Mastering Orthopedic Basic Science: FRCS Exam MCQ Engine & Revision
Key Takeaway
Preparing for FRCS Orthopedic Basic Science involves mastering core concepts through targeted practice. Our interactive MCQ engine provides exam-style questions covering fracture healing, biomechanics, anatomy, and physiology. Detailed explanations accompany each question, identifying critical factors like interfragmentary strain in fracture repair, crucial for deep understanding and effective revision towards exam success.
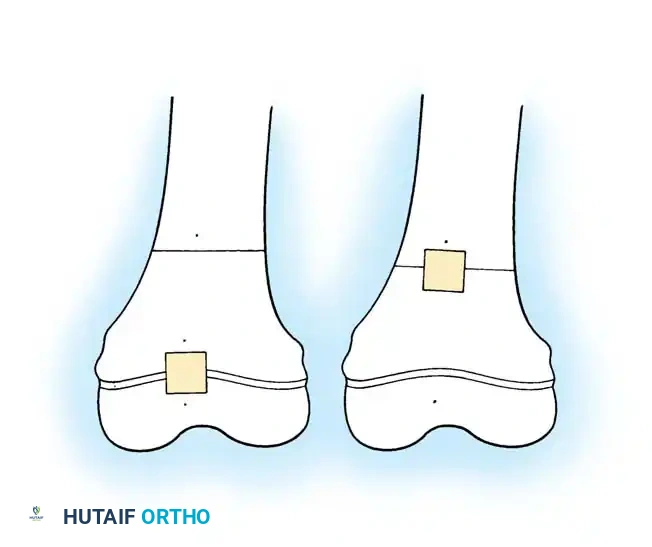
A 4-year-old child presents with a painless, bony prominence around the distal femur. The plain radiograph is shown below. Describe your findings and outline the management principles.
Candidate: The image shows a pedunculated bony exostosis arising from the metaphysis of the distal femur, pointing away from the physis. This is classic for an osteochondroma. I would evaluate for pain, mechanical symptoms, or neurovascular compromise. Management is typically observation unless there are symptoms or suspicion of malignant transformation.
Failing to mention the "danger signs" of malignant transformation (such as a thick cartilage cap >2cm in an adult, new pain in a previously quiescent lesion, or growth after skeletal maturity). Candidates often forget to enquire about family history (Hereditary Multiple Exostoses) or fail to describe the radiographic relationship between the medullary canal of the lesion and the host bone.
A structured response is essential: 1. Description: Pedunculated bony projection, corticomedullary continuity with the host bone, apex pointing away from the physis. 2. Diagnosis: Solitary Osteochondroma. 3. Assessment: Rule out Hereditary Multiple Exostoses (HME). 4. Red Flags: Discuss indications for MRI (cartilage cap thickness, pain, growth in adulthood) to rule out secondary chondrosarcoma. 5. Management: Conservative for asymptomatic lesions. Surgical excision only for mechanical irritation, neurovascular compromise, or suspected malignant transformation.
