Essential Guide: Mastering Every Approach to the Shoulder
Key Takeaway
This article provides essential research regarding Essential Guide: Mastering Every Approach to the Shoulder. An approach to the shoulder describes surgical methods used to access the joint for treating conditions like instability, rotator cuff lesions, or fractures of the proximal humerus. Common approaches include anterior (often a "work-horse" incision), posterior, lateral, anterolateral, and arthroscopic techniques, each tailored for specific anatomical exposure and pathology.
Comprehensive Introduction and Patho-Epidemiology
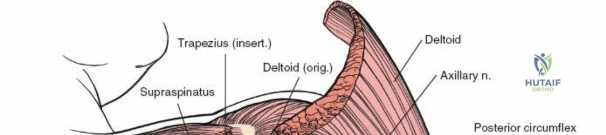
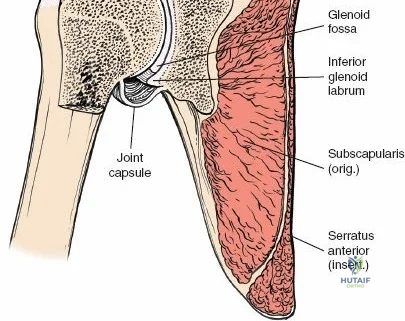
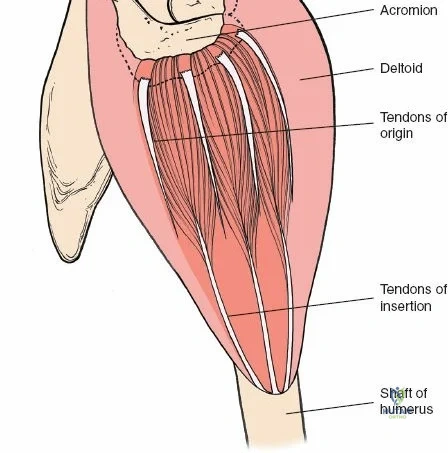
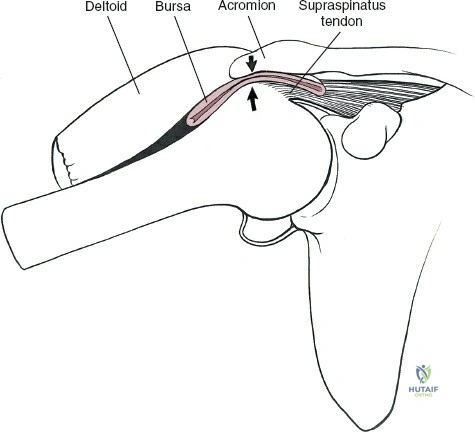
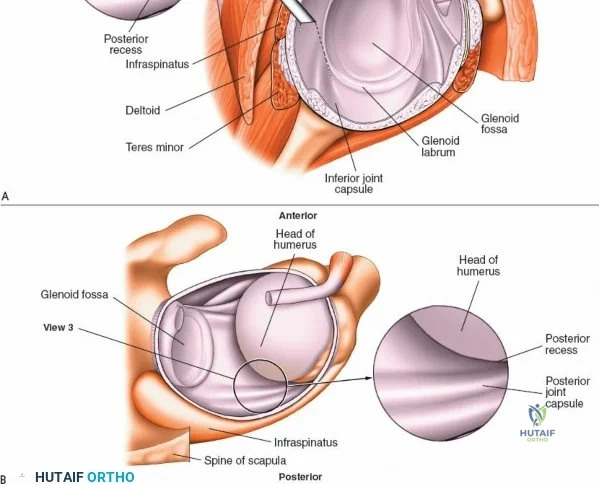
The shoulder represents the most mobile and biomechanically complex joint in the human body, characterized by a profound evolutionary trade-off between extensive global range of motion and intrinsic osseous stability. The glenohumeral joint is essentially a shallow ball-and-socket articulation where the humeral head surface area is roughly three to four times that of the glenoid fossa. Consequently, the joint relies almost entirely on its dynamic and static soft-tissue envelopes for constraint. It is surrounded by two distinct muscular sleeves: the outer sleeve, dominated by the deltoid muscle, which serves as the primary prime mover for elevation and abduction; and the inner sleeve, comprising the rotator cuff musculature, which is absolutely critical for the concavity compression and dynamic stability of the joint.
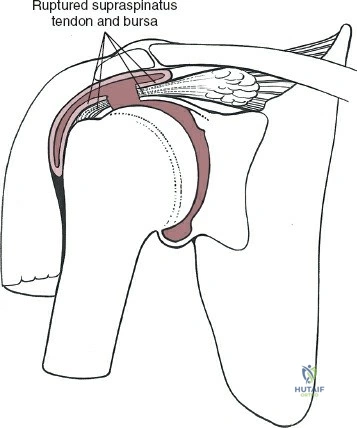
The epidemiology of shoulder pathology dictates the necessity for a versatile armamentarium of surgical approaches. The three most ubiquitous shoulder pathologies necessitating open or arthroscopic surgical intervention include glenohumeral instability (such as recurrent anterior dislocation resulting in Bankart lesions or significant glenoid bone loss), degenerative or traumatic lesions of the rotator cuff, and complex fractures of the proximal humerus and clavicle. As the aging population expands and high-energy trauma remains prevalent, orthopedic surgeons are increasingly tasked with addressing complex, multifactorial shoulder derangements that require precise, anatomically sound surgical exposures.
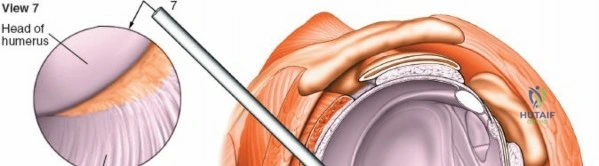
Historically, open surgical approaches were the exclusive modality for addressing these pathologies. However, the paradigm has shifted dramatically over the past three decades with the advent and refinement of arthroscopic techniques. Despite this minimally invasive revolution, mastery of open approaches remains a non-negotiable requirement for the comprehensive orthopedic surgeon. Nine primary surgical approaches form the foundation of shoulder surgery: the anterior (deltopectoral) and posterior approaches to the shoulder, the anterolateral approach to the acromioclavicular joint and subacromial space, the anterior approach to the clavicle, the lateral and minimally invasive lateral approaches to the proximal humerus, the minimally invasive anterolateral approach for humeral nailing, and the standard arthroscopic anterior and posterior approaches.

Of these, the anterior deltopectoral approach remains the undisputed "workhorse" incision of the shoulder. It provides unparalleled, extensile exposure of the glenohumeral joint, its anterior capsulolabral coverings, and the proximal humerus, making it indispensable for trauma and arthroplasty. Conversely, the anterolateral approach, once the gold standard for rotator cuff repair, has seen a decline in utilization due to the efficacy of all-arthroscopic techniques, though it remains highly relevant for specific proximal humerus fracture patterns. The posterior approach, while utilized less frequently, is critical for addressing recurrent posterior instability, open reduction and internal fixation (ORIF) of posterior glenoid rim fractures, and complex intra-articular scapular neck fractures. Ultimately, the selection of the approach must be meticulously tailored to the specific pathoanatomy, the planned reconstruction, and the patient's physiologic demands.
Detailed Surgical Anatomy and Biomechanics
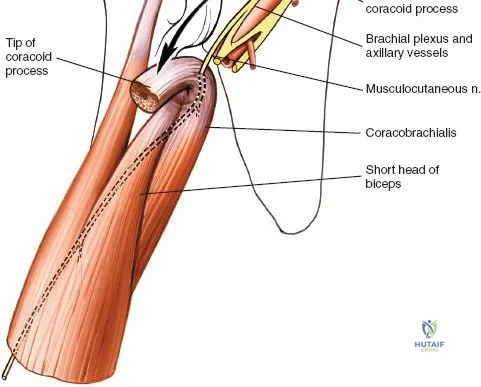
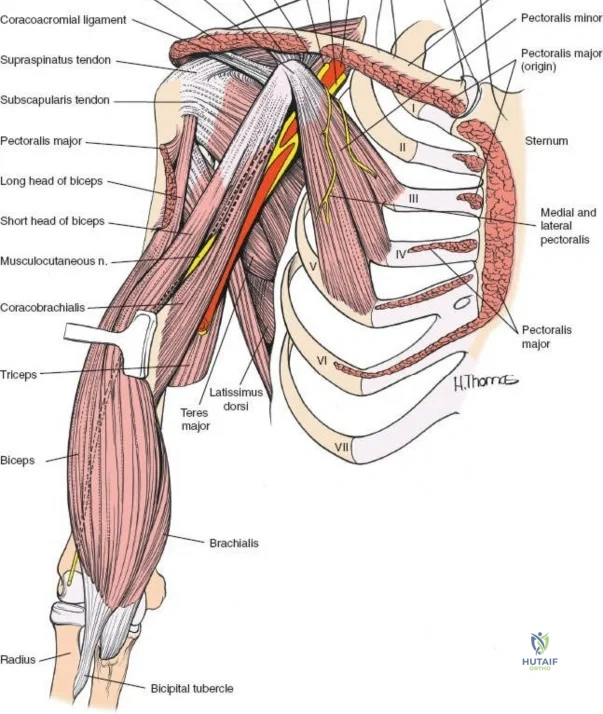
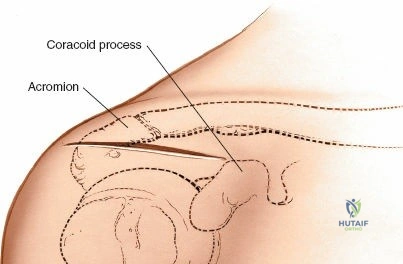
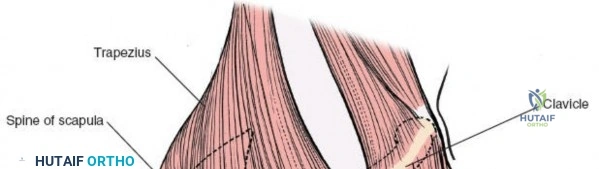
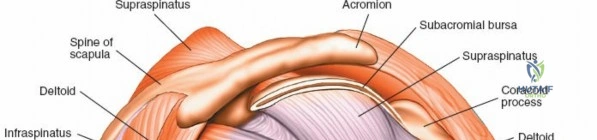
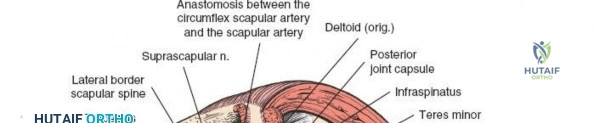
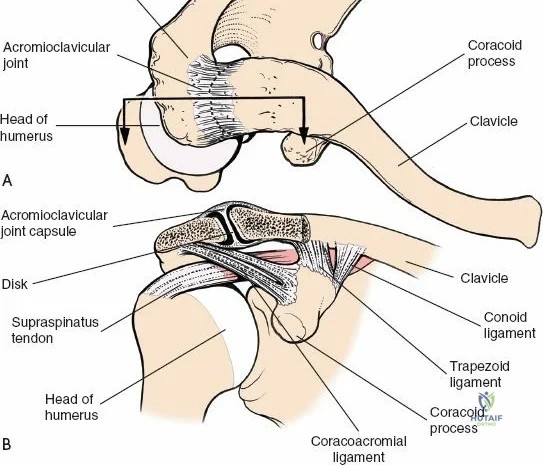
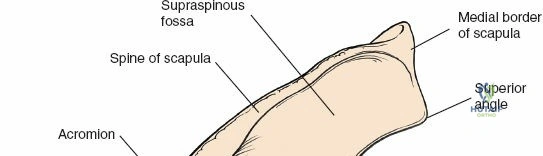
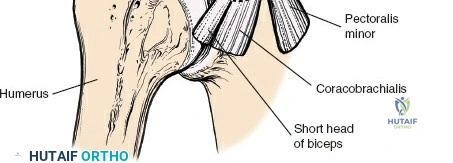
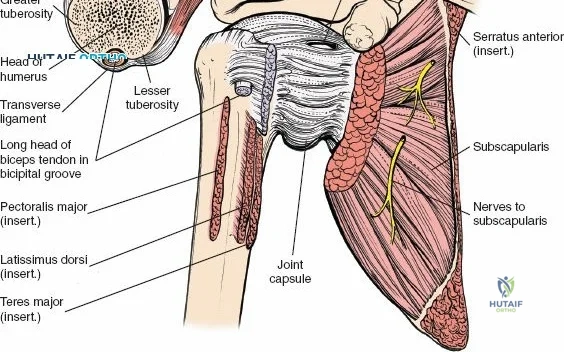
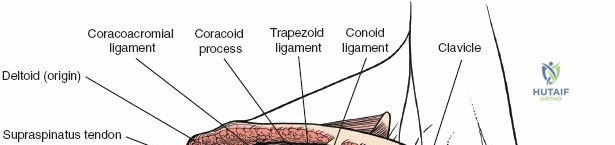
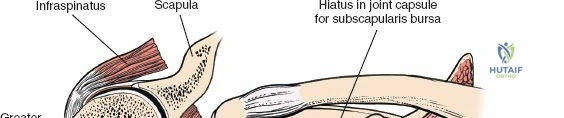
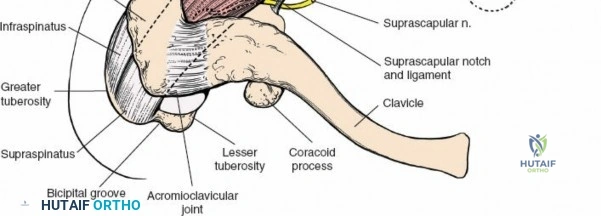
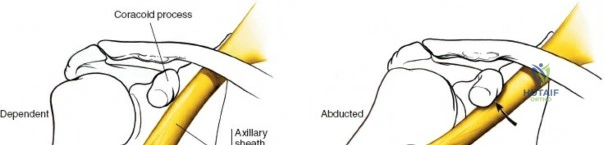
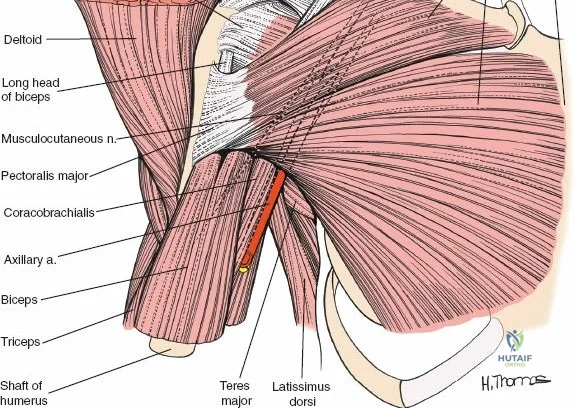
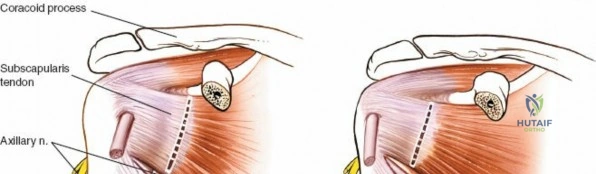
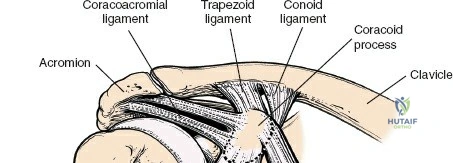
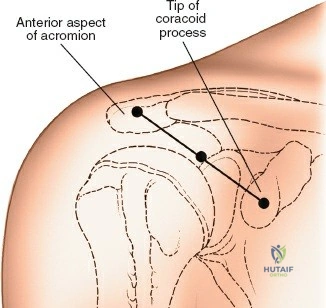
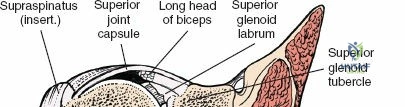
A profound understanding of the surgical anatomy of the shoulder girdle is paramount for safe and effective surgical intervention. The osteology of the region dictates the functional biomechanics; the glenoid is typically retroverted by approximately 2 to 5 degrees, while the proximal humeral head exhibits a retroversion of roughly 30 degrees relative to the transepicondylar axis of the distal humerus. This geometric alignment is critical to restore during arthroplasty or fracture fixation to prevent postoperative instability or impingement. The coracoid process, often referred to as the "lighthouse of the shoulder," serves as a crucial anatomical landmark pointing anterolaterally. It provides the origin for the short head of the biceps and the coracobrachialis (the conjoint tendon), as well as the insertion for the pectoralis minor, defining the medial boundary of the safe zone during anterior approaches.
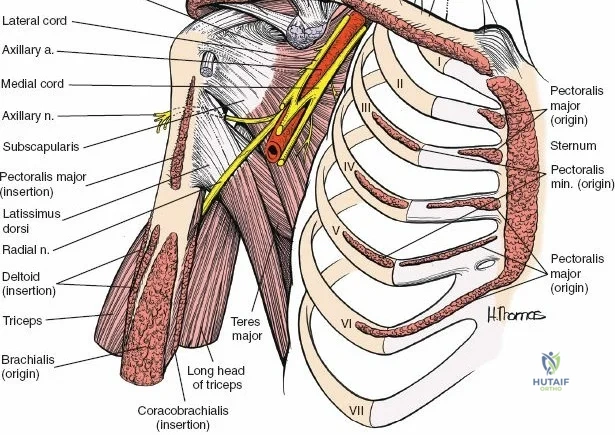
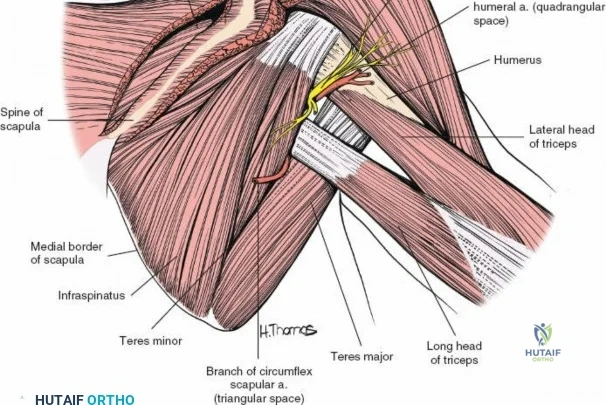
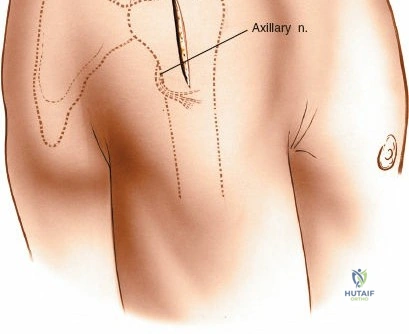
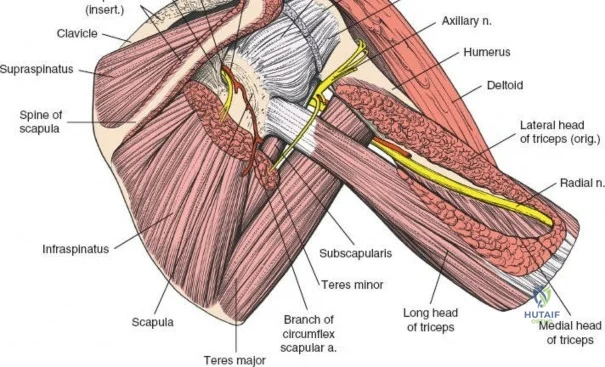
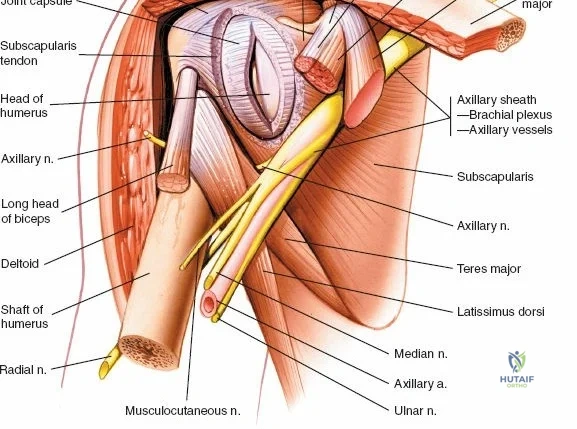
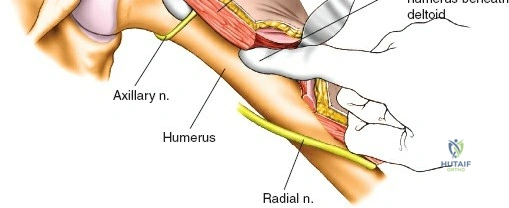
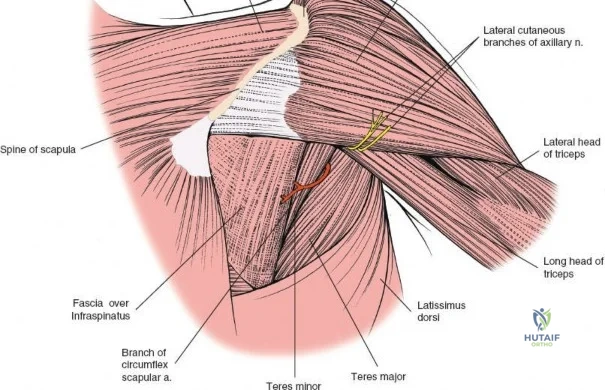
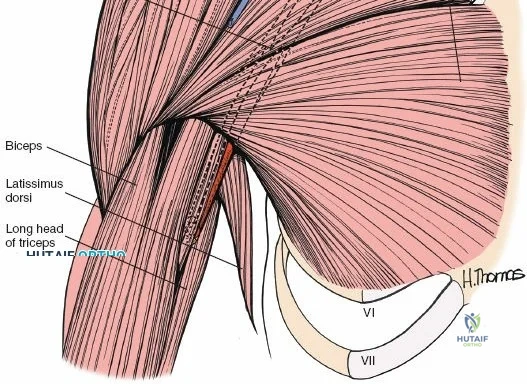
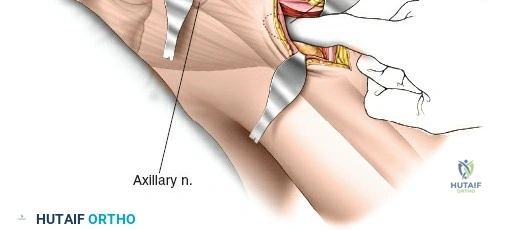
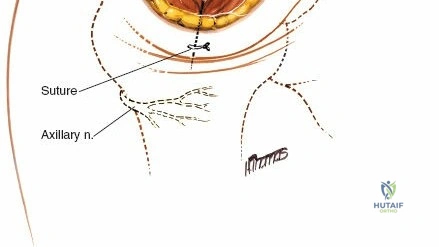
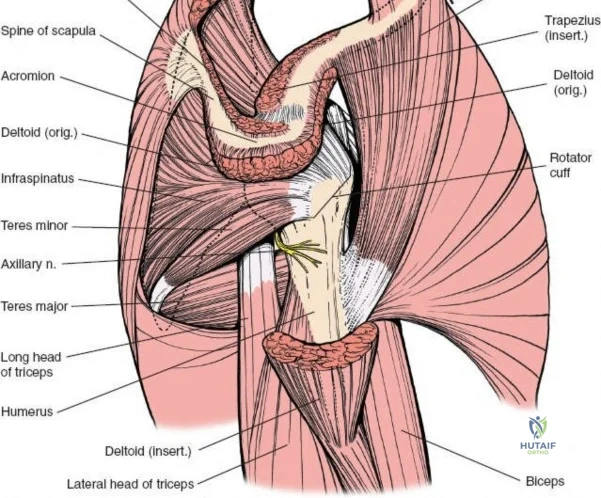
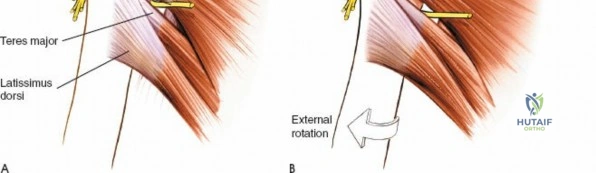
The neurovascular anatomy surrounding the shoulder is dense, highly variable, and exceptionally unforgiving of surgical error. The brachial plexus and the axillary artery transition from the neck into the axilla, passing posterior to the clavicle and medial to the coracoid process. The axillary nerve, a terminal branch of the posterior cord, is of particular concern during lateral and posterior approaches. It exits the axilla through the quadrangular space—bounded by the teres minor superiorly, the teres major inferiorly, the long head of the triceps medially, and the surgical neck of the humerus laterally. It then courses circumferentially around the deep surface of the deltoid, typically lying 5 to 7 centimeters distal to the lateral edge of the acromion. Violation of this structure results in catastrophic loss of deltoid function and profound shoulder dysfunction.
The vascular supply to the proximal humerus is another critical anatomical consideration, particularly in the context of fracture management. The anterior circumflex humeral artery (ACHA) and the posterior circumflex humeral artery (PCHA) form an anastomotic ring around the surgical neck. Historically, the ascending branch of the ACHA (the arcuate artery of Laing) was considered the primary blood supply to the humeral head. However, contemporary microvascular studies have demonstrated that the PCHA provides the dominant intraosseous vascularity to the humeral head. Preservation of the posteromedial hinge during proximal humerus fracture fixation is therefore vital to maintain this blood supply and mitigate the risk of avascular necrosis.
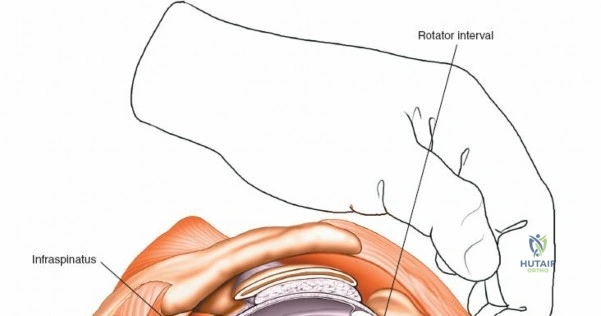
Biomechanically, the shoulder operates through a complex system of force couples. In the coronal plane, the inferiorly directed pull of the rotator cuff counterbalances the superiorly directed shear force of the deltoid, allowing for smooth concentric rotation of the humeral head within the glenoid fossa. In the transverse/axial plane, the anterior pull of the subscapularis is balanced by the posterior pull of the infraspinatus and teres minor. Surgical approaches must respect these force couples. For instance, aggressive tenotomy or failure to meticulously repair the subscapularis during an anterior approach can lead to anterior instability, weakness in internal rotation, and catastrophic failure of total shoulder arthroplasty components due to eccentric anterior loading.
Exhaustive Indications and Contraindications
The decision to proceed with an open surgical approach to the shoulder requires a rigorous assessment of the underlying pathology, the patient's physiological status, and the technical demands of the required reconstruction. The anterior deltopectoral approach is indicated for a vast array of procedures. It is the gold standard for anatomic total shoulder arthroplasty (TSA) and reverse total shoulder arthroplasty (RTSA), providing the necessary exposure for humeral head resection, glenoid preparation, and component implantation. Furthermore, it is the preferred approach for the Latarjet procedure (coracoid transfer) in cases of recurrent anterior instability with critical glenoid bone loss, as well as for open reduction and internal fixation of complex two-, three-, and four-part proximal humerus fractures where the medial calcar requires direct visualization and reduction.

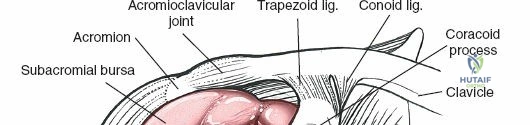
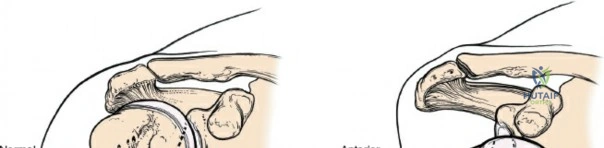
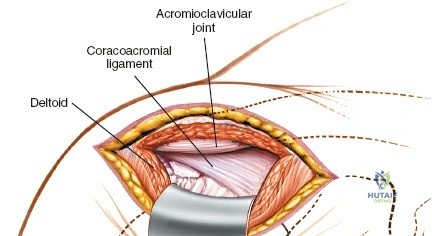
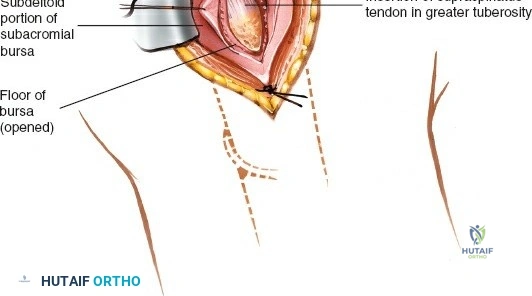
Conversely, the lateral or deltoid-splitting approach is specifically indicated for pathologies localized to the greater tuberosity, the subacromial space, or for the minimally invasive percutaneous plating of specific proximal humerus fractures. It allows direct, orthogonal access to the lateral aspect of the humerus without the need for extensive soft tissue retraction required by the anterior approach. The anterior approach to the clavicle is utilized for ORIF of displaced midshaft clavicle fractures, reconstruction of the acromioclavicular or sternoclavicular joints, and the management of clavicular nonunions or osteomyelitis. The posterior approach is reserved for highly specific indications, primarily the fixation of posterior glenoid rim fractures, excision of posterior labral cysts, and rarely, posterior shoulder arthroplasty in the setting of severe posterior glenoid wear (B2 or C glenoids) where anterior access is deemed insufficient.
Contraindications to these approaches are both absolute and relative. Absolute contraindications include active, untreated focal or systemic infection (unless the approach is specifically for irrigation and debridement), severe medical comorbidities precluding anesthesia, and complete lack of functional deltoid or rotator cuff musculature when an anatomic reconstruction is planned. Relative contraindications involve severe soft tissue compromise, such as extensive burns or prior radiation therapy to the surgical field, which exponentially increases the risk of wound dehiscence and deep infection. In cases of massive, irreparable rotator cuff tears with superior migration of the humeral head, a standard anatomic TSA via an anterior approach is contraindicated; instead, a reverse total shoulder arthroplasty is necessitated.
| Surgical Approach | Primary Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Anterior (Deltopectoral) | TSA/RTSA, Latarjet, Proximal Humerus ORIF, Anterior Capsulorrhaphy | Active local infection (unless I&D), Unfit for anesthesia | Prior extensive anterior radiation, Severe axillary scarring |
| Lateral (Deltoid-Splitting) | Greater tuberosity ORIF, Proximal humerus nailing, Subacromial decompression | Pathology requiring inferior glenoid access | Axillary nerve palsy, Deltoid atrophy |
| Posterior (Judet) | Posterior glenoid ORIF, Scapular neck fractures, Posterior instability | Anterior instability, Anterior glenohumeral pathology | Poor overlying skin envelope, Inability to position laterally |
| Anterior Clavicle | Clavicle ORIF, AC/SC joint reconstruction, Clavicle nonunion | Overlying active cellulitis | Severe osteoporosis (requires modified fixation) |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful shoulder surgery, beginning with a comprehensive suite of radiographic imaging. Standard true anteroposterior (Grashey), scapular Y, and axillary lateral radiographs are mandatory to assess joint congruency, fracture displacement, and glenoid morphology. In contemporary practice, a non-contrast computed tomography (CT) scan with 3D reconstructions is considered the gold standard for evaluating proximal humerus fractures (to assess head-split components and tuberosity displacement) and for preoperative templating in shoulder arthroplasty. Advanced 3D templating software allows the surgeon to map glenoid version, calculate bone loss, and pre-select baseplate and glenosphere sizes, thereby minimizing intraoperative guesswork and optimizing component positioning. Magnetic Resonance Imaging (MRI) remains invaluable for assessing the integrity of the rotator cuff musculature and the degree of fatty infiltration (Goutallier classification), which directly dictates the choice between anatomic and reverse arthroplasty.
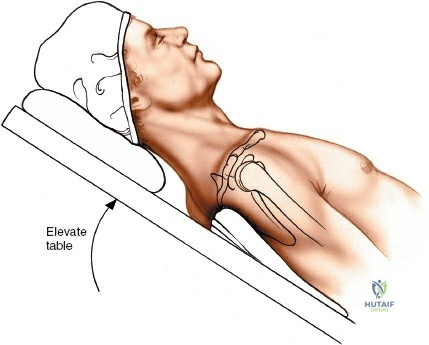
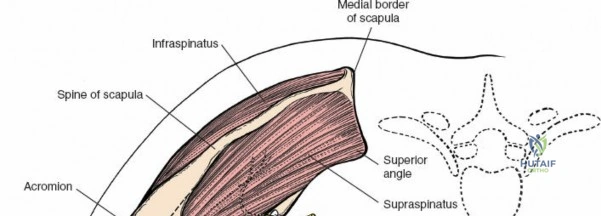
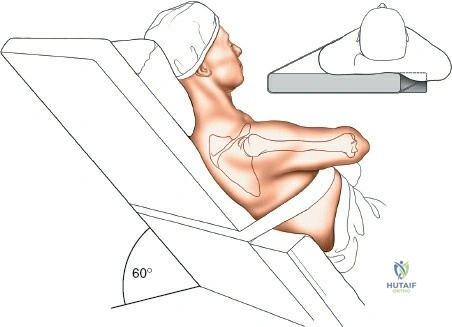
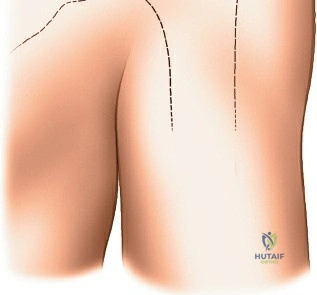
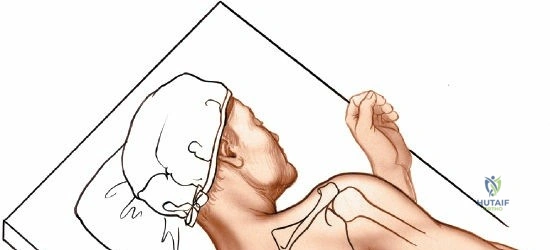
Patient positioning is a critical step that directly impacts the ease of the surgical approach, intraoperative blood loss, and access for fluoroscopy. The two predominant positions utilized for shoulder surgery are the beach chair (modified Fowler) position and the lateral decubitus position. For open anterior and lateral approaches, the beach chair position is almost universally preferred. The patient is placed supine, and the table is broken to elevate the head and torso to approximately 30 to 45 degrees. This elevation is crucial as it reduces venous pressure in the upper extremity, thereby significantly decreasing intraoperative bleeding and keeping the surgical field clear. A sandbag or a specialized scapular bump is placed between the medial border of the scapula and the spine; this maneuver protracts the scapula, allows the shoulder to drop posteriorly, and essentially "opens up" the anterior aspect of the joint.
Careful attention must be paid to the stabilization of the head and neck to prevent catastrophic cervical spine hyperextension or pressure necrosis. If a specialized headrest is utilized, it must be thoroughly padded, ensuring the occiput is protected and the cervical spine remains in a neutral alignment. The operative arm must be draped completely free, allowing for unrestricted manipulation—abduction, adduction, internal, and external rotation—which is absolutely necessary to sequentially expose different aspects of the proximal humerus and glenoid during the procedure. Furthermore, prior to the final sterile prep and drape, the surgeon must ensure that the C-arm fluoroscopy unit can easily access the surgical field and obtain orthogonal views without compromising the sterile boundary.
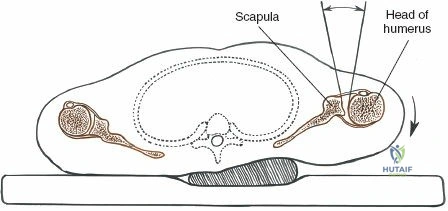
For posterior approaches, the patient is typically placed in the lateral decubitus position with the operative arm suspended using a balanced traction system. This position allows gravity to assist in distracting the glenohumeral joint and provides unobstructed access to the posterior scapula and glenoid. All bony prominences, particularly the contralateral fibular head and greater trochanter, must be meticulously padded to prevent iatrogenic neurapraxia or pressure ulcers during prolonged procedures.
Step-by-Step Surgical Approach and Fixation Technique
Anterior Approach to the Clavicle
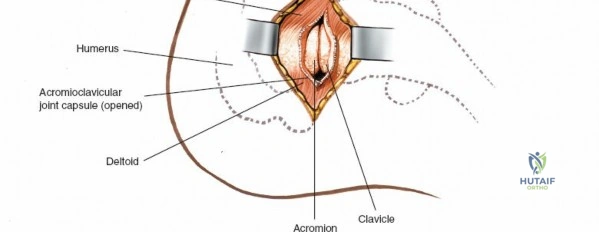
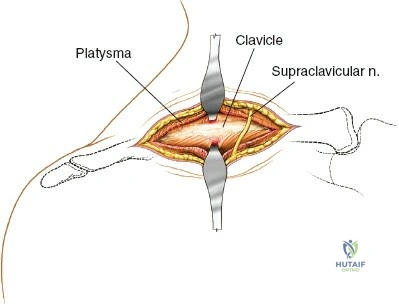
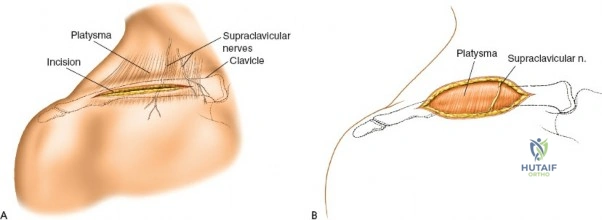
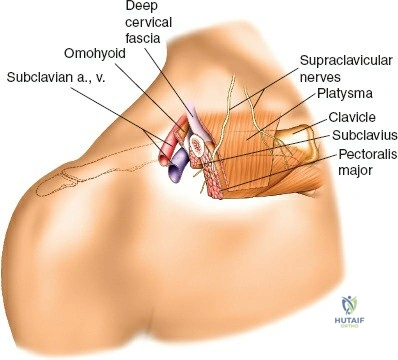
The anterior approach to the clavicle is executed with the patient in the beach chair position. The primary landmarks are the sternal notch medially and the acromioclavicular joint laterally. A longitudinal or slightly oblique incision is made directly over the subcutaneous surface of the clavicle, tailored in length to the specific pathology and the planned implant. The superficial dissection requires traversing the platysma muscle. It is imperative to utilize electrocautery meticulously here, as bleeding from the numerous vessels within the platysma is common and can rapidly obscure the field. The surgeon must be hyper-vigilant regarding the supraclavicular nerves, which branch from the cervical plexus and cross the operative field from superior to inferior. While safe zones exist (within 2.5 cm of the SC joint and 2 cm of the AC joint), division of these nerves in the midshaft region can lead to irritating postoperative chest wall numbness, though significant overlap in cutaneous distribution often mitigates long-term morbidity.
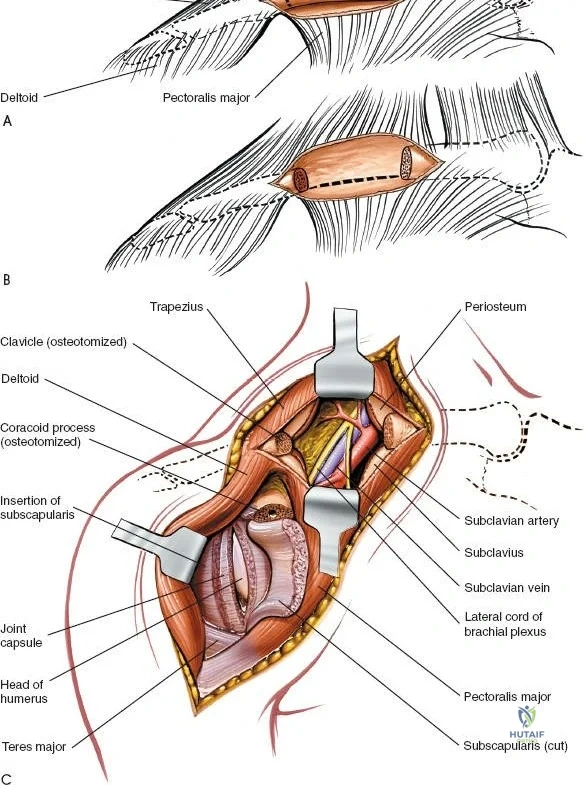
Deep surgical dissection involves incising the clavipectoral fascia and stripping the soft tissues off the clavicle. This must be done in a strict epiperiosteal plane to preserve the periosteal blood supply, which is critical for fracture healing. The surgeon must exercise extreme caution when dissecting inferior and posterior to the middle and medial thirds of the clavicle. The subclavian artery, subclavian vein, and the cords of the brachial plexus lie in perilous proximity to the bone in this region. Over-penetration with a drill bit or careless placement of a bone clamp can result in catastrophic, life-threatening hemorrhage or permanent brachial plexopathy. Fixation is typically achieved using pre-contoured locking plates applied to the superior or anteroinferior surface of the bone, depending on the fracture morphology and biomechanical requirements.
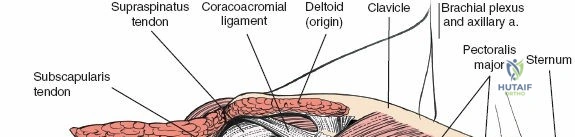
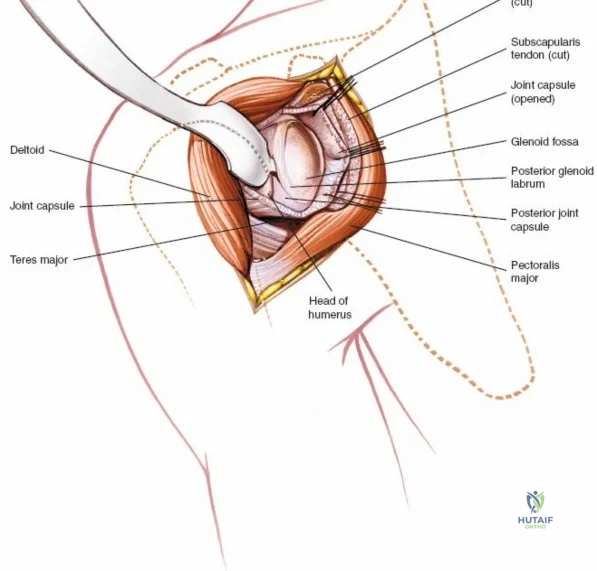
The Deltopectoral Approach to the Anterior Shoulder
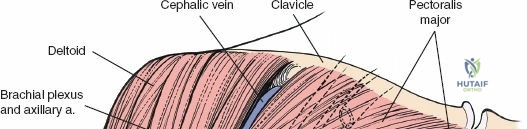
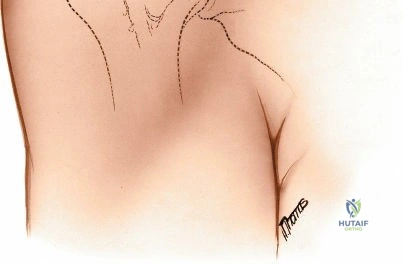
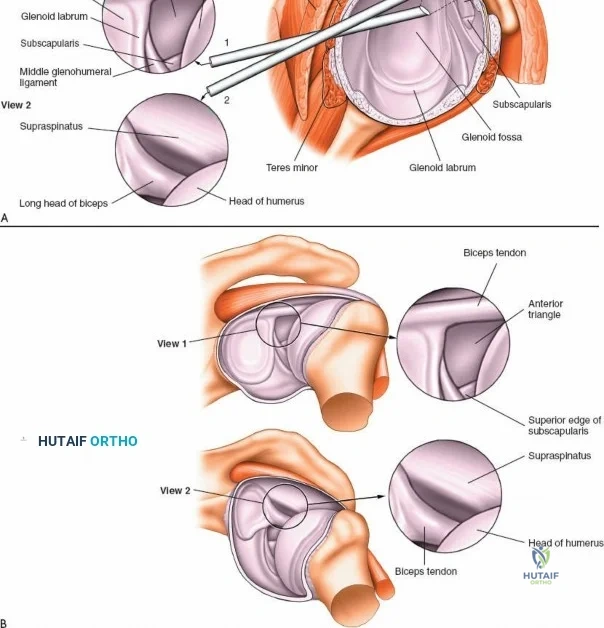
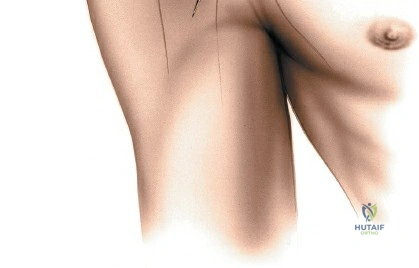
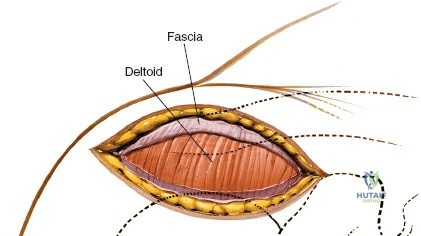
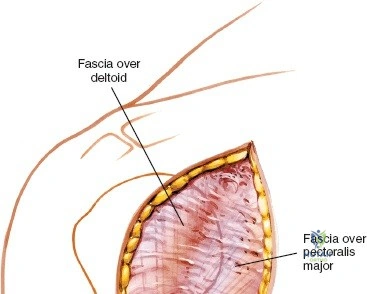
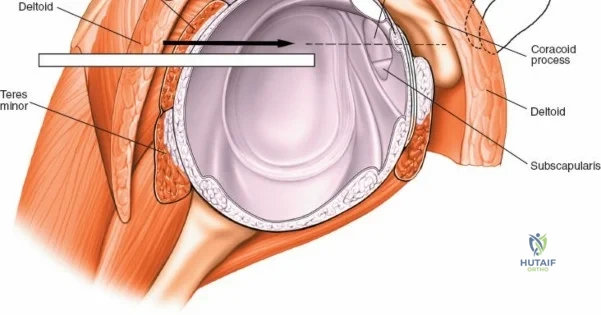
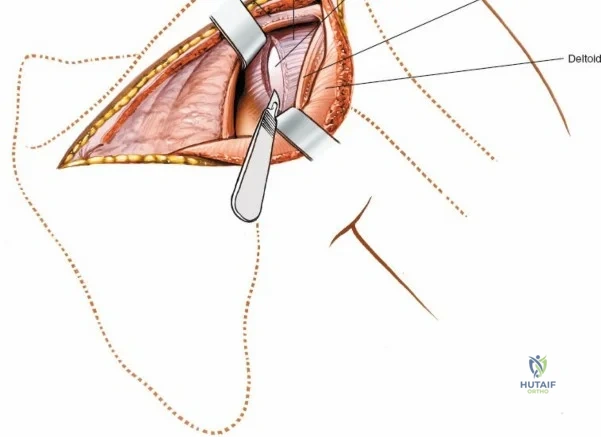
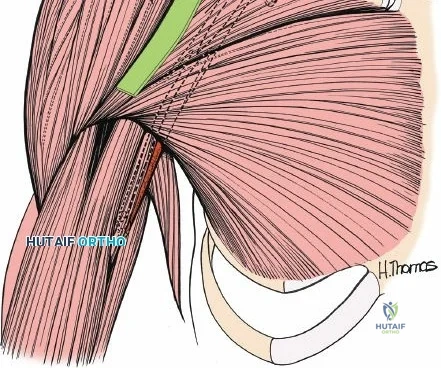
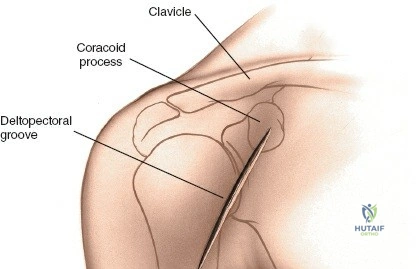
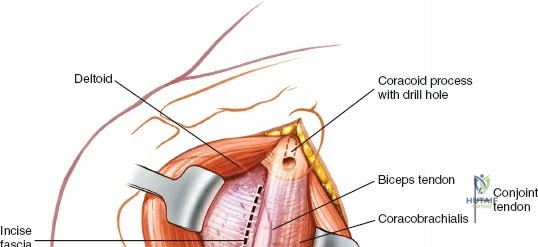
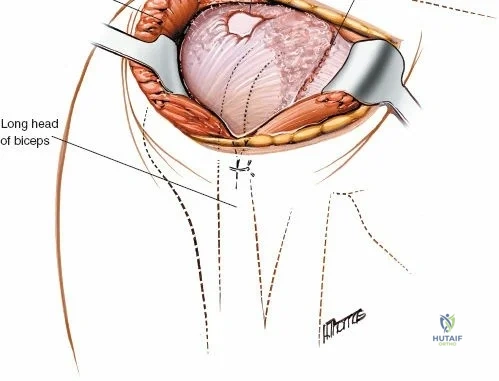
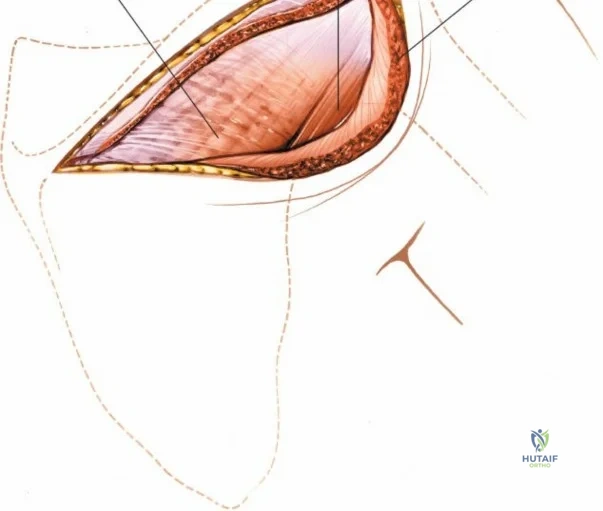
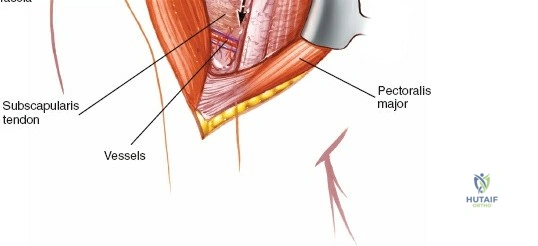
The deltopectoral approach utilizes a true internervous plane, making it exceptionally safe and extensile. The landmarks include the coracoid process, which is palpated in the deepest point of the clavicular concavity, and the deltopectoral groove. The skin incision can be a standard linear incision starting from the coracoid and extending distally toward the deltoid insertion, or a cosmetic axillary incision hidden within the axillary fold. The internervous plane lies between the deltoid muscle (innervated by the axillary nerve from the posterior cord) and the pectoralis major muscle (innervated by the medial and lateral pectoral nerves from the medial and lateral cords, respectively).
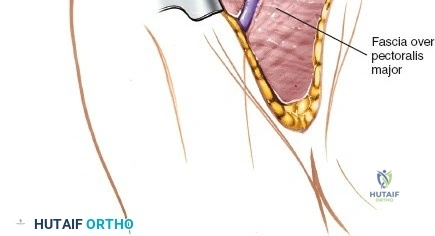
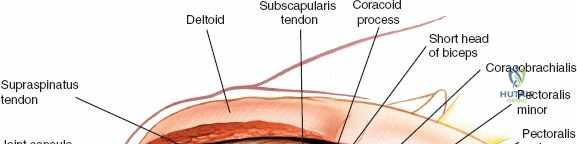
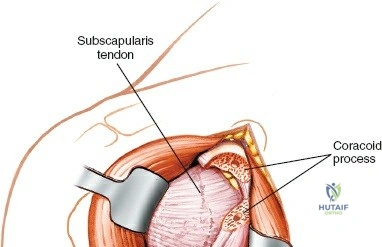
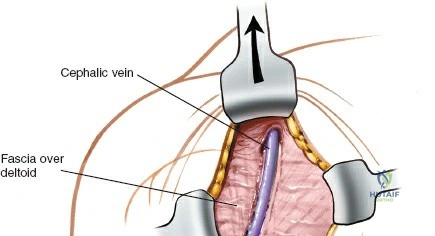
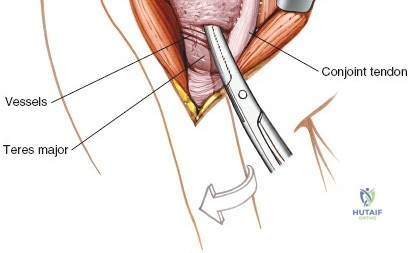
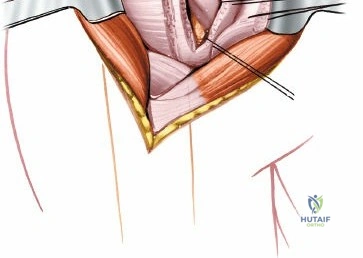
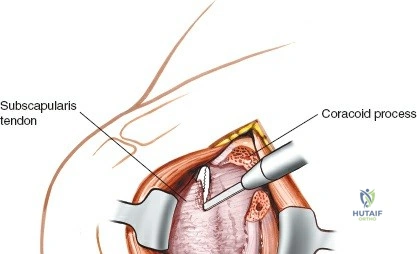
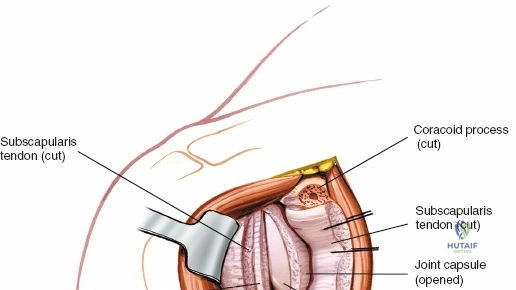
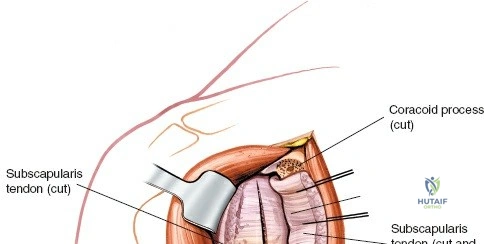
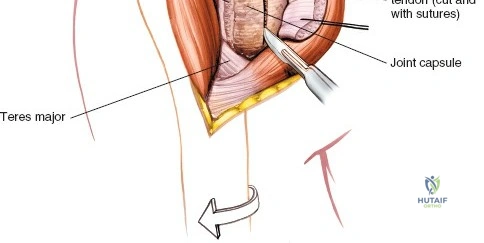
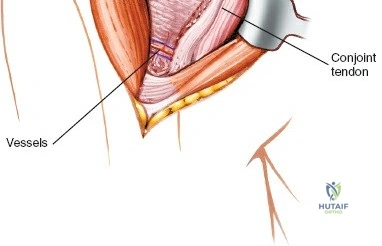
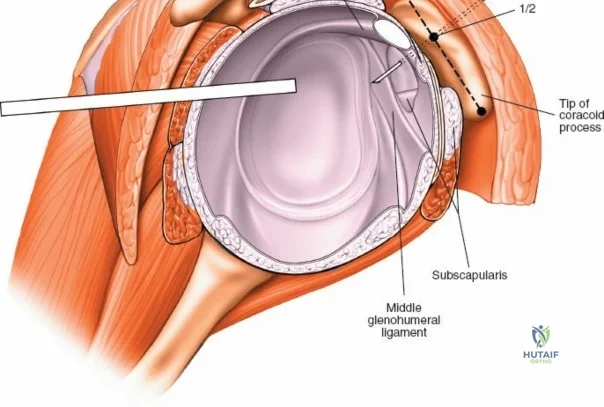
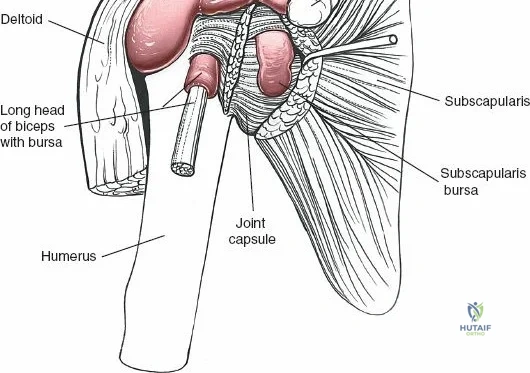
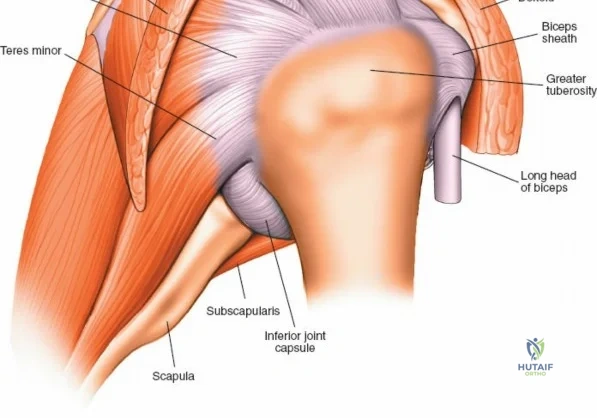
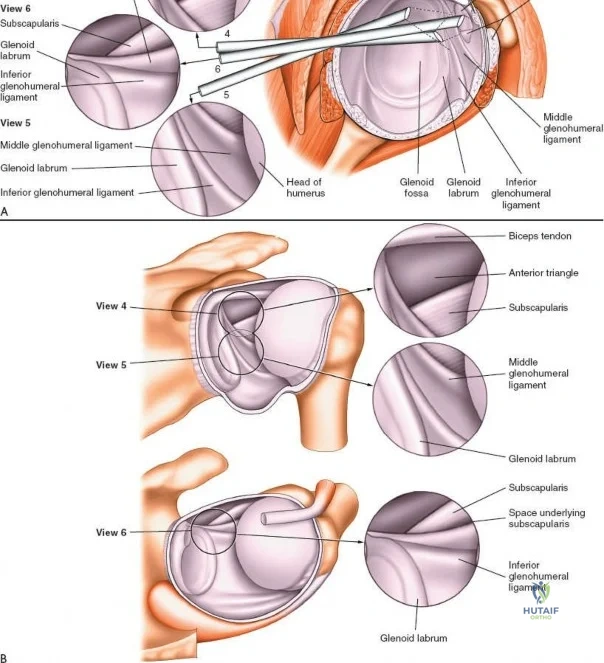
Superficial dissection reveals the cephalic vein, which serves as the primary anatomic beacon for the interval. The vein can be retracted medially or laterally; however, retracting it laterally with the deltoid is generally preferred to preserve its primary venous tributaries from the deltoid muscle, thereby reducing postoperative deltoid edema. Once the interval is developed, the clavipectoral fascia is incised lateral to the conjoint tendon. The conjoint tendon is retracted medially, exposing the subscapularis muscle and the anterior capsule of the shoulder joint. The axillary nerve must be protected inferiorly as it passes across the anterior surface of the subscapularis before diving into the quadrangular space.
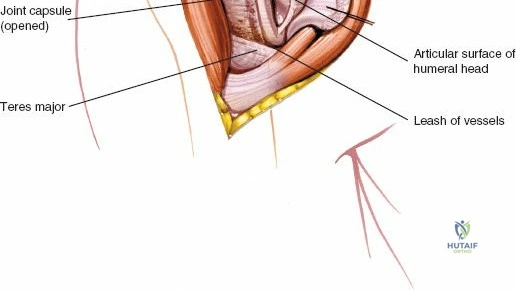
To access the glenohumeral joint, the subscapularis must be managed. This can be achieved via a lesser tuberosity osteotomy, a formal tenotomy, or a subscapularis peel off the bone. The choice depends on the procedure and surgeon preference, but meticulous repair is mandatory to prevent postoperative anterior instability. Once the joint is open, the surgeon has excellent visualization of the humeral head and the anterior glenoid. If deeper inferior access is required, the anterior humeral circumflex vessels (the "three sisters") located at the inferior border of the subscapularis must be identified and ligated to prevent troublesome bleeding.
The Lateral and Posterior Approaches
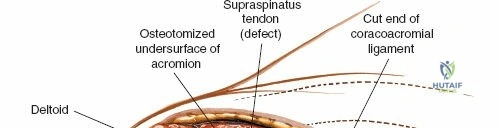
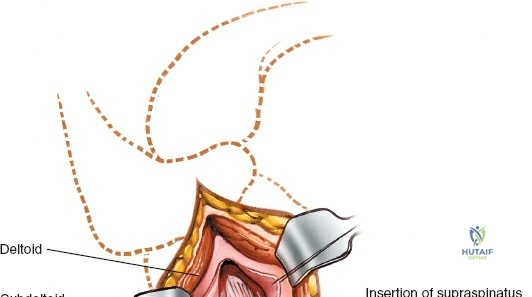
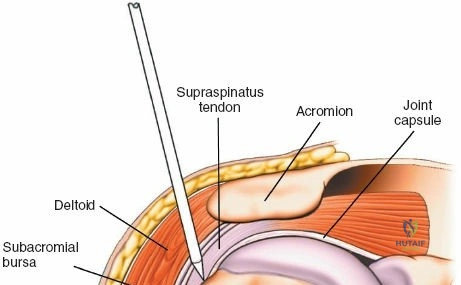
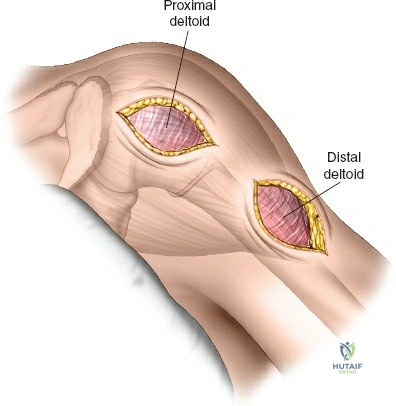
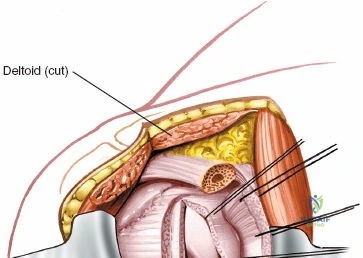
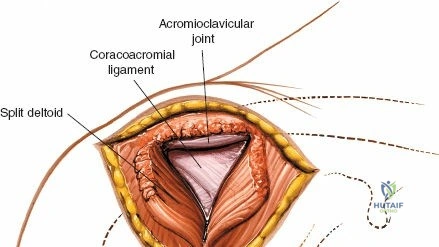
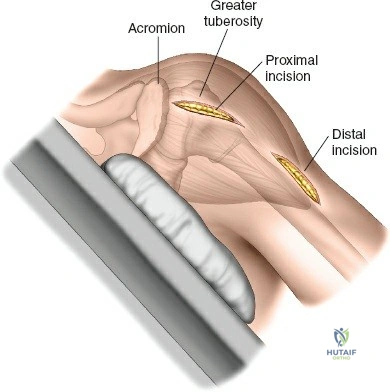
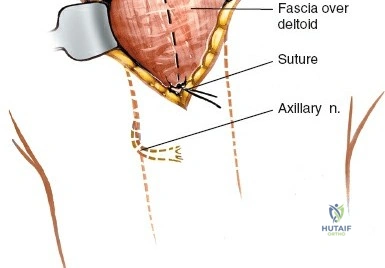
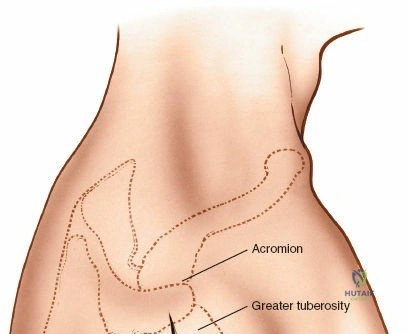
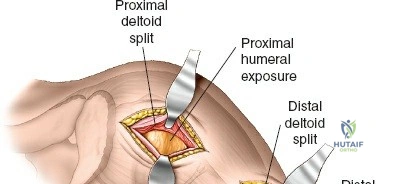
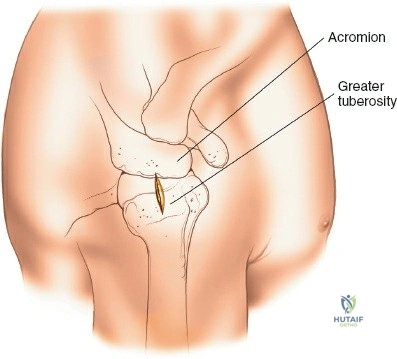
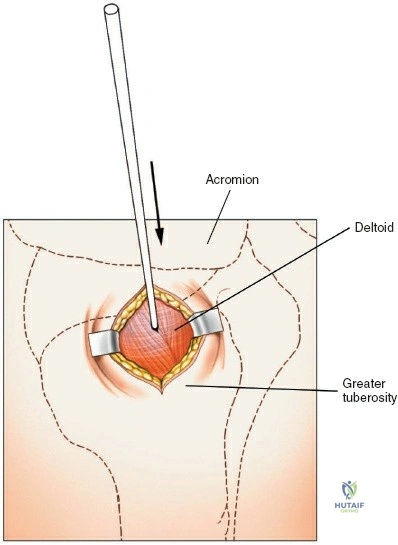
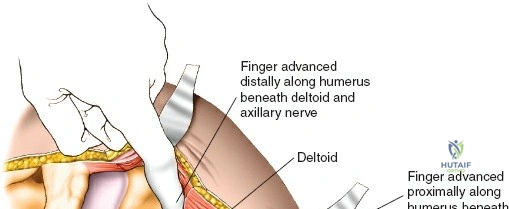
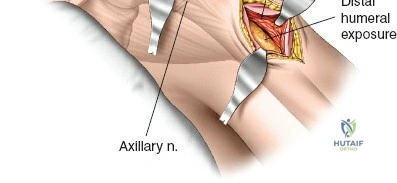
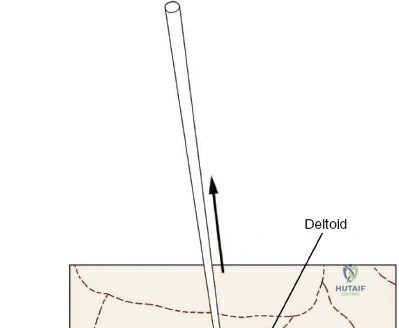
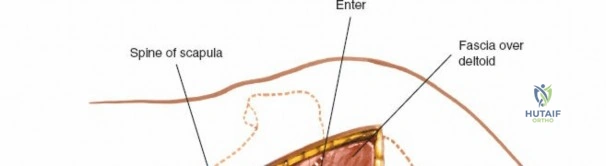
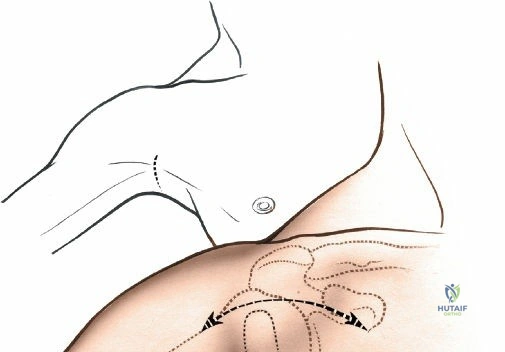
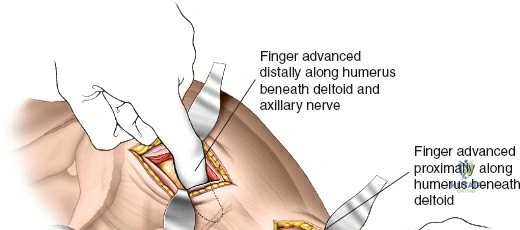
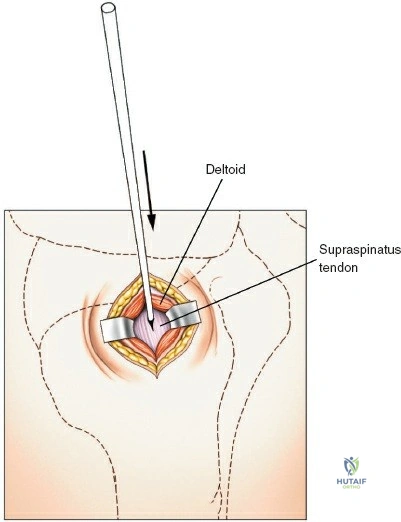
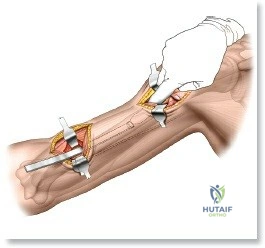
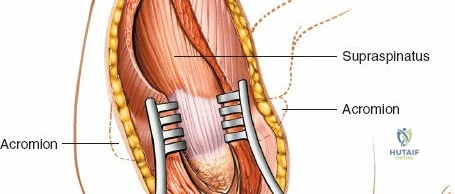
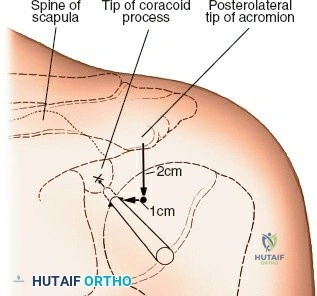
The lateral (deltoid-splitting) approach is utilized primarily for proximal humerus fractures. An incision is made from the lateral edge of the acromion extending distally for no more than 5 centimeters. The deltoid is split in line with its fibers. The critical danger here is the axillary nerve, which crosses the operative field transversely. Dissection distal to 5 cm from the acromion places the nerve at high risk. To extend this approach safely, a second distal window can be created (the minimally invasive anterolateral approach), allowing a plate to be slid submuscularly and secured, thereby bridging the fracture while protecting the axillary nerve in the intervening muscle bridge.

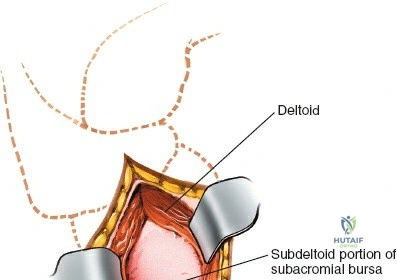
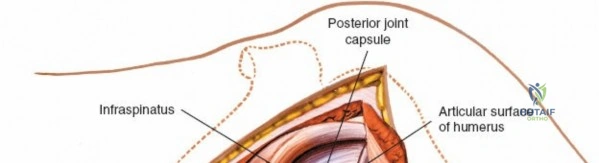
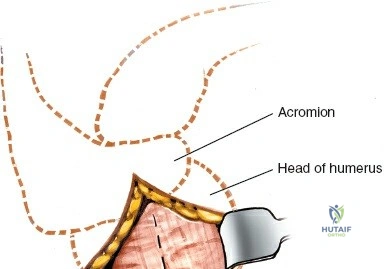
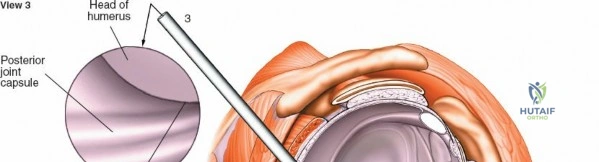
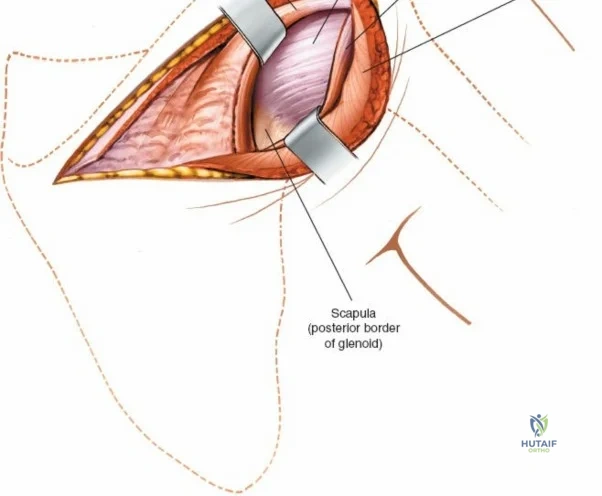
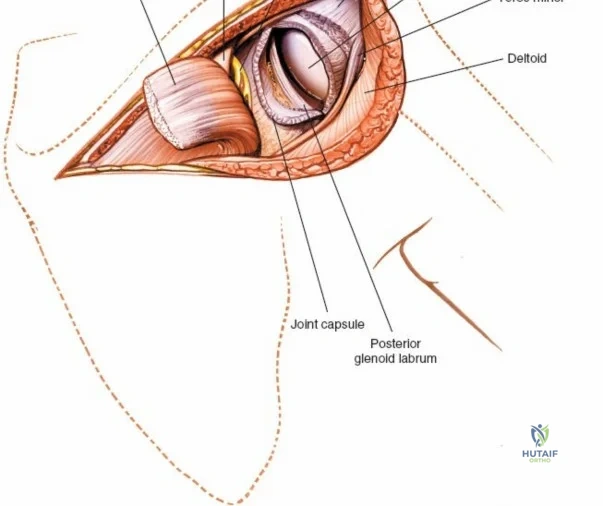
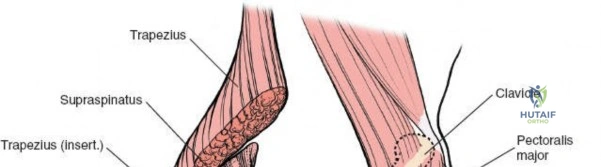
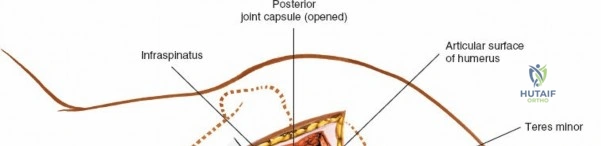
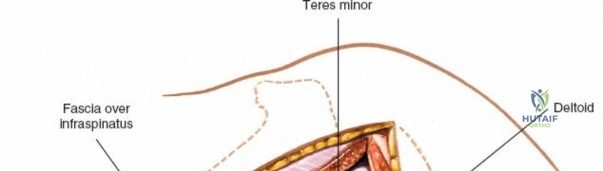
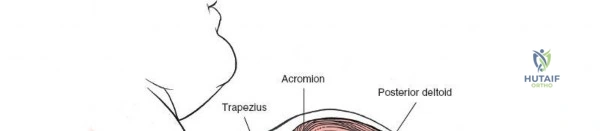
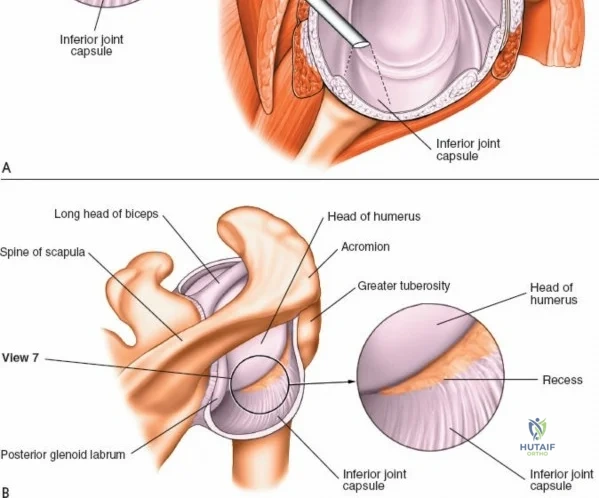
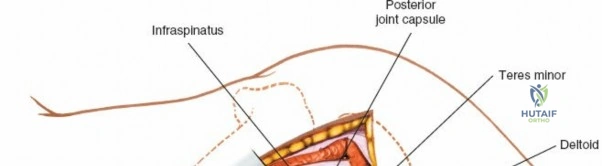
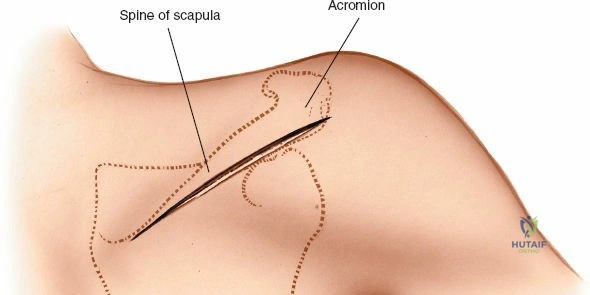
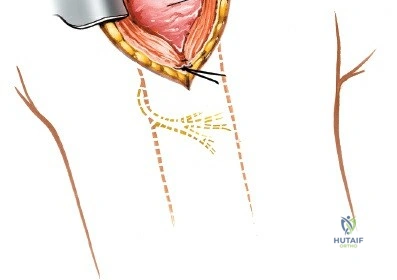
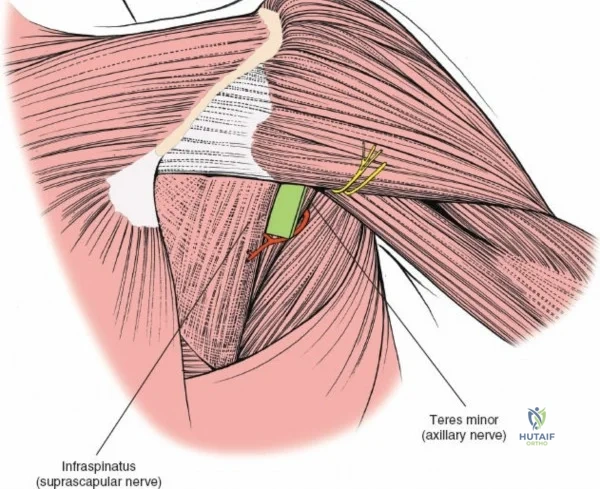
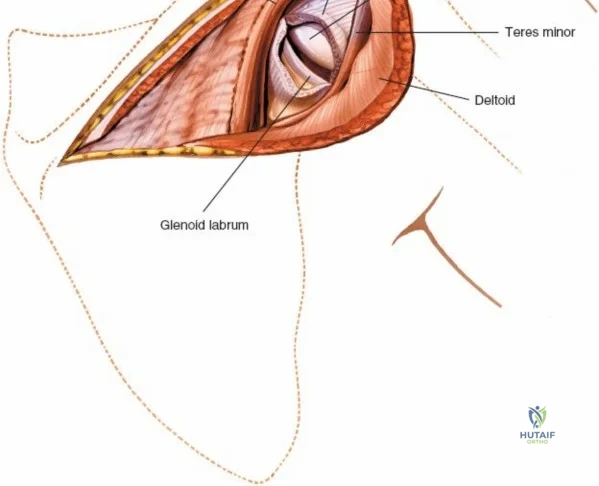
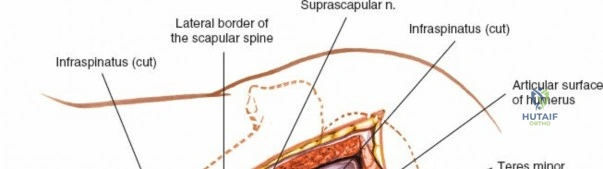
The posterior approach (Judet) involves a curvilinear incision along the spine of the scapula and the posterior border of the deltoid. The deltoid is detached from the scapular spine and retracted laterally and inferiorly. The internervous plane here is between the infraspinatus (suprascapular nerve) and the teres minor (axillary nerve). This approach provides excellent access to the posterior glenoid neck and articular surface. However, the surgeon must be acutely aware of the suprascapular nerve as it passes through the spinoglenoid notch, ensuring retractors are not placed too medially, which could cause a traction neurapraxia.
Complications, Incidence Rates, and Salvage Management
Surgical approaches to the shoulder, while generally safe when executed with anatomical precision, carry inherent risks of severe complications. Neurovascular injury is the most feared complication. The axillary nerve is particularly vulnerable during the lateral deltoid-splitting approach, during inferior capsular release in total shoulder arthroplasty, and during the placement of inferior retractors on the glenoid. The incidence of transient axillary neurapraxia following open shoulder surgery ranges from 1% to 4%, but permanent palsy is catastrophic, resulting in a functionally useless deltoid. The musculocutaneous nerve, which enters the coracobrachialis approximately 5 to 8 cm distal to the coracoid, is at risk during aggressive medial retraction of the conjoint tendon during the deltopectoral approach.
Infection is a devastating complication, particularly following arthroplasty or ORIF. The shoulder is unique due to the high colonization burden of Cutibacterium acnes (formerly Propionibacterium acnes) within the dermal sebaceous glands of the deltopectoral and axillary regions. This indolent, slow-growing, anaerobic gram-positive bacillus is a leading cause of periprosthetic joint infection (PJI) in the shoulder. Standard preoperative skin preparations often fail to eradicate C. acnes residing deep in the dermis. Consequently, the incidence of deep infection ranges from 1% to 3%. Salvage management for deep PJI typically requires extensive irrigation, debridement, hardware or component removal, placement of an antibiotic-impregnated cement spacer, and targeted long-term intravenous antibiotic therapy, followed by a delayed two-stage revision.
Mechanical failures, including hardware pullout, nonunion, and malunion, are frequently encountered in the management of osteoporotic proximal humerus fractures. The incidence of varus collapse and screw cut-out following locked plating can approach 15% to 20% in severe osteoporotic bone. Salvage for a failed proximal humerus ORIF with intra-articular screw penetration or avascular necrosis typically involves conversion to a reverse total shoulder arthroplasty. Postoperative stiffness, or secondary adhesive capsulitis, is another common complication, particularly following extensive trauma or prolonged immobilization. It requires aggressive, phased physical therapy and, in refractory cases, may necessitate arthroscopic capsular release or manipulation under anesthesia.
| Complication | Estimated Incidence | Primary Etiology / At-Risk Step | Salvage / Management Strategy |
|---|---|---|---|
| Axillary Nerve Palsy | 1% - 4% | Lateral approach > 5cm distal; Inferior glenoid retractors | Observation & EMG at 3 mos; Nerve grafting/transfer if no recovery |
| Deep Infection (C. acnes) | 1% - 3% | Arthroplasty/Trauma; Inadequate deep skin prep | I&D, Component removal, Antibiotic spacer, 2-stage revision |
| Subscapularis Failure | 2% - 5% | Poor repair post-deltopectoral approach; Early active IR | Revision repair; Pectoralis major transfer; RTSA conversion |
| Hardware Failure / Varus Collapse | 10% - 20% | Osteoporotic proximal humerus ORIF; Medial calcar comminution | Revision ORIF with fibular strut; Conversion to RTSA |
Phased Post-Operative Rehabilitation Protocols
The success of any open surgical procedure on the shoulder is inextricably linked to the execution of a rigorous, phased postoperative rehabilitation protocol. The shoulder's reliance on dynamic soft-tissue stabilizers means that surgical repair must be protected while simultaneously preventing the rapid onset of adhesive capsulitis. Rehabilitation is generally divided into four distinct phases. Phase 1 (Weeks 0-4) is the maximum protection phase. The patient is typically immobilized in a sling or abduction orthosis. Therapy focuses on strict passive range of
Clinical & Radiographic Imaging Archive