Wrist Arthroscopy: A Masterclass in Dorsal, Midcarpal, and Volar Portal Techniques
Key Takeaway
Join us in the OR for an immersive masterclass in wrist arthroscopy. We'll meticulously detail dorsal, midcarpal, and volar portal techniques, emphasizing comprehensive surgical anatomy, neurovascular risks, and real-time intraoperative execution. Learn to navigate complex wrist pathology, from ligamentous tears to chondral lesions, with precision and confidence, ensuring optimal outcomes and managing potential pitfalls.
Comprehensive Introduction and Patho-Epidemiology
Wrist arthroscopy has undergone a profound evolution over the past three decades, transforming from a nascent, purely diagnostic modality into an indispensable therapeutic cornerstone of modern hand and upper extremity surgery. Initially popularized by pioneers such as Terry Whipple in the 1980s, the procedure was originally reserved for visualizing intra-articular pathology that eluded traditional imaging or open arthrotomy. Today, it is a highly sophisticated discipline requiring a deep, three-dimensional understanding of carpal kinematics, precise micro-instrument handling, and an absolute mastery of regional neurovascular anatomy. This masterclass chapter is designed to transition the orthopedic surgeon from basic diagnostic proficiency to advanced therapeutic competence, detailing the nuances of dorsal, midcarpal, and volar portal techniques.
The epidemiology of wrist pathology necessitates a robust arthroscopic skill set. Chronic wrist pain remains one of the most challenging diagnostic dilemmas in orthopedic practice. A significant portion of these cases involves subtle soft-tissue derangements—such as intrinsic ligament tears (scapholunate and lunotriquetral) or triangular fibrocartilage complex (TFCC) lesions—that frequently escape detection on standard magnetic resonance imaging (MRI) or MR arthrography. Furthermore, the incidence of high-energy distal radius fractures and complex carpal trauma has driven the demand for minimally invasive, arthroscopically assisted reduction techniques. By offering direct, magnified visualization of the articular surface, arthroscopy allows for the precise restoration of joint congruency, thereby mitigating the long-term risk of post-traumatic osteoarthritis.

Mastering wrist arthroscopy involves navigating a notoriously steep learning curve. Unlike the knee or shoulder, the radiocarpal and midcarpal joints offer limited working space, demanding meticulous portal placement to avoid iatrogenic injury to the dense network of overlying tendons and sensory nerves. The surgeon must develop a profound tactile and spatial awareness, often triangulating instruments within a joint space barely a few millimeters wide. This requires not only a steady hand but also an intimate familiarity with the tactile feedback provided by various arthroscopic probes and shavers as they interact with healthy versus pathologic chondral and ligamentous tissue.

Recent technological advancements have significantly expanded the therapeutic horizons of wrist arthroscopy. The advent of smaller, high-definition arthroscopes (ranging from standard 2.7 mm down to 1.9 mm and even sub-millimeter nanoscopes), specialized radiofrequency ablation probes, and low-profile suture anchors has enabled surgeons to perform complex reconstructions entirely through the arthroscope. From the management of scapholunate advanced collapse (SLAC) and scaphoid nonunion advanced collapse (SNAC) to the complete arthroscopic resection of volar ganglion cysts, the modern orthopedic surgeon must be adept at utilizing these advanced tools within the confined architecture of the wrist.
Detailed Surgical Anatomy and Biomechanics
A rigorous comprehension of wrist anatomy is the absolute prerequisite for safe and effective arthroscopy. The wrist is not a single joint but a complex articulation comprising the radiocarpal, midcarpal, and distal radioulnar joints (DRUJ). The radiocarpal joint is formed by the articulation of the distal radius and the TFCC with the proximal carpal row (scaphoid, lunate, and triquetrum). The inherent stability of this joint relies heavily on the intricate network of extrinsic volar and dorsal radiocarpal ligaments, as well as the intrinsic interosseous ligaments. Understanding the precise origins and insertions of these ligaments is crucial, as they serve as vital intra-articular landmarks during the arthroscopic examination.
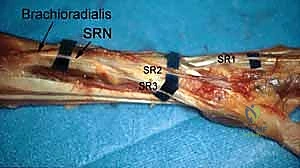
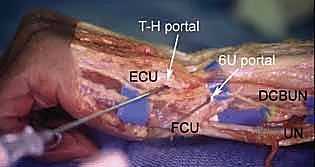
The dorsal topography of the wrist is defined by the six extensor compartments, which serve as the primary navigational beacons for dorsal portal placement. Lister's tubercle, a prominent bony ridge on the dorsal distal radius, separates the second compartment (extensor carpi radialis longus and brevis) from the third compartment (extensor pollicis longus). The intervals between these compartments provide relatively safe corridors for joint access. However, the surgeon must remain acutely aware of the superficial venous network and the cutaneous sensory nerves that traverse this region. The superficial branch of the radial nerve (SBRN) and the dorsal cutaneous branch of the ulnar nerve (DCBUN) are highly variable in their branching patterns and are exquisitely vulnerable to iatrogenic injury during portal creation.
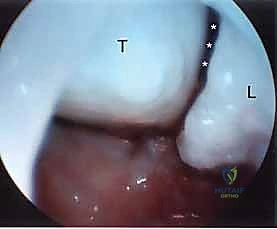
The biomechanics of the wrist further dictate the arthroscopic approach. The proximal carpal row acts as an intercalated segment, moving passively in response to forces transmitted from the distal carpal row and the forearm. This dynamic relationship is best appreciated during midcarpal arthroscopy, where the integrity of the scapholunate (SL) and lunotriquetral (LT) intervals can be dynamically assessed under direct visualization. The "dart-thrower's motion"—a coupled movement of radial deviation/extension to ulnar deviation/flexion—primarily occurs at the midcarpal joint. Recognizing normal versus abnormal kinematics during arthroscopic probing is essential for diagnosing dynamic carpal instability.
Volar wrist anatomy presents a significantly higher degree of complexity and risk, making volar portals the domain of the advanced arthroscopist. The volar aspect is densely packed with critical neurovascular structures, including the median nerve, the ulnar neurovascular bundle, and the radial artery, alongside the robust flexor tendon apparatus. Accessing the radiocarpal joint from the volar side requires precise navigation through specific internervous and intertendinous planes. The volar capsule itself is thick and reinforced by the stout volar extrinsic ligaments (e.g., radioscaphocapitate, long radiolunate), which must be carefully bypassed to enter the joint space without causing destabilizing iatrogenic trauma.
Exhaustive Indications and Contraindications
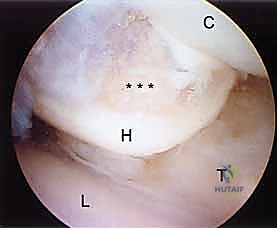
The indications for wrist arthroscopy have broadened significantly, encompassing both diagnostic and complex therapeutic interventions. Diagnostically, it remains the gold standard for evaluating chronic, unexplained wrist pain that has proven refractory to conservative measures such as immobilization, nonsteroidal anti-inflammatory drugs (NSAIDs), and targeted corticosteroid injections. When advanced imaging modalities yield equivocal results, arthroscopy provides unparalleled, magnified visualization of the articular cartilage, intrinsic ligaments, and the TFCC. It allows for the dynamic assessment of ligamentous competence, facilitating the identification of subtle, dynamic instabilities (Geissler grade I and II tears) that are entirely undetectable on static imaging.

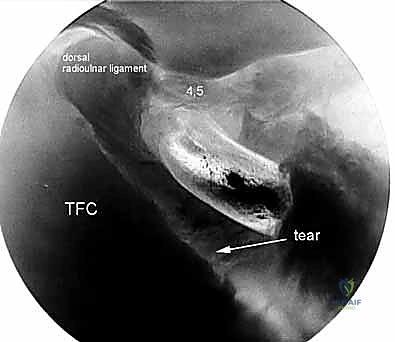
Therapeutically, wrist arthroscopy is now routinely employed for a vast array of pathologies. It is highly effective for the debridement or repair of TFCC tears (Palmer classifications), synovectomy in inflammatory arthritides, and the resection of both dorsal and volar carpal ganglion cysts. Furthermore, it serves as an invaluable adjuvant procedure in the management of intra-articular distal radius and scaphoid fractures. By allowing direct visualization of the articular surface, the surgeon can ensure anatomic reduction, meticulously clear fracture hematoma and debris, and concurrently address associated soft-tissue injuries, which are present in a significant percentage of these fractures.
Despite its utility, wrist arthroscopy carries specific contraindications that must be rigorously respected to prevent catastrophic complications. Absolute contraindications include active local or systemic infection, which poses a severe risk of introducing pathogens deep into the joint space, potentially leading to septic arthritis. Additionally, profound, uncorrectable coagulopathies present an unacceptable risk of uncontrollable intra-articular hemarthrosis, which not only obscures visualization but can also lead to long-term joint stiffness and cartilage degradation.
Relative contraindications require careful clinical judgment. Marked distortion of the regional anatomy—whether due to severe acute trauma, massive swelling, or prior extensive surgical procedures—can obscure the standard topographical landmarks, making safe portal placement exceedingly difficult and drastically increasing the risk of neurovascular injury. Similarly, the presence of massive capsular tears is a critical relative contraindication; the infusion of pressurized irrigation fluid can lead to rapid, massive extravasation into the forearm compartments, precipitating acute compartment syndrome.
| Category | Specific Condition | Rationale / Clinical Context |
|---|---|---|
| Diagnostic Indications | Unexplained Chronic Wrist Pain | Direct visualization of occult chondral, ligamentous, or capsular pathology missed by MRI/CT. |
| Suspected Carpal Instability | Dynamic probing allows Geissler staging of SL and LT interosseous ligament tears. | |
| Therapeutic Indications | TFCC Tears (Palmer Types 1 & 2) | Allows precise debridement of central tears or anatomic suture repair of peripheral avulsions. |
| Intra-articular Fractures | Ensures step-off free reduction of distal radius/scaphoid fractures; addresses concomitant soft-tissue injury. | |
| Ganglion Cyst Resection | Minimally invasive stalk resection for both dorsal and volar ganglia, reducing postoperative stiffness. | |
| Absolute Contraindications | Active Local/Systemic Infection | High risk of iatrogenic septic arthritis and systemic dissemination. |
| Severe Uncorrected Coagulopathy | Risk of massive hemarthrosis, obscured visualization, and postoperative stiffness. | |
| Relative Contraindications | Severe Anatomic Distortion | Loss of palpable landmarks increases the risk of iatrogenic injury to SBRN, DCBUN, and tendons. |
| Massive Capsular Disruption | High risk of fluid extravasation leading to acute forearm compartment syndrome. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the foundation of a successful wrist arthroscopy. The surgeon must comprehensively review all available imaging modalities, including high-resolution plain radiographs, computed tomography (CT) scans for osseous architecture, and MRI or MR arthrography for soft-tissue assessment. Mental templating is crucial; the surgeon must pre-determine the primary viewing and working portals based on the specific targeted pathology. For instance, addressing a radial-sided TFCC avulsion will require a different portal strategy and instrument trajectory than repairing a dorsal capsular avulsion of the scapholunate ligament.

The surgical setup demands precise coordination with the operating room staff. The choice of anesthesia—typically a regional block (supraclavicular or axillary) combined with intravenous sedation, or general anesthesia—depends on the anticipated length of the procedure and patient specific factors. A pneumatic tourniquet is routinely applied to the proximal arm to ensure a bloodless field, which is absolutely critical for maintaining clear visualization within the small confines of the wrist joint. The limb is exsanguinated using an Esmarch bandage prior to tourniquet inflation, typically set to 250 mm Hg.
Patient positioning is standardized but requires exacting attention to detail. The patient is positioned supine, with the operative arm extended onto a radiolucent hand table. A specialized traction tower is clamped securely to the table. Sterile finger traps are applied—typically to the index and middle fingers for central/radial pathology, or the middle and ring fingers to bias ulnar distraction. The arm is suspended, and the elbow is flexed to 90 degrees. Counter-traction is applied via a padded strap over the distal humerus. Approximately 10 to 15 pounds of longitudinal traction is applied; this weight must be sufficient to distract the radiocarpal and midcarpal joints by 2 to 3 millimeters, facilitating safe trocar entry, without causing neuropraxia to the brachial plexus or peripheral nerves.

Equipment selection must be finalized prior to the incision. The standard workhorse is the 2.7 mm, 30-degree angled arthroscope, though a 1.9 mm scope is frequently required for tight midcarpal joints or smaller patients. The surgeon must ensure the availability of a comprehensive array of specialized hand arthroscopy instruments: blunt and sharp trocars, a calibrated probe, various biters and graspers, and motorized shaver systems (typically 2.0 mm to 2.9 mm). If therapeutic intervention is planned, the specific devices—such as RF ablation wands, suture passing devices, or micro-anchors—must be readily available on the sterile field. Fluoroscopy must be positioned to allow easy C-arm access without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
The creation of arthroscopic portals must adhere to strict surgical principles to mitigate the risk of iatrogenic injury. The universal rule for wrist arthroscopy is the "nick and spread" technique. After identifying the anatomical landmarks and marking the portal sites, a superficial incision is made strictly through the epidermis using a #15 blade. A fine, curved hemostat is then introduced and used to bluntly dissect the subcutaneous tissues down to the joint capsule. This blunt spreading pushes the superficial sensory nerves (SBRN and DCBUN) and traversing veins out of the trajectory of the trocar, drastically reducing the incidence of painful postoperative neuromas.

Dorsal Radiocarpal Portals
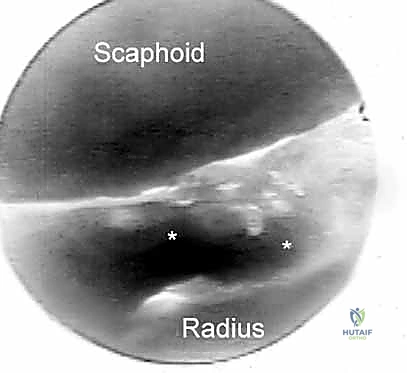
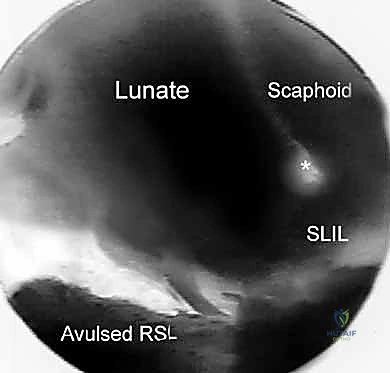
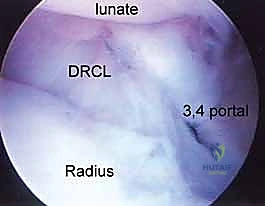
The dorsal radiocarpal portals are the foundational access points for wrist arthroscopy. The 3-4 portal is the standard initial viewing portal. Located approximately 1 cm distal to Lister's tubercle, between the extensor pollicis longus (EPL, 3rd compartment) and the extensor digitorum communis (EDC, 4th compartment), it provides a commanding view of the radioscaphoid and radiolunate articulations. The trocar must be directed with a 10 to 15-degree volar tilt to match the natural volar inclination of the distal radius articular surface.
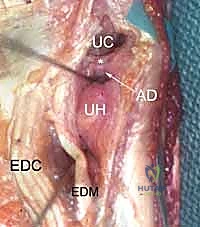
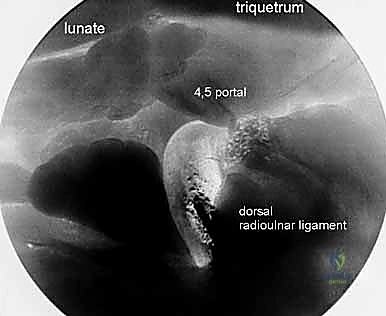
The 4-5 portal serves as the primary working portal for radial-sided pathology and the primary viewing portal for the ulnocarpal joint. It is situated between the EDC (4th compartment) and the extensor digiti minimi (EDM, 5th compartment). When establishing this portal, the surgeon must be cognizant of the DCBUN branches, which become increasingly prevalent as one moves ulnarly. Triangulation between the 3-4 and 4-5 portals allows for comprehensive assessment and instrumentation of the majority of radiocarpal pathology.
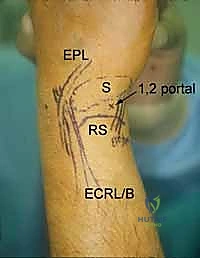
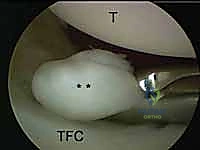
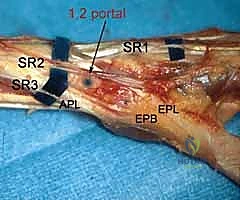
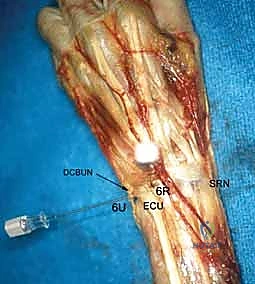
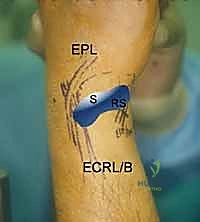
Further ulnar access is achieved via the 6R (radial to ECU) and 6U (ulnar to ECU) portals. The 6R portal is an excellent working portal for TFCC debridement and repair, offering a direct trajectory to the ulnar insertion of the complex. The 6U portal is frequently utilized as an outflow tract or for specific ulnar-sided repairs, but it carries a higher risk to the main trunk of the DCBUN. Conversely, the 1-2 portal, located between the first (APL/EPB) and second (ECRL/ECRB) compartments, is utilized for radial styloidectomy and viewing the extreme radial aspect of the joint. The SBRN branches are highly concentrated here, demanding extreme caution and meticulous blunt dissection.
Midcarpal Portals
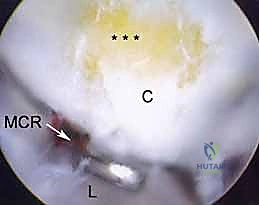
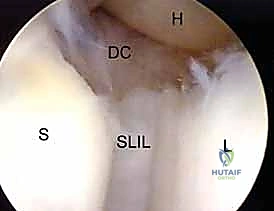
Midcarpal arthroscopy is essential for evaluating dynamic carpal instability and staging degenerative diseases like SLAC and SNAC. The Radial Midcarpal (MCR) portal is located approximately 1 cm distal to the 3-4 portal, in the soft spot between the capitate, scaphoid, and lunate. This portal provides an exceptional view of the scapholunate interval from its distal aspect, allowing the surgeon to probe the articulation and assess for Geissler grade instability.
The Ulnar Midcarpal (MCU) portal, situated 1 cm distal to the 4-5 portal, aligns with the capitohamate, lunate, and triquetrum articulation. It is the primary portal for evaluating the lunotriquetral (LT) interosseous ligament. The STT (Scaphotrapeziotrapezoid) portal, located just distal to the scaphoid tubercle and radial to the FCR tendon, is specialized for evaluating STT arthritis and assisting in localized procedures, though it requires careful avoidance of the radial artery branches.

Volar Portals
Volar portals represent an advanced frontier in wrist arthroscopy, utilized primarily when dorsal access is insufficient or for specific pathologies like volar ganglion cysts or volar capsular repairs. These portals carry a significantly higher risk profile. The Volar Radial (VR) portal is established through the bed of the flexor carpi radialis (FCR) sheath. The surgeon must meticulously retract the FCR tendon ulnarly and the radial artery radially to safely access the joint capsule, avoiding the palmar cutaneous branch of the median nerve.
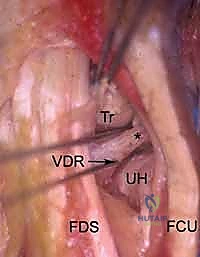
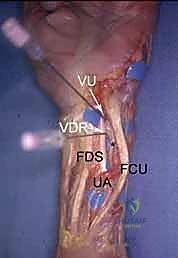
The Volar Ulnar (VU) portal is placed between the flexor digitorum superficialis (FDS) tendons and the flexor carpi ulnaris (FCU). The critical structures at risk here are the main trunk of the ulnar nerve and artery, which lie immediately ulnar to the portal trajectory. Creation of volar portals often involves an "inside-out" technique, where a switching stick is passed from a dorsal portal out through the volar capsule to precisely identify the safe zone before making the volar skin incision.

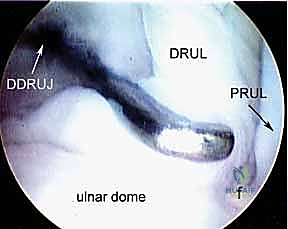
Distal Radioulnar Joint (DRUJ) Portals
Assessment of the DRUJ is critical in patients with ulnar-sided wrist pain, TFCC pathology, or DRUJ instability. The Proximal DRUJ portal is located just proximal to the ulnar head, between the EDM and ECU tendons. It allows visualization of the proximal aspect of the sigmoid notch and the ulnar head cartilage.

The Distal DRUJ portal is placed slightly more distally in the same EDM-ECU interval, providing access to the deep surface of the TFCC (the foveal insertion) and the distal articular surfaces. Navigating the DRUJ requires a smaller arthroscope (typically 1.9 mm) due to the highly constrained nature of the joint space. Care must be taken to avoid the transverse branches of the DCBUN during portal placement in this region.