Introduction to Tibial and Fibular Shaft Malunions
The management of malunions of the shafts of the tibia and fibula remains a complex challenge in operative orthopedics. While the precise degree of deformity that mandates surgical intervention is not universally defined, it is a fundamental biomechanical principle that angular deformities of the tibial shaft cause significant alterations in the contact pressures of the knee and ankle joints. Over time, these altered kinematics predispose the patient to the development of secondary osteoarthritis (OA).
However, clinical series with long-term follow-up have presented a nuanced view of this hypothesis. Merchant and Dietz found no direct correlation between the degree of angular deformity and functional outcome in long-term follow-ups of tibial shaft fractures, though their study did not stratify by the specific site of the deformity. Conversely, mathematical analyses and clinical series by Puno et al. demonstrated that angular deformity of the tibia affects the ankle joint more profoundly than the knee joint, emphasizing that the location of the fracture is highly significant. Poorer functional ankle scores strongly correlate with the degree of malalignment and the proximity of the deformity to the ankle joint.
Clinical Pearl: Varus deformities of the tibial shaft are generally more poorly tolerated than valgus deformities, leading to a higher incidence of medial compartment osteoarthritis of the knee and accelerated degenerative changes in the ankle.
Biomechanics and the Risk of Osteoarthritis
The relationship between malalignment and osteoarthritis has been extensively studied. Milner et al. evaluated patients 30 years post-tibial shaft fracture, noting that while fracture malunion did not universally cause a higher incidence of ipsilateral ankle and subtalar arthritis, there was a distinct trend toward medial compartment knee osteoarthritis in patients with varus malalignment. Furthermore, shortening of 10 mm or more correlated strongly with subjective complaints of knee pain.
van der Schoot et al. evaluated the influence of malalignment on radiographic osteoarthritic changes in 88 patients followed for an average of 15 years. The incidence of osteoarthritic changes was significantly higher in the fractured leg (36% ankle arthritis, 19% knee arthritis) compared to the uninjured leg (6% ankle arthritis, 3% knee arthritis). Fractures that healed with an angular deformity of 5 degrees or more were associated with a higher incidence of arthritic changes (58%) than those with lesser deformity (31%). Interestingly, rotational deformity was not independently associated with arthritic changes in this cohort.
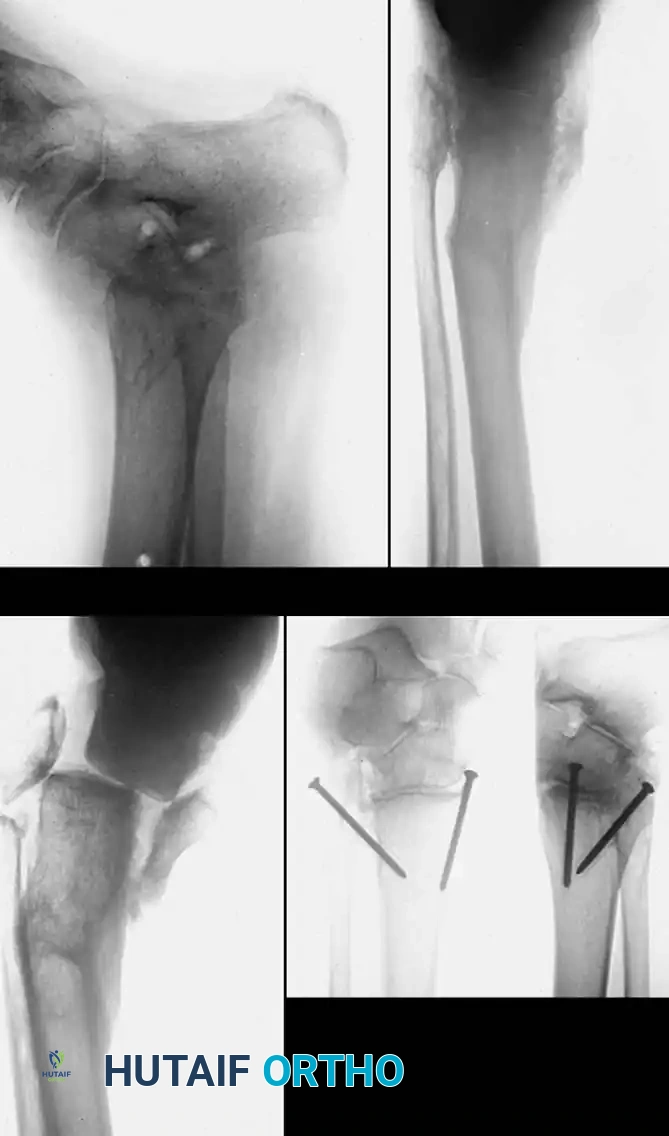
Fig. 1: (A) Malunion of a bimalleolar ankle fracture with preexisting malunion of the distal tibia. (B) Correction achieved; however, arthritis developed. (C and D) Tibiotalar arthrodesis performed using compression clamps, resulting in a painless, stable ankle.
Indications for Surgical Correction
When considering surgery for a tibial malunion, the surgeon must synthesize the degree of deformity, the patient’s symptoms, the condition of the soft-tissue envelope, and the patient's functional demands. Disability is primarily produced by rotational deformity, lateral and posterior bowing, and shortening.
The degree of "acceptable" deformity varies among authorities, but general consensus guidelines suggest surgical correction is indicated for:
* Valgus deformity: > 12 degrees
* Varus deformity: > 6 degrees
* External rotation deformity: > 15 to 20 degrees
* Internal rotation deformity: > 10 to 15 degrees
* Shortening: > 2.0 to 2.5 cm (Shortening ≤ 2 cm is usually well-tolerated with shoe modifications, but > 2.5 cm causes significant gait disability and pelvic obliquity).
Symptoms warranting intervention include intractable ankle, knee, or back pain; severe gait disturbances; and cosmetically unacceptable deformities. Often, a resulting contracture of the Achilles tendon causes an equinus deformity of the foot, which must be addressed concurrently.
Preoperative Evaluation and Planning
A meticulous preoperative evaluation is mandatory. The limb must be assessed for a history of neurological or vascular injury, the adequacy of soft-tissue coverage, and any history of infection.
Soft Tissue and Vascular Assessment
If there is a history of vascular injury, preoperative arteriography or CT angiography is essential to determine the safety of the operative approach. In cases where the soft tissues over the planned osteotomy site are compromised, a simultaneous local rotation flap or a vascularized free tissue transfer may be required to ensure adequate coverage, promote bone healing, and prevent catastrophic wound complications.
Infection Workup
In patients with a history of open fractures or previous osteomyelitis, latent infection must be ruled out. Preoperative indium-labeled white blood cell scans, gallium scans, or technetium bone scans are valuable adjuncts to determine the activity of any residual infection. It is an absolute prerequisite to eradicate active infection before performing a corrective osteotomy for malunion.
Mathematical Modeling of the Deformity
Preoperative planning requires precise determination of the angular deformity, rotational malalignment, leg-length discrepancy, and translation.
Angular deformities in the frontal (varus-valgus) and sagittal (flexion-extension) planes can be mathematically resolved into a single uniplanar deformity in an oblique plane. The degree of maximal deformity is always greater than the angular measurements seen on standard orthogonal anteroposterior (AP) or lateral radiographs.
Surgical Technique Tip: The plane of maximal deformity can be identified intraoperatively by rotating the leg under fluoroscopy until the maximal degree of angulation is visualized. A radiograph taken at exactly 90 degrees to this plane will show zero angular deformity. The corrective oblique osteotomy must be made perpendicular to this plane of maximal deformity.
Rotational deformity is best evaluated with a computed tomography (CT) scan measuring the tibial torsion angle, or clinically by measuring the transmalleolar axis relative to the tibial tubercle. Sangeorzan et al. developed a highly effective mathematical model for planning oblique osteotomies that simultaneously correct angular and rotational deformities while allowing for axial lengthening.

Fig. 2: Preoperative templating and mathematical modeling of a multiplanar tibial deformity, identifying the plane of maximal angulation.
Surgical Strategies and Osteotomy Design
Simple opening wedge, closing wedge, or dome-shaped osteotomies are effective for relatively small degrees of uniplanar malunion. However, closing wedge osteotomies inherently create additional limb shortening, and opening wedge osteotomies require structural bone grafting and carry a higher risk of delayed union.
Supramalleolar Osteotomy
Although osteotomies are typically performed at the apex of the deformity (often the old fracture site), a supramalleolar osteotomy may be preferable if the previous fracture site is covered with poor soft tissue, contains extremely dense avascular sclerotic bone, or has a history of recalcitrant nonunion.
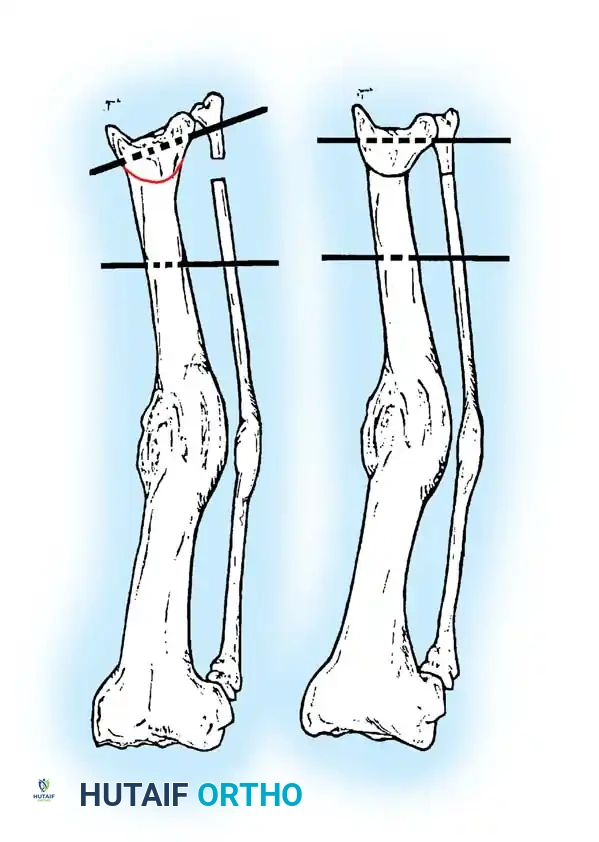
Fig. 3: Supramalleolar dome osteotomy. (A) Dome osteotomy created 1 to 1.5 cm proximal to the ankle joint. Threaded pins are inserted parallel to the ankle and knee joint lines. (B) Osteotomy completed, and pins brought parallel to correct varus or valgus deformity.
Oblique Osteotomy for Multiplanar Deformities
Oblique osteotomies are the gold standard for correcting complex, multiplanar deformities. They provide a broad, vascularized surface area for bone healing. Furthermore, limb lengthening can be achieved simultaneously by sliding the distal fragment along the oblique osteotomy plane.

Fig. 4: Visualization of a multiplanar deformity requiring an oblique osteotomy cut to simultaneously correct coronal and sagittal malalignment.
Fixation Options
Satisfactory alignment after osteotomy is difficult to maintain without rigid internal or external fixation. The choice of fixation depends on the soft tissue envelope, the location of the osteotomy, and the surgeon's preference.
Intramedullary Nailing
Reamed, locked intramedullary (IM) nailing is highly recommended for diaphyseal osteotomies. Kempf, Grosse, and Abalo reported excellent union rates using dynamically locked nails, though statically locked nails are generally preferred initially to maximize rotational stability.
Contraindications to IM Nailing:
1. Extensive soft-tissue stripping required for deformity correction (reaming further devascularizes the bone).
2. History of previous external fixation with documented pin-tract infections (high risk of deep medullary sepsis).
Plate and Screw Fixation
Oblique tibial osteotomies stabilized with dynamic compression plates and lag screws provide rigid fixation and allow for precise correction of multiplanar deformities. E.E. Johnson and Sanders et al. have demonstrated excellent functional results using this technique, achieving simultaneous correction of angulation, rotation, and length.
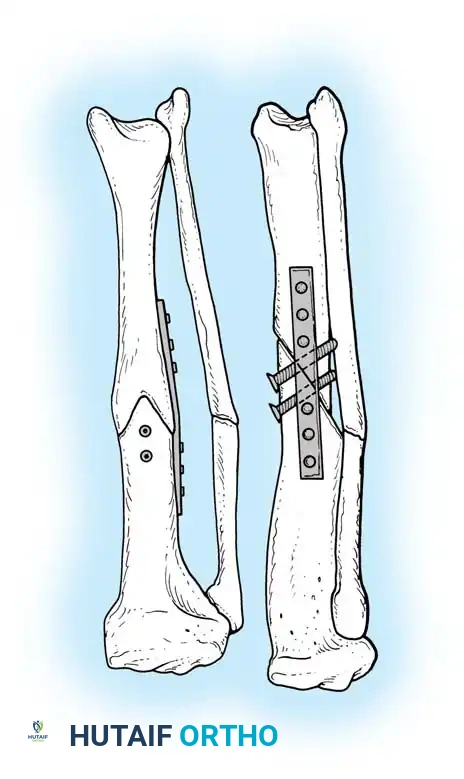
Fig. 5: Application of a dynamic compression plate following an oblique osteotomy.
External Fixation
For infected tibial malunions, or those associated with a severely compromised soft-tissue envelope, external fixation (such as the Ilizarov method) is the treatment of choice. This allows for a minimally invasive corticotomy and gradual correction of the deformity via distraction osteogenesis.
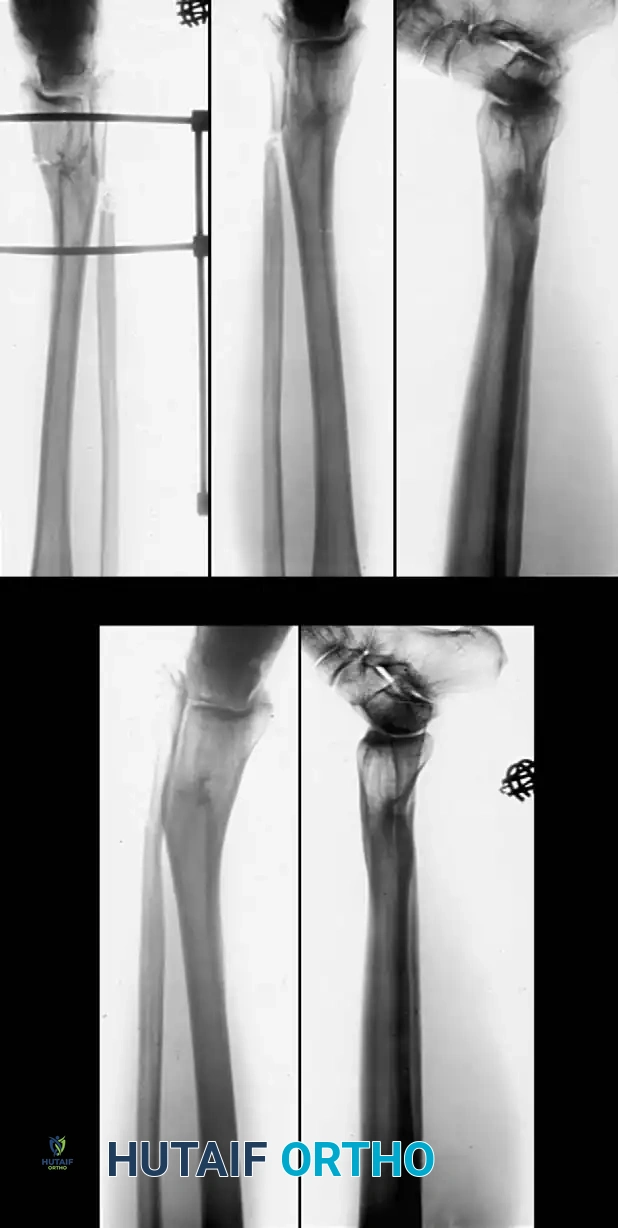
Fig. 6: (A, B) Varus malunion of the distal tibia. (C) Osteotomy of the tibia and fibula with reduction maintained by a circular external fixator. (D, E) Tibial union obtained with normal alignment.
🔪 Surgical Technique: Supramalleolar Osteotomy (Graehl, Hersh, and Heckman)
This technique is ideal for distal third malunions where the apex of deformity is near the ankle joint, or where the diaphyseal soft tissue is compromised.
- Patient Positioning: Place the patient supine on a radiolucent table. Apply a proximal thigh tourniquet.
- Fibular Osteotomy: Through a lateral longitudinal incision, expose and osteotomize the fibula to allow for mobilization of the distal tibial segment. This is critical for correcting either varus or valgus deformities.
- Tibial Exposure: Through the same lateral incision (or a separate anterior/medial incision depending on the soft tissue), expose the lateral surface of the tibia approximately 1.3 cm proximal to the ankle joint line.
- The Osteotomy: Drive a wide osteotome transversely almost entirely through the bone. Complete the fracture via manual osteoclasis to preserve the medial periosteal hinge.
- Deformity Correction: Open the osteotomy to correct the deformity. Insert cancellous iliac crest bone graft, or use a wedge-shaped structural graft taken from the proximal tibial shaft, packing it into the lateral side of the osteotomy to hold it open.
- Fixation: Stabilize the osteotomy. If using an external fixator, apply it in standard fashion with pins traversing the tibia and the talus. Alternatively, internal fixation with a contoured plate and screws can be utilized if the soft tissue permits.
- Closure: Close the wound in layers over a suction drain. Apply a bulky Jones dressing. If internal fixation was used without an external frame, apply a well-padded cast from the tibial tuberosity to the toes.

Fig. 7: Execution of the osteotomy cut, ensuring preservation of the soft tissue hinge.
🔪 Surgical Technique: Oblique Tibial Osteotomy (Sanders, Anglen, and Mark)
This technique is designed for multiplanar deformities requiring simultaneous correction of angulation, rotation, and up to 2.5 cm of lengthening.
Surgical Warning: To prevent catastrophic neurological complications during acute lengthening, somatosensory evoked potentials (SSEPs) must be monitored continuously. If SSEP signals degrade, the amount of acute lengthening must be immediately reduced.
- Preparation: Place a tourniquet on the proximal thigh. Prepare and drape both legs free so that clinical alignment, rotation, and length can be directly compared intraoperatively.
- Neuromonitoring: Place electrodes for the measurement of SSEPs, establishing a baseline before inflation of the tourniquet.
- Fluoroscopic Mapping: Under fluoroscopic control, rotate the affected leg until the plane of maximal deformity is visualized. Mark this plane on the skin.
- Fibular Osteotomy: Perform an oblique osteotomy of the fibula at a level different from the planned tibial osteotomy to prevent cross-union.
- Tibial Osteotomy: Expose the tibia via an extensile anterolateral or medial approach. Perform a single-cut oblique osteotomy perpendicular to the previously identified plane of maximal deformity. The angle of the cut typically ranges from 50 to 60 degrees relative to the mechanical axis.
- Mobilization and Lengthening: Release contracted soft tissues as necessary. If an equinus contracture is present, perform a percutaneous or open Achilles tendon lengthening. Slide the distal fragment along the oblique osteotomy plane to achieve the desired lengthening and rotational correction.
- Temporary Fixation: Provisionally hold the reduction with large reduction clamps and Kirschner wires. Verify alignment, rotation, and length clinically and fluoroscopically.
- Definitive Fixation: Apply a broad dynamic compression plate (or locking plate) to the tension side of the deformity. Secure the osteotomy with interfragmentary lag screws placed through the plate or independently outside the plate to maximize compression across the broad osteotomy surface.
- Grafting: If a significant gap exists or if lengthening exceeds 1.5 cm, pack the defect with autogenous cancellous bone graft.
- Closure: Deflate the tourniquet, achieve meticulous hemostasis, and close the soft tissues over a drain.
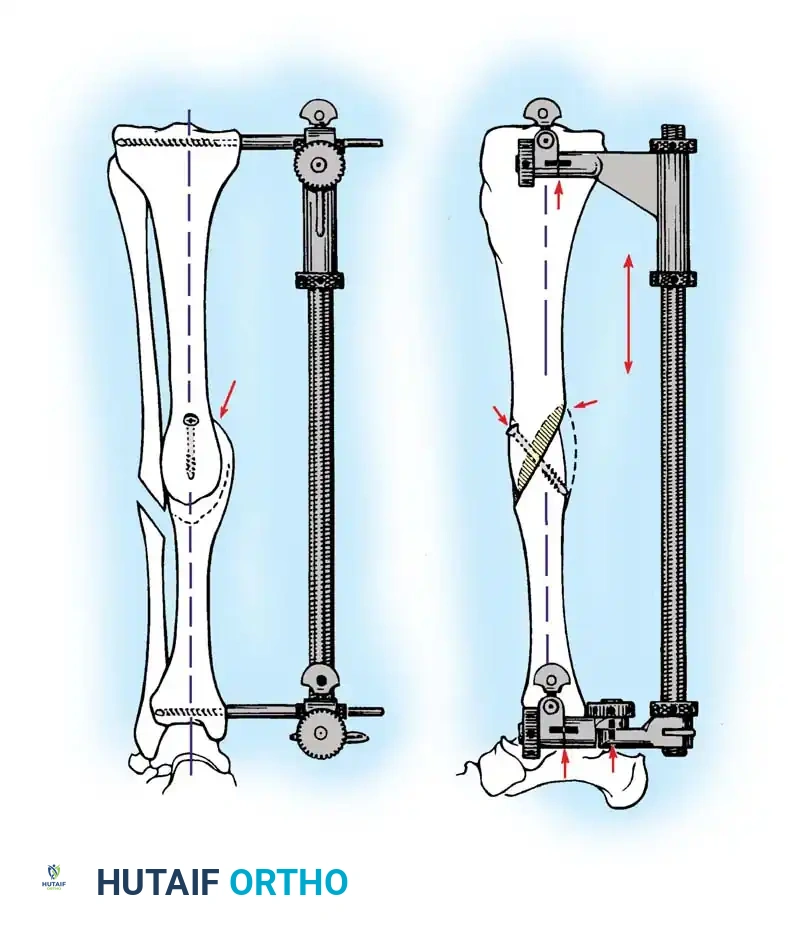
Fig. 8: Hardware placement detail showing interfragmentary lag screws securing the oblique osteotomy prior to final plate application.
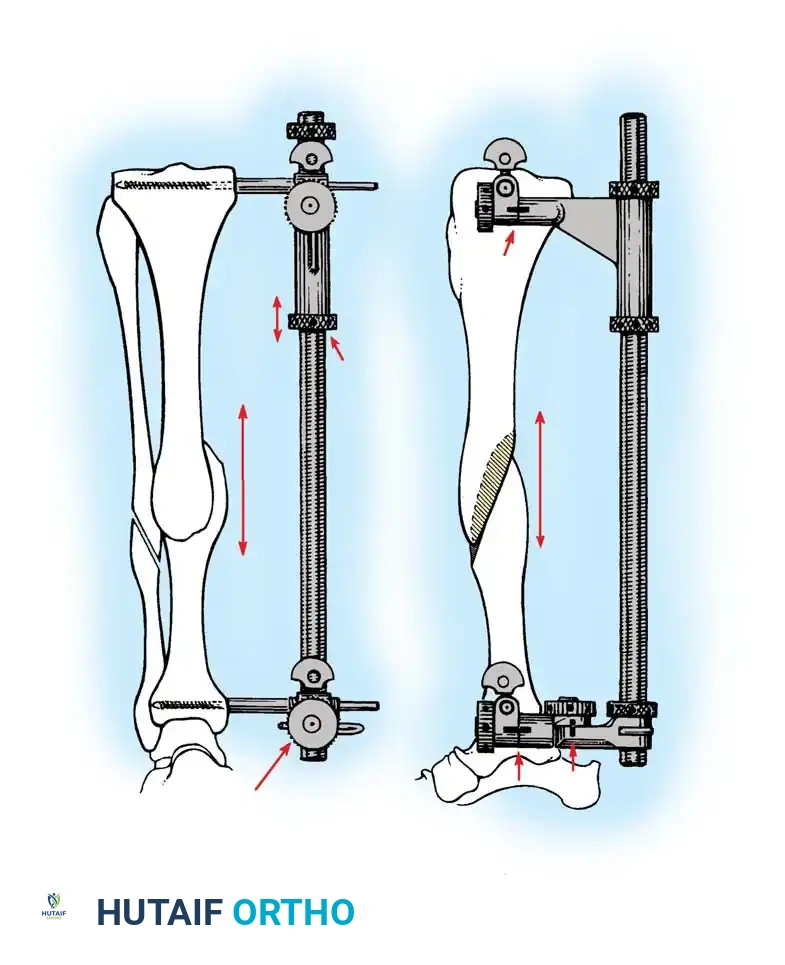
Fig. 9: Postoperative radiograph demonstrating robust callus formation and healing of the oblique osteotomy stabilized with a dynamic compression plate.

Fig. 10: Final alignment view confirming restoration of the mechanical axis in both the coronal and sagittal planes.
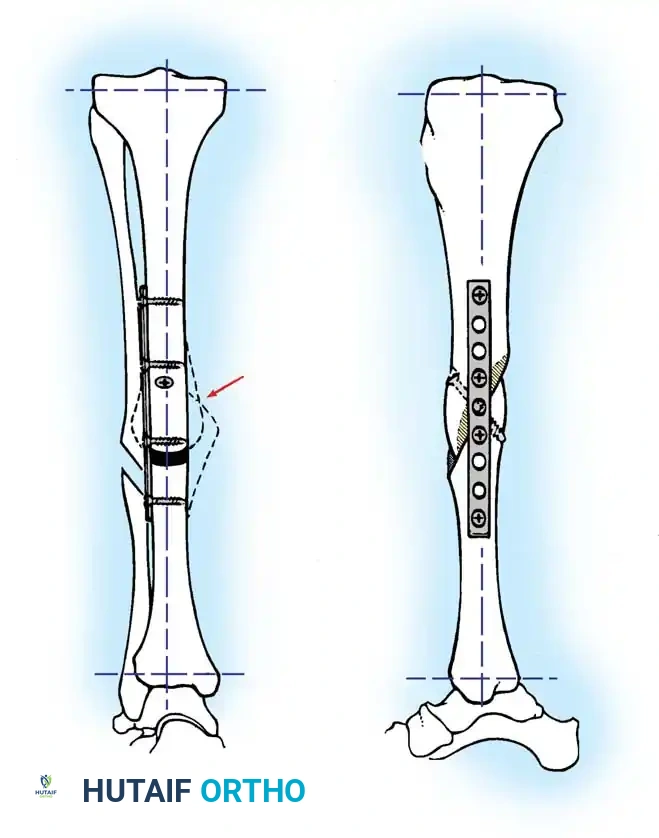
Fig. 11: Long-term follow-up demonstrating complete remodeling of the tibial shaft with maintenance of anatomical alignment and joint congruency.
Postoperative Protocol and Complications
Rehabilitation
Postoperative care is dictated by the stability of the fixation. For rigidly plated oblique osteotomies, patients are typically kept non-weight-bearing for 6 to 8 weeks. Early active and passive range of motion of the knee and ankle is initiated immediately to prevent stiffness and promote cartilage nutrition. Progressive partial weight-bearing is advanced once bridging callus is visualized on orthogonal radiographs.
Complications
- Delayed Union / Nonunion: More common in opening wedge osteotomies or when extensive periosteal stripping occurs. Treatment involves bone grafting and potentially revising the fixation.
- Infection: Deep infection requires aggressive surgical debridement, hardware removal (if stability is compromised or union is achieved), and transition to external fixation.
- Neurological Injury: Transient nerve palsies (particularly the peroneal nerve) can occur with acute lengthening > 2.5 cm or correction of severe valgus deformities. Continuous SSEP monitoring is the best preventative measure.
- Compartment Syndrome: The risk is elevated following acute correction of severe deformities. A low threshold for four-compartment fasciotomy must be maintained.
Meticulous adherence to biomechanical principles, careful soft-tissue handling, and precise preoperative mathematical modeling are the cornerstones of successful tibial and fibular malunion reconstruction.
