred to other structures.
* Rotator Cuff Tears: Associated rotator cuff tears are present in over 30% of patients older than 40, and this incidence skyrockets to more than 80% in patients older than 60 years old.
* Fractures: Fractures of the greater tuberosity are highly prevalent in patients older than 40 years old, with some series reporting an incidence of 42%.
* Treatment Hierarchy: In this older age group, the surgical treatment of rotator cuff tears or fractures of the greater tuberosity generally takes precedence over the treatment of the capsular injury.
Special Populations and Considerations
Voluntary Dislocators and Psychological Factors
The mental set of the patient must be rigorously evaluated before treatment is initiated. Some patients with posterior or multidirectional instability learn to dislocate their shoulder through selective, asynchronous muscular contractions.
* Management: Although voluntary dislocation does not inherently indicate a pathological overlay, some patients utilize voluntary dislocation for secondary gain. In these specific patients, surgical treatment is absolutely doomed to failure and is contraindicated.
Neuromuscular and Collagen Disorders
In patients with primary neuromuscular disorders or syndromes presenting with recurrent dislocation, conservative, nonoperative treatment should be the initial approach.
* Collagen Disorders: Patients with primary collagen disorders, such as Ehlers-Danlos syndrome or Marfan syndrome, should be treated with extensive, supervised conservative rehabilitation.
* Surgical Caveat: If surgical intervention becomes strictly necessary, the high probability of the abnormal, dysplastic tissue stretching out and allowing the dislocation to recur must be explicitly stressed to the patient and their family during the informed consent process.
Evaluation of Bony Defects
When severe dysplastic or traumatic glenohumeral deformity is present, soft-tissue procedures alone are insufficient. Capsular and bony procedures become necessary. The evaluation of critical bone loss is paramount. Reformatted 3-Dimensional Computed Tomography (3D CT) images are highly beneficial in determining the need for osteotomy or bone grafting procedures.
Radiographic Assessment of Bone Loss
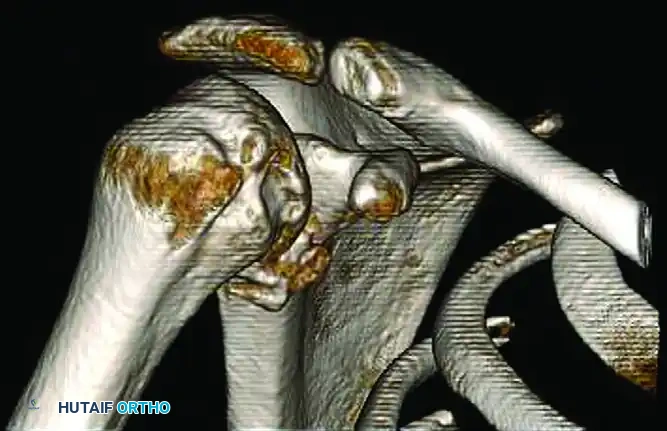
FIGURE 47-25 A: Three-dimensional CT showing a large, engaging Hill-Sachs lesion on the posterolateral humeral head and a deficient anterior glenoid rim. The presence of bipolar bone loss significantly increases the risk of recurrent instability if treated with soft-tissue repair alone.
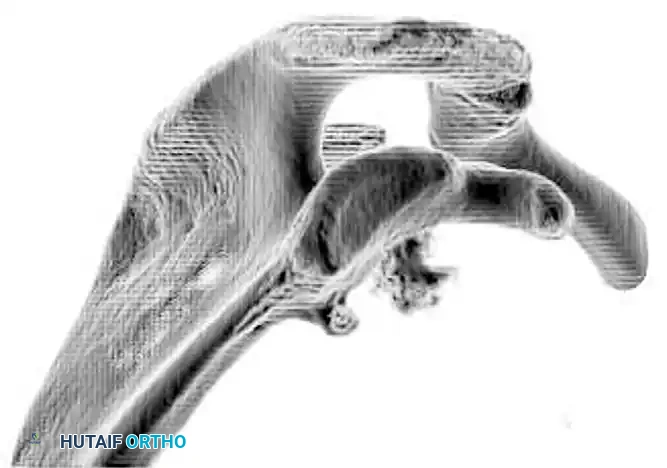
FIGURE 47-25 B: Three-dimensional CT with the humeral head digitally subtracted, providing an en face view of the glenoid. This clearly demonstrates the loss of the anterior glenoid surface (the "inverted pear" appearance), quantifying the defect which dictates the necessity for a bony augmentation procedure such as the Latarjet.
Clinical Pearl: The concept of the "glenoid track" is essential here. If a Hill-Sachs lesion engages the anterior glenoid rim during abduction and external rotation (an "off-track" lesion), a Bankart repair alone will fail. Bony augmentation of the glenoid (Latarjet) or filling the humeral defect (Remplissage) is required.
Surgical Indications and Positioning
Indications for Surgery
- TUBS: Recurrent traumatic anterior dislocations, especially in young, active patients (<25 years old) where the natural history dictates a >90% recurrence rate.
- Bony Lesions: Anterior glenoid bone loss >15-20%, or an off-track Hill-Sachs lesion.
- AMBRII: Failure of a prolonged (6+ months) dedicated physical therapy program focusing on periscapular and rotator cuff strengthening.
- Concomitant Pathology: Acute dislocation in a patient >40 years old with a massive, acute rotator cuff tear.
Patient Positioning
- Lateral Decubitus: Preferred by many for arthroscopic Bankart repairs. The arm is placed in 45 degrees of abduction and 15 degrees of forward flexion with 10-15 lbs of longitudinal traction. This provides excellent visualization of the inferior recess and facilitates capsular shifting.
- Beach Chair: Preferred for open procedures (Latarjet, open capsular shifts) and arthroscopic procedures where concomitant rotator cuff repair is anticipated. The patient is seated at 45-60 degrees. Ensure the head is securely stabilized and the operative arm is completely free for manipulation.
Step-by-Step Surgical Approaches
1. Arthroscopic Bankart Repair and Capsular Plication (For TUBS)
Step 1: Diagnostic Arthroscopy and Portal Placement
Establish a standard posterior viewing portal. Create an anterior-inferior (5 o'clock) portal just superior to the subscapularis tendon, and an anterior-superior (1 o'clock) portal at the rotator interval. Use a cannula in the anterior-inferior portal for anchor placement and suture management.
Step 2: Mobilization of the Capsulolabral Complex
This is the most critical step. Use an arthroscopic elevator and electrocautery to release the scarred labrum and capsule from the anterior glenoid neck. The release must extend inferiorly to the 6 o'clock position. A successful release is confirmed when the subscapularis muscle belly can be visualized beneath the mobilized capsule.
Step 3: Glenoid Preparation
Decorticate the anterior glenoid rim using a motorized burr or rasp to create a bleeding bone bed, which is essential for biological healing of the labrum.
Step 4: Anchor Placement and Suture Passing
Place the first suture anchor at the 5:30 position on the glenoid face, precisely at the articular margin. Pass the suture through the capsule and labrum inferior and lateral to the anchor to achieve an inferior-to-superior and lateral-to-medial capsular shift.
Step 5: Knot Tying and Superior Progression
Tie the sutures using a sliding-locking knot followed by alternating half-hitches. Proceed superiorly, placing subsequent anchors at the 4 o'clock and 2:30 positions, sequentially shifting the capsule superiorly to eliminate the plastic deformation and restore the anterior bumper.
2. The Latarjet Procedure (For Critical Bone Loss)
When 3D CT (as seen in Figures 47-25 A and B) demonstrates >15-20% glenoid bone loss, the Latarjet procedure is indicated.
Step 1: Approach and Coracoid Exposure
Utilize a standard deltopectoral approach. Identify the cephalic vein and retract it laterally with the deltoid. Expose the coracoid process and the attached conjoint tendon (short head of biceps and coracobrachialis).
Step 2: Coracoid Osteotomy and Preparation
Release the coracoacromial ligament, leaving a 1 cm stump for later repair to the capsule. Release the pectoralis minor from the medial aspect of the coracoid. Perform an osteotomy at the base of the coracoid using an oscillating saw. Decorticate the inferior surface of the coracoid to flat, bleeding bone. Drill two holes through the coracoid for subsequent screw fixation.
Step 3: Subscapularis Split and Glenoid Exposure
Perform a horizontal split in the subscapularis tendon at the junction of the middle and inferior thirds. Expose the anterior shoulder capsule, perform a vertical capsulotomy, and expose the anterior glenoid. Prepare the anterior glenoid neck with a burr to create a flat, bleeding surface that perfectly matches the prepared coracoid.
Step 4: Graft Fixation
Pass the coracoid graft through the subscapularis split. Position it flush with the articular cartilage of the anterior glenoid (avoiding lateral overhang, which causes rapid osteoarthritis). Secure the graft using two 3.75mm or 4.0mm partially threaded cannulated screws.
Step 5: Capsular Repair
Repair the native capsule to the stump of the coracoacromial ligament left on the graft. This creates an extra-articular position for the bone graft and provides an additional soft-tissue restraint.
Biomechanical Pearl: The Latarjet provides a "triple effect" of stability: 1) The bone graft restores the glenoid articular arc; 2) The conjoint tendon acts as a dynamic sling across the anterior-inferior capsule when the arm is abducted and externally rotated; 3) The capsular repair to the CA ligament stump restores the static capsular restraint.
Postoperative Rehabilitation Protocols
Rehabilitation must be meticulously tailored to the specific procedure performed and the patient's inherent tissue quality.
Phase I: Protection (Weeks 0-4)
- Immobilization: The shoulder is immobilized in a sling. For Bankart repairs, neutral rotation is preferred.
- Motion: Passive range of motion (PROM) is initiated early to prevent stiffness, but external rotation is strictly limited to 0-10 degrees to protect the anterior repair. Forward flexion is limited to 90 degrees.
- Exercises: Grip strengthening, wrist/elbow ROM, and scapular retractions.
Phase II: Intermediate Motion (Weeks 4-8)
- Sling Weaning: Discontinue the sling at 4-6 weeks.
- Motion: Progress to active-assisted range of motion (AAROM) and then active range of motion (AROM). Gradually increase external rotation by 10 degrees per week.
- Strengthening: Initiate submaximal isometric strengthening for the rotator cuff and deltoid.
Phase III: Strengthening (Weeks 8-12)
- Motion: Achieve full, symmetric AROM.
- Strengthening: Progress to isotonic strengthening using resistance bands and light weights. Focus heavily on periscapular stabilizers (rhomboids, trapezius, serratus anterior) and dynamic concavity compression via the rotator cuff.
Phase IV: Return to Play (Months 3-6+)
- Advanced Strengthening: Plyometrics, proprioceptive neuromuscular facilitation (PNF), and sport-specific drills.
- Clearance: Return to contact sports or heavy overhead labor is typically permitted between 5 to 6 months postoperatively, provided the patient has full, painless ROM, normal scapulothoracic kinematics, and isokinetic strength >90% of the contralateral shoulder. Patients with Latarjet procedures must have radiographic evidence of complete graft union before returning to contact sports.
