Introduction to Calcaneal Malunions
Pain and severe disability frequently persist following fractures of the calcaneus, even when the initial injury was managed with skillful operative or nonoperative techniques. This chronic morbidity is especially pronounced in patients whose occupations require ambulation over uneven or rough terrain. The pathoanatomy of a calcaneal malunion is complex, typically characterized by a loss of calcaneal height, increased heel width, varus deformity of the tuberosity, and profound derangement of the subtalar joint kinematics.
Deformities associated with the nonoperative management of displaced intra-articular calcaneal fractures inevitably lead to a cascade of biomechanical failures. The loss of heel height decreases the talocalcaneal angle (talar inclination), resulting in a horizontal talus. This horizontal orientation causes anterior ankle impingement, restricting dorsiflexion. Concurrently, the lateral wall blowout creates a large exostosis that impinges upon the fibula and peroneal tendons (subfibular impingement), while the depressed articular fragments lead to rapid, post-traumatic subtalar osteoarthritis.
Clinical Pearl: When evaluating a patient with a calcaneal malunion, carefully assess ankle dorsiflexion. A horizontal talus secondary to loss of calcaneal height will mechanically block the anterior distal tibia, limiting dorsiflexion to less than 10 degrees. This is a primary indication for a distraction bone-block arthrodesis rather than an in situ fusion.
Classification of Calcaneal Malunions
Surgical decision-making is heavily guided by the structural morphology of the malunion. The Stephens and Sanders CT Classification provides a prognostic framework based on the presence of lateral wall exostosis, subtalar arthritis, and hindfoot alignment.
Type I Malunion
Characterized by a large lateral wall exostosis with an intact, relatively normal subtalar joint. Patients primarily present with subfibular impingement and peroneal tendinopathy.

Type II Malunion
Characterized by a large lateral wall exostosis combined with significant post-traumatic subtalar arthritis. The hindfoot alignment remains relatively neutral.

Type III Malunion
The most severe form, characterized by a lateral exostosis, significant subtalar arthritis, and a calcaneal body malalignment of more than 10 degrees of hindfoot varus.
Guidelines for Treatment of Calcaneal Malunions (Stephens & Sanders)
- Type I: Lateral exostectomy through an extensile L-shaped lateral incision.
- Type II: Lateral exostectomy plus subtalar arthrodesis, utilizing the resected lateral wall exostosis as local autograft.
- Type III: Lateral exostectomy plus subtalar arthrodesis combined with a calcaneal osteotomy to correct the varus malalignment.
Preoperative Decision Making: In Situ vs. Bone Block Arthrodesis
The choice between an in situ subtalar arthrodesis and a bone-block distraction arthrodesis remains a topic of academic debate. Several bone-block fusion techniques designed to restore heel height and improve talar inclination have been described, historically boasting union rates of 80% to 100% with no varus malunions.
However, critical outcome studies warrant caution. Flemister et al. demonstrated that clinical outcomes were largely similar regardless of the reconstructive procedure utilized (lateral calcaneal closing wedge osteotomy, bone block arthrodesis, or in situ fusion). Crucially, they found that malunion and nonunion rates were significantly higher following bone block procedures (15%) compared to in situ fusions (5%). Consequently, in situ fusion is generally recommended unless severe anterior ankle impingement strictly dictates a more complex bone block fusion.
Surgical Warning: Trnka et al. reported an alarming 29 complications following subtalar bone block arthrodesis. Notably, four out of the five nonunions in their series occurred in patients where structural allografts were utilized. The use of bulk allograft in calcaneal malunion reconstruction is strongly cautioned against. Autologous structural graft (e.g., tricortical iliac crest) remains the gold standard.
Furthermore, smoking is a profound risk factor. High nonunion rates and residual lateral pain (present in 64% of patients) are heavily correlated with tobacco use. Rigid fixation using large-diameter (7.3 mm or 8.0 mm) titanium cannulated screws placed with a strict lag technique is mandatory to prevent implant failure.
Surgical Approaches
The Posterolateral Approach
For complex malunions requiring subtalar arthrodesis, the posterolateral approach offers distinct advantages over traditional extensile lateral or Gallie-type posterior approaches. The benefits include:
1. Minimization of soft tissue dissection and devascularization.
2. Excellent, direct visualization of the posterior facet of the subtalar joint.
3. Easier access to the medial subtalar capsule and the sustentaculum tali, facilitating medial releases necessary for deformity correction.
4. Decreased risk of iatrogenic damage to the sural nerve.
Operative Techniques
1. Subtalar Distraction Realignment Arthrodesis
Distraction arthrodesis is strictly indicated for patients with disabling pain, severe loss of heel height, and less than 10 degrees of ankle dorsiflexion due to anterior impingement.
Step 1: Exposure and Joint Preparation
Utilize a posterolateral approach. Perform a lateral exostectomy to decompress the subfibular space. The resected bone should be morselized for later use as autograft. Perform a thorough medial subtalar capsulotomy to mobilize the joint. Denude the remaining cartilage from the posterior facet down to bleeding subchondral bone.
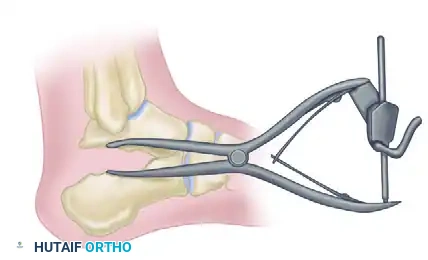
Step 2: Subtalar Distraction
Insert a lamina spreader into the posterior aspect of the subtalar joint. Carefully distract the joint to restore calcaneal height and correct the talar inclination angle.

Step 3: Structural Grafting and Fixation
Harvest a tricortical autograft (typically from the iliac crest) and shape it into a tapered wedge. Insert the anterior wedge bone graft into the distracted joint space to maintain the corrected height and alignment.
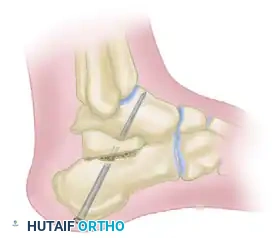
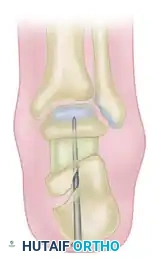
Secure the arthrodesis and the graft using large-diameter (7.3 mm or 8.0 mm) cannulated titanium screws directed from the calcaneal tuberosity into the talar dome, utilizing a lag technique for maximal compression.
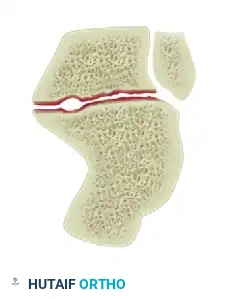
2. Reconstructive Osteotomy (Romash Technique)
Romash described a highly effective reconstructive osteotomy of the calcaneus combined with subtalar arthrodesis for severe malunions. This technique essentially re-creates the primary fracture line. By mobilizing the osteotomy, the surgeon can reposition the calcaneal tuberosity medially to narrow the heel, alleviate lateral impingement, and translate the tuberosity inferiorly to return height to the heel. The concurrent subtalar arthrodesis definitively addresses the post-traumatic arthritis.
3. The Gallie Subtalar Fusion Technique
The Gallie technique is a classic posterior approach to subtalar fusion, utilizing a mortise and tenon structural grafting concept. While less commonly used today for complex malunions requiring multi-planar correction, it remains a biomechanically sound method for in situ fusion.
Step 1: Incision and Exposure
Place the skin incision just lateral to the tendo calcaneus, extending distally toward the calcaneal tuberosity.

Step 2: Mortise Creation
Identify the posterior aspect of the subtalar joint. Using an osteotome, remove a rectangular mortise of bone spanning across the subtalar joint.

Extend this mortise deep into the joint, reaching through to the transverse sinus (sinus tarsi).

Step 3: Graft Harvest
Harvest a robust, rectangular block of cortical-cancellous bone from the anteromedial surface of the proximal tibia.

Step 4: Graft Preparation and Insertion
Prepare the tibial graft to match the dimensions of the created mortise.

Carefully impact the structural graft into the subtalar mortise. The cortical face of the graft provides immediate structural stability against shear forces.
If necessary, the graft can be divided in two to fill the medial and lateral aspects of the mortise more precisely, ensuring maximum bone-to-bone contact.

4. Triple Arthrodesis: Indications and Controversies
If the midtarsal joints (talonavicular and calcaneocuboid) are arthritic or structurally involved in the malunion, a triple arthrodesis is advisable.
For a severe crushing fracture of the calcaneus—whether fresh or malunited—triple arthrodesis has historically been recommended. In these catastrophic injuries, there is not only complete derangement of the subtalar joint but also subluxation of the calcaneocuboid and talonavicular joints caused by the severe depression of the sustentaculum tali.
Biomechanical Principle: With subtalar fusion alone in the presence of a depressed sustentaculum tali, the head and neck of the talus are left projecting forward without medial support. This creates a constant, pathologic lever arm during weight-bearing that places immense stress on the midfoot and actively interferes with subtalar fusion consolidation.
According to Conn, triple arthrodesis is preferable to isolated subtalar fusion in these severe cases because the talonavicular, calcaneocuboid, and subtalar joints function with a reciprocal, coupled action. Fusing all three does not significantly add to the patient's clinical disability, as little functional midtarsal motion remains after the original crushing injury.
However, modern orthopedic consensus dictates a more joint-preserving approach. Many surgeons believe that triple arthrodesis offers no functional advantage in the majority of patients with standard calcaneal malunions. Current Recommendation: Unless the midtarsal joints are overtly arthritic or structurally compromised by the malunion, arthrodesis should be strictly limited to the subtalar joint. Motion in the midtarsal joints may actually increase compensatorily with activity post-fusion and should be meticulously preserved whenever possible.
Postoperative Protocol and Rehabilitation
Successful consolidation of a subtalar or triple arthrodesis requires strict adherence to postoperative immobilization protocols.
1. Phase I (0-2 Weeks): The patient is placed in a bulky, non-weight-bearing (NWB) posterior splint. Elevation is critical to manage hindfoot edema and protect the surgical incision.
2. Phase II (2-6 Weeks): Sutures are removed. The patient is transitioned to a short-leg cast, remaining strictly NWB.
3. Phase III (6-10 Weeks): Radiographs are obtained to assess early trabecular bridging. If progressing well, the patient is transitioned to a CAM boot and may begin progressive partial weight-bearing (PWB). Active range of motion (AROM) of the ankle and midfoot (if unfused) is initiated.
4. Phase IV (10+ Weeks): Transition to full weight-bearing in supportive footwear. Physical therapy focuses on proprioception, peroneal strengthening, and gait normalization. Maximal medical improvement is typically reached between 9 and 12 months postoperatively.
