Masterclass: Arthroscopic & Open Management of Pediatric Tibial Spine Fractures
Key Takeaway
This masterclass details the comprehensive management of pediatric tibial spine fractures, from advanced surgical anatomy and meticulous preoperative planning to granular intraoperative execution. We explore arthroscopic and open reduction techniques using screws, sutures, or K-wires, emphasizing physeal preservation. Fellows will gain insights into critical pearls, pitfalls, and postoperative protocols for optimal patient outcomes, ensuring stable anatomic fixation and successful rehabilitation.
Comprehensive Introduction and Patho-Epidemiology
Colleagues, welcome to this advanced masterclass on the management of pediatric tibial spine fractures. In the realm of pediatric orthopedic trauma and sports medicine, the tibial spine fracture represents a critical, high-stakes injury. Synonymous with an anterior cruciate ligament (ACL) avulsion fracture, this pathology is predominantly observed in the skeletally immature population. Unlike adults, who typically sustain midsubstance ACL ruptures under extreme valgus and rotational loads, children possess ligaments that are biomechanically stronger than their corresponding osteochondral attachments. Consequently, the tensile forces transmitted through the ACL during trauma often exceed the cohesive strength of the unossified or partially ossified tibial eminence, resulting in an avulsion fracture rather than a ligamentous tear.
Experimental biomechanical models have elucidated the precise mechanisms governing this injury pattern. Studies demonstrate that rapid loading rates tend to cause midsubstance ACL tears across all age groups, whereas a more gradual loading mechanism, combined with the relative weakness of the pediatric physeal and chondral structures, precipitates these tibial spine avulsions. Interestingly, advanced imaging studies comparing skeletally immature knees with tibial spine fractures to those with midsubstance ACL tears have identified morphological variations, such as a narrower intercondylar notch in patients who sustain midsubstance tears. This anatomical predisposition highlights the unique, multifactorial biomechanics at play in the developing knee joint.
Epidemiologically, this injury predominantly affects younger individuals—typically between the ages of 8 and 14 years—with an incidence of approximately 3 per 100,000 children annually. Historically, the classic mechanism of injury involved a fall from a bicycle. However, with the increasing participation of youth in high-velocity, competitive sports, we are witnessing a paradigm shift. Sports-related injuries, particularly from skiing, soccer, and football, now account for a significant and growing proportion of these fractures. The kinematic mechanism usually involves a forced valgus moment applied to the knee, coupled with external rotation forces, or a violent hyperextension injury with rotational moments.
To standardize our approach and guide treatment algorithms, we rely on the time-honored Meyers and McKeever classification system, along with the Zaricznyj modification. This system categorizes the injury based on the degree of displacement and comminution:
* Type I: A completely nondisplaced fracture where the osteochondral fragment rests anatomically in its bed.
* Type II: A partially displaced fracture. The anterior portion of the fragment is elevated (often described as a "beak"), while the posterior cortex remains intact, acting as a functional hinge.
* Type III: Complete displacement of the fragment. The avulsed bone is entirely separated from its bed and may be rotated or translated.
* Type IV (Zaricznyj modification): A comminuted fracture, indicating multiple osseous fragments or severe fragmentation of the avulsed bone, which significantly complicates fixation strategies.
FIG 1 • Meyers and McKeever classification. Type I has minimally displaced fragments. Type II has displacement through the anterior portion of the fracture with an intact posterior hinge. Type III has complete displacement of the fracture fragments.

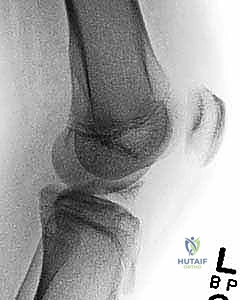
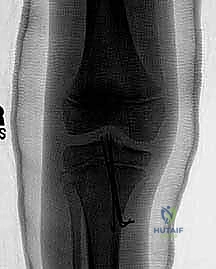
FIG 2 • AP and lateral radiographs of the knee demonstrating a completely displaced tibial spine fracture (Type III).
Clinical Presentation and Diagnostic Workup
Patients presenting with a tibial spine fracture typically report a painful, acutely swollen knee following a specific traumatic event. The rapid onset of swelling is invariably due to a tense hemarthrosis resulting from the intra-articular fracture bleeding. These patients will almost universally present with an antalgic gait or an absolute inability to bear weight on the affected extremity. The knee is often held in a position of slight flexion (typically 15 to 20 degrees) to maximize intra-articular volume and minimize capsular tension, thereby reducing pain.
A meticulous physical examination is the cornerstone of initial evaluation, though it must be performed gently to accommodate patient apprehension and pain. Inspection will reveal the effusion, and palpation will elicit exquisite tenderness localized over the anterior joint line and tibial eminence. Range of motion is predictably restricted and painful, particularly in terminal extension, which stretches the ACL and pulls on the fracture fragment. Ligamentous stability testing is paramount; the Lachman test is the most sensitive clinical maneuver. A positive Lachman test—characterized by increased anterior tibial translation with a soft or absent endpoint—indicates functional disruption of the ACL complex. The anterior drawer test may also be positive, though it is often limited by the hemarthrosis and protective hamstring spasm.
Radiographic evaluation begins with standard orthogonal views: Anteroposterior (AP) and lateral radiographs of the knee. These are usually sufficient to diagnose the fracture, classify the injury according to Meyers and McKeever, and define the extent of the bony avulsion. However, in very young children where the tibial spine is predominantly cartilaginous, radiographs might only reveal a subtle, millimeter-sized fleck of avulsed bone. In modern practice, Magnetic Resonance Imaging (MRI) has become the gold standard adjunct. MRI not only confirms the diagnosis and delineates the exact size of the chondral fragment but is absolutely critical for identifying concomitant intra-articular pathology. Meniscal tears, entrapment of the anterior horn of the medial meniscus or the transverse intermeniscal ligament beneath the fracture fragment, and occult osteochondral lesions are frequently identified on MRI and will fundamentally alter the surgical plan.
Detailed Surgical Anatomy and Biomechanics
Before advancing to surgical intervention, a profound, three-dimensional understanding of the knee's surgical anatomy is non-negotiable. The intercondylar area of the tibia is a complex geographic landscape. The tibial eminence serves as our primary focal point, located centrally between the medial and lateral articular surfaces. It is characterized by two distinct triangular elevations: the medial and lateral intercondylar tubercles. The medial elevation is of paramount clinical importance, as its anterior slope provides the primary anatomical footprint for the fibers of the anterior cruciate ligament. The lateral tubercle, conversely, typically lacks direct ligamentous attachments but serves as a crucial anatomical landmark during arthroscopy.
The ligamentous and meniscal anatomy surrounding the tibial spine is dense and highly interrelated. The anterior horn of the medial meniscus inserts directly anterior to the ACL footprint, while the anterior horn of the lateral meniscus inserts slightly posterior and lateral to the ACL, often blending with the ACL fibers. The transverse intermeniscal ligament connects these two anterior horns, draping directly across the anterior aspect of the tibial eminence. When a tibial spine fracture displaces (Type II or III), the anterior horn of the medial meniscus or the intermeniscal ligament frequently prolapses into the fracture crater. This soft tissue interposition acts as a mechanical block to anatomical reduction, a phenomenon that mandates meticulous arthroscopic clearing before any fixation is attempted.
FIG 3 • Axial view of the tibial plateau. A. The intercondylar eminence lies between the medial and lateral condyles. B. The medial portion serves as the attachment of the anterior cruciate ligament.
Neurovascular and Physeal Considerations
Navigating the pediatric knee requires acute awareness of surrounding neurovascular structures to prevent iatrogenic injury. The infrapatellar branch of the saphenous nerve is particularly vulnerable. This sensory nerve courses transversely across the proximal anteromedial tibia and frequently crosses the surgical field during the establishment of the anteromedial arthroscopic portal or a medial parapatellar mini-arthrotomy. Inadvertent transection or entrapment in a suture knot can lead to a debilitating, painful neuroma or persistent numbness over the anteromedial aspect of the knee. Careful superficial dissection and spreading with a hemostat during portal placement can mitigate this risk.
Deeper structures, while less commonly injured during anterior approaches, must remain in the surgeon's cognitive map. The popliteal artery and its genicular branches lie directly posterior to the posterior capsule. Over-penetration of guide pins, drills, or K-wires during trans-tibial tunnel creation or screw fixation can result in catastrophic vascular compromise. Similarly, the common peroneal nerve is at risk during extreme varus or internal rotation maneuvers, though less directly threatened by the standard anterior portals used for tibial spine fixation.
Perhaps the most critical anatomical consideration unique to this patient population is the presence of the proximal tibial physis and the tibial tubercle apophysis. The proximal tibial growth plate is responsible for a significant portion of longitudinal leg growth. Any fixation device—be it a screw, K-wire, or drill tunnel for sutures—that crosses this physis carries an inherent risk of iatrogenic premature physeal closure. This can result in devastating complications, including angular deformities (such as genu recurvatum if the anterior physis arrests) or significant limb length discrepancies. Consequently, our surgical techniques must be meticulously designed to be physeal-sparing, utilizing epiphyseal drillings or avoiding hardware across the growth plate whenever anatomically feasible.
Exhaustive Indications and Contraindications
The decision-making process for managing pediatric tibial spine fractures hinges on achieving a stable, anatomical reduction that restores the tension of the ACL while respecting the biological constraints of the growing skeleton. The treatment algorithm is primarily dictated by the Meyers and McKeever classification, the reducibility of the fracture, and the presence of concomitant intra-articular injuries.
| Treatment Modality | Primary Indications | Relative/Absolute Contraindications |
|---|---|---|
| Non-Operative (Casting) | - Meyers & McKeever Type I (Nondisplaced) - Meyers & McKeever Type II (Reducible with closed maneuvers) - Absence of meniscal entrapment |
- Meyers & McKeever Type III or IV - Irreducible Type II fractures - Concomitant meniscal tears requiring repair - Polytrauma preventing cast care |
| Arthroscopic Fixation | - Meyers & McKeever Type III (Completely displaced) - Irreducible Type II fractures - Meyers & McKeever Type IV (Comminuted) - Soft tissue entrapment (meniscus/ligament) |
- Severe capsular disruption with massive fluid extravasation risk - Extremely small, purely cartilaginous fragments (relative - requires advanced suturing) |
| Open Fixation (Mini-Arthrotomy) | - Failure of arthroscopic reduction - Severe comminution requiring direct visualization and bone grafting - Surgeon preference/lack of arthroscopic expertise |
- Uncomplicated Type I or II fractures - High risk of arthrofibrosis (relative) |
Non-Operative Management Protocols
Non-operative management remains the gold standard for genuinely nondisplaced Type I fractures and select Type II fractures that demonstrate concentric, stable reduction following closed manipulation. The technique for closed reduction of a Type II fracture must be performed with precision. Initially, under sterile conditions, the tense hemarthrosis is aspirated. This not only provides immediate analgesic relief but also decompresses the joint, removing the hydraulic block to reduction. Following aspiration, a local anesthetic (such as intra-articular bupivacaine) is injected to facilitate patient relaxation.
The reduction maneuver relies on the cam effect of the femoral condyles. The knee is brought into full, passive extension. As the knee extends, the intercondylar notch and the lateral femoral condyle apply direct downward pressure onto the elevated, anteriorly displaced "beak" of the tibial spine fragment, pressing it back into its anatomical bed. It is critical to note that this maneuver is highly effective for large, ossified fragments but may fail in purely cartilaginous lesions where the soft tissue hinges prevent seating.
Following the reduction maneuver, immediate AP and lateral radiographs are obtained to confirm anatomical restoration. If reduction is acceptable, the limb is immobilized in a long-leg cast. The optimal position of immobilization has been a subject of historical debate. While older literature advocated for full extension to maintain the reduction via the femoral condyle, this position maximizes tension on the ACL, potentially leading to gradual displacement or plastic deformation of the ligament. Current consensus strongly recommends casting the knee in 10 to 20 degrees of flexion. This slight flexion relaxes the ACL fibers, reducing the distracting tensile forces on the fracture fragment, while still maintaining sufficient condylar pressure to prevent displacement. Close radiographic follow-up at 1 and 2 weeks post-injury is mandatory; any loss of reduction necessitates prompt conversion to surgical fixation.
Pre-Operative Planning, Templating, and Patient Positioning
Surgical success in pediatric tibial spine fractures is predicated on exhaustive preoperative planning. The surgeon must transition from a general understanding of the injury to a highly specific, patient-tailored surgical blueprint. This begins with a rigorous review of all available imaging. Plain radiographs provide the baseline architecture, but the MRI is the definitive roadmap. The surgeon must scrutinize the MRI to determine the exact dimensions of the osseous fragment versus the cartilaginous envelope. A large, robust bony fragment may be highly amenable to cannulated screw fixation. Conversely, a fragment that is predominantly cartilaginous or highly comminuted (Type IV) will almost certainly require a suture-based cerclage or transosseous equivalent technique.
Mentally templating the trajectory of fixation is crucial. If screw fixation is planned, the surgeon must calculate the required angle of approach to ensure the screw achieves perpendicular compression across the fracture site without violating the posterior tibial cortex or the proximal tibial physis. If suture fixation is anticipated, the surgeon must plan the placement of the trans-tibial or epiphyseal drill tunnels, ensuring an adequate bone bridge between the tunnels to prevent cutout when the sutures are tensioned.
Examination Under Anesthesia and Operating Room Setup
Once the patient is in the operating theater, an Examination Under Anesthesia (EUA) is the first formal surgical step. With the patient completely relaxed and free of muscle guarding, the surgeon must assess the true degree of anteroposterior laxity (Lachman and Drawer tests) and varus/valgus stability. This establishes a baseline for comparison once fixation is achieved. Furthermore, assessing the passive range of motion, particularly terminal extension, helps identify mechanical blocks that will need to be addressed arthroscopically.
Patient positioning is optimized for standard knee arthroscopy. The patient is placed supine on the operating table. A well-padded high-thigh tourniquet is applied to the operative leg to ensure a bloodless field, which is critical for visualizing the intricate anatomy of the intercondylar notch. The operative leg can be placed in a standard leg holder, allowing for dynamic manipulation of the knee between 0 and 120 degrees of flexion. Alternatively, a lateral post can be utilized, allowing the leg to rest in a dependent position over the edge of the table. The contralateral leg is placed in a well-padded gynecological stirrup or supported on a flat board, ensuring all bony prominences are protected to prevent neuropathies. The arthroscopy tower is positioned across from the surgeon, and a standard 30-degree arthroscope is utilized. A 70-degree scope should be available on the back table, as it can occasionally be useful for visualizing the posterior aspect of the fracture bed or confirming the reduction of the posterior hinge.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of tibial spine fractures has evolved significantly, with arthroscopic techniques now representing the standard of care due to reduced morbidity, improved visualization of intra-articular structures, and the ability to concurrently address meniscal pathology.
Arthroscopic Evaluation and Preparation of the Bed
The procedure commences with the establishment of standard anterolateral and anteromedial portals. The anterolateral portal is created first, serving as the primary viewing portal. Upon entering the joint, the surgeon is typically met with a dense hemarthrosis. A thorough joint lavage is performed using an arthroscopic shaver to clear the hematoma and establish clear visualization.
The initial diagnostic sweep must be systematic. The surgeon evaluates the patellofemoral compartment, the medial and lateral gutters, and both menisci. Attention is then directed to the intercondylar notch. The displaced tibial spine fragment is identified, often attached to a lax and hemorrhagic ACL. The critical next step is identifying the barrier to reduction. Using an arthroscopic probe, the surgeon meticulously inspects the fracture crater. In a vast majority of Type II and III fractures, the anterior horn of the medial meniscus, or the transverse intermeniscal ligament, is found prolapsed into the defect.


FIG 4 • Arthroscopic visualization of the fracture bed. Careful debridement of hematoma and interposed soft tissue is mandatory.
Using a combination of the shaver, an arthroscopic elevator, and biting forceps, the fracture bed is meticulously cleared of all interposed soft tissue, organized hematoma, and small, non-viable osseous debris. The base of the ACL and the undersurface of the avulsed fragment are also gently debrided to expose bleeding cancellous bone, which is essential for biological healing. Once the bed is prepared, a trial reduction is performed. An arthroscopic probe or a specialized reduction tool is used to push the fragment down and posterior into its anatomical footprint. The knee is cycled through a range of motion to assess the stability of the reduction.


FIG 5 • Instruments are used to clear the crater and trial the reduction of the tibial spine fragment.
Suture Fixation Technique
Suture fixation is highly versatile and is the preferred method for comminuted fractures, purely cartilaginous fragments, and very young patients where screw fixation poses an unacceptable risk to the physis.
The technique begins with passing high-strength, non-absorbable sutures (e.g., #2 or #5 UltraBraid or FiberWire) through the base of the ACL, immediately proximal to the osteochondral fragment. This can be achieved using various arthroscopic suture-passing devices, such as a suture lasso, a penetrating bird-beak device, or a specialized ACL drill guide. Typically, two to three sutures are passed in a luggage-tag or simple configuration, capturing the robust ligamentous tissue.

FIG 6 • Passing high-strength non-absorbable sutures through the base of the ACL just above the bony avulsion.
Next, trans-tibial tunnels must be created to shuttle the sutures out of the joint. An ACL tibial drill guide is introduced through the anteromedial portal and positioned at the medial and lateral margins of the fracture bed. Through a small, 2-cm incision over the anteromedial proximal tibia, guide pins are drilled into the joint. Crucially, in skeletally immature patients, the surgeon must use fluoroscopy to ensure these drill tunnels remain entirely within the epiphysis, avoiding the proximal tibial physis. If epiphyseal drilling is not possible due to patient size, smooth K-wires may be used to create small transphyseal tunnels, as smooth, small-diameter tunnels pose a lower risk of physeal arrest than larger, threaded devices.


FIG 7 • Creation of trans-tibial tunnels using a targeting guide, ensuring placement avoids the physis where possible.
The free ends of the sutures are then retrieved through the joint and shuttled down the respective medial and lateral trans-tibial tunnels.

FIG 8 • Shuttling the sutures down the trans-tibial tunnels.
With the knee held in 15 to 20 degrees of flexion, the sutures are tensioned simultaneously. This action pulls the ACL distally, compressing the osteochondral fragment firmly into its anatomical bed. The reduction is confirmed arthroscopically. Finally, the sutures are tied securely over the robust bone bridge on the anteromedial tibial cortex.
Screw Fixation Technique
For older adolescents or patients with a large, solitary, and robust osseous fragment, screw fixation provides excellent biomechanical compression and rigid stability.
Following bed preparation and trial reduction, the fragment is held in an anatomically reduced position using a K-wire or an arthroscopic probe. An ACL tibial guide or a freehand technique is used to advance a guidewire from the anteromedial portal, through the center of the avulsed fragment, and into the intact proximal tibia.
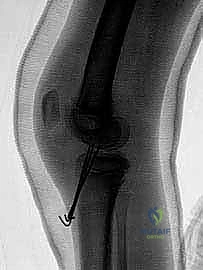
FIG 9 • Guidewire placement through the reduced fragment. Fluoroscopy is used to confirm trajectory.
Fluoroscopy is mandatory at this stage to confirm that the guidewire trajectory is appropriate, that it captures the fragment centrally, and most importantly, that it does not cross the proximal tibial physis. Once the guidewire is perfectly positioned, a cannulated, partially threaded screw (typically 3.5mm or 4.0mm) is advanced over the wire. Headless compression screws are particularly advantageous in this application, as they can be buried beneath the articular cartilage, eliminating the risk of hardware impingement in the intercondylar notch during terminal extension.

FIG 10 • Final fixation with a cannulated screw, achieving excellent compression of the fragment into its bed.
Regardless of the fixation method chosen, the final steps involve a meticulous arthroscopic inspection. The surgeon must confirm that the fragment is flush with the surrounding cartilage, that the ACL tension is restored (evidenced by a taut ligament when probed), and that there is no impingement of the hardware or the ACL against the roof of the intercondylar notch when the knee is brought into full extension.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the management of pediatric tibial spine fractures is fraught with potential complications. The surgeon must be profoundly aware of these risks, counsel the family appropriately preoperatively, and possess the surgical acumen to manage them should they arise.
| Complication | Estimated Incidence | Etiology / Pathophysiology | Management / Salvage Strategy |
|---|---|---|---|
| Arthrofibrosis | 10% - 15% | Most common complication. Caused by prolonged immobilization, excessive surgical trauma, or failure to initiate early ROM. | Aggressive physical therapy. If refractory beyond 3-4 months, requires Arthroscopic Lysis of Adhesions (LOA) and Manipulation Under Anesthesia (MUA). |
| Residual ACL Laxity | 20% - 40% | Plastic deformation (stretching) of the ACL substance prior to the avulsion event. Often asymptomatic. | Conservative management if asymptomatic. If patient experiences symptomatic instability (giving way), requires formal ACL reconstruction. |
| Malunion / Notch Impingement | 5% - 10% | Failure to achieve anatomical reduction, or use of prominent hardware (screw heads) blocking terminal extension. | Arthroscopic debridement, notchplasty, or hardware removal. |
| Physeal Growth Arrest | < 2% | Iatrogenic injury to the proximal tibial physis via drill tunnels, screws, or excessive heat necrosis. | Close radiographic monitoring. May require epiphysiodesis of the contralateral limb, or corrective osteotomy for angular deformity (e.g., recurvatum). |
| Nonunion | < |
