Mastering the Anterior Approach for Tendon of the Long Head Repair
Key Takeaway
Discover the latest medical recommendations for Mastering the Anterior Approach for Tendon of the Long Head Repair. The anterior approach to the shoulder joint is a surgical technique offering wide exposure for repairing anterior, inferior, and superior coverings. This approach is crucial for reconstructing recurrent dislocations, draining sepsis, excising tumors, fixing humerus fractures, and performing shoulder arthroplasties. It also enables effective repair or stabilization of the tendon of the long head of the biceps.
Comprehensive Introduction and Patho-Epidemiology
The anterior surgical approach to the shoulder, universally recognized as the deltopectoral approach, remains the quintessential workhorse corridor for orthopedic surgeons. It provides unparalleled, extensile exposure to the anterior, inferior, and superior aspects of the glenohumeral joint. While its historical roots are deeply embedded in the management of recurrent anterior instability and fracture fixation, its utility has evolved significantly. Today, mastering the anterior approach is absolutely critical for the meticulous repair, stabilization, and tenodesis of the tendon of the long head of the biceps (LHB), as well as the management of concomitant subscapularis pathology.
Pathology of the long head of the biceps is rarely an isolated clinical entity; it is frequently inextricably linked to rotator cuff disease, particularly involving the subscapularis and supraspinatus tendons. The LHB acts as a dynamic depressor of the humeral head, though its exact biomechanical necessity remains a topic of academic debate. When the delicate balance of the biceps pulley system—comprising the superior glenohumeral ligament (SGHL), the coracohumeral ligament (CHL), and the distal insertion of the subscapularis—is disrupted, the LHB is prone to medial subluxation, tearing, and profound tendinopathy. Epidemiologically, LHB pathology is identified in up to 60% of patients undergoing surgical intervention for rotator cuff tears.
The anterior approach allows for a comprehensive evaluation of the bicipital groove, the transverse humeral ligament, and the proximal articular margin. Beyond LHB repair, the versatility of this approach permits a myriad of procedures: reconstruction of recurrent dislocations (e.g., Bankart, Latarjet), drainage of septic arthritis, biopsy and wide excision of primary bone or soft tissue tumors, shoulder arthroplasties (anatomic and reverse), and open reduction and internal fixation (ORIF) of complex proximal humerus fractures.
However, the anterior approach is notorious for the substantial bleeding that can occur from the highly vascularized skin and subcutaneous tissues during superficial dissection. Meticulous hemostasis must be achieved before progressing to the deeper fascial layers. Failure to control this superficial bleeding will inevitably obscure critical neurovascular landmarks, thereby endangering their integrity and compromising the surgical outcome.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the topographic and deep surgical anatomy of the anterior shoulder is the bedrock of a safe and effective deltopectoral approach. The surgeon must navigate a complex three-dimensional web of neurovascular structures while preserving the dynamic stabilizers of the glenohumeral joint.
Superficial Topography and Landmarks
The primary palpable landmark for the anterior approach is the coracoid process. To accurately identify this structure, the surgeon should palpate distally approximately 2.5 cm from the anterior edge of the clavicle, at the deepest point of the clavicular concavity. By pressing laterally and posteriorly in an oblique vector, the firm, bony prominence of the coracoid process can be appreciated. Because it lies deep to the anterior fibers of the deltoid and the superior margin of the pectoralis major, it requires firm palpation. The coracoid process faces anterolaterally and serves as the "lighthouse of the shoulder," guiding the surgeon away from the perilous neurovascular structures of the axilla.
The deltopectoral groove is the critical superficial landmark. In muscular or obese patients, the groove is often easier to visualize than to palpate. The cephalic vein, which courses directly within this groove, frequently serves as a visible blue linear guide, provided the subcutaneous fat does not obscure it.
The Internervous Plane
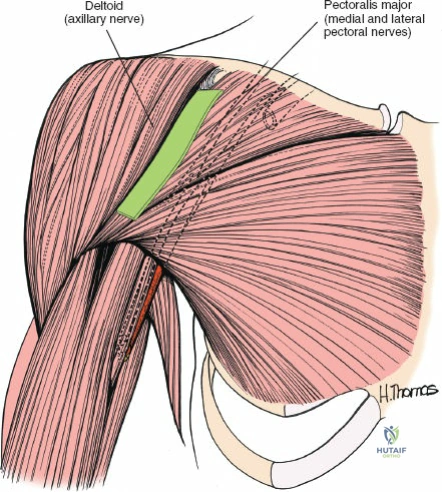
The true elegance of the anterior approach lies in its exploitation of a true internervous plane. This plane resides between the deltoid muscle (innervated by the axillary nerve, a terminal branch of the posterior cord of the brachial plexus) and the pectoralis major muscle (innervated by the medial and lateral pectoral nerves, originating from the medial and lateral cords, respectively). Because these muscles receive their innervation from entirely different cords of the brachial plexus, the plane between them can be developed extensively without risking denervation to either muscle belly.
Deep Neuromuscular Anatomy
Deep to the deltopectoral interval lies the clavipectoral fascia, which envelops the short head of the biceps and the coracobrachialis—collectively known as the conjoined tendon. The musculocutaneous nerve penetrates the coracobrachialis muscle on its medial aspect, typically 5 to 8 cm distal to the tip of the coracoid process. Excessive medial or inferior traction on the conjoined tendon can result in a devastating neurapraxia of the musculocutaneous nerve.
Inferior to the subscapularis muscle, the axillary nerve courses posteriorly through the quadrangular space, accompanied by the posterior circumflex humeral artery. The inferior border of the subscapularis is demarcated by the anterior circumflex humeral vessels, often referred to as the "three sisters" (one artery and two venae comitantes). These vessels must be meticulously identified, ligated, or cauterized to prevent obscuring hemorrhage during deep exposure.
Exhaustive Indications and Contraindications
The decision to utilize the anterior approach must be predicated on a thorough understanding of the patient's pathology, structural demands, and the intrinsic limitations of the surgical corridor. While it is the gold standard for many anterior shoulder pathologies, it is not universally applicable.
| Clinical Parameter | Indications for Anterior Approach | Contraindications |
|---|---|---|
| Biceps Pathology | Irreparable SLAP lesions in older patients, LHB subluxation/dislocation, severe LHB tendinopathy requiring open subpectoral or suprapectoral tenodesis. | Isolated intra-articular LHB fraying amenable to arthroscopic debridement. |
| Rotator Cuff | Massive subscapularis tears, combined subscapularis and supraspinatus tears requiring open mobilization. | Isolated posterior/superior rotator cuff tears (better managed arthroscopically or via mini-open lateral approach). |
| Instability | Recurrent anterior dislocation with significant glenoid bone loss (Latarjet procedure), open Bankart repair (historically). | Isolated posterior instability, multidirectional instability without structural anterior pathology. |
| Trauma | 2-, 3-, and 4-part proximal humerus fractures, anterior glenoid fractures, coracoid fractures. | Scapular body fractures, isolated greater tuberosity fractures displaced posteriorly. |
| Arthroplasty | Total shoulder arthroplasty (TSA), Reverse total shoulder arthroplasty (rTSA), Hemiarthroplasty. | Active profound glenohumeral sepsis (relative contraindication for immediate arthroplasty, requires staged management). |
| Miscellaneous | Biopsy/excision of proximal humerus tumors, open drainage of septic arthritis. | Pathologies requiring strictly posterior glenohumeral access. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning is paramount. For LHB pathology and subscapularis repairs, advanced imaging, specifically Magnetic Resonance Arthrography (MRA), is highly recommended to assess the integrity of the biceps pulley, the degree of subscapularis retraction, and the quality of the muscle belly (Goutallier classification).
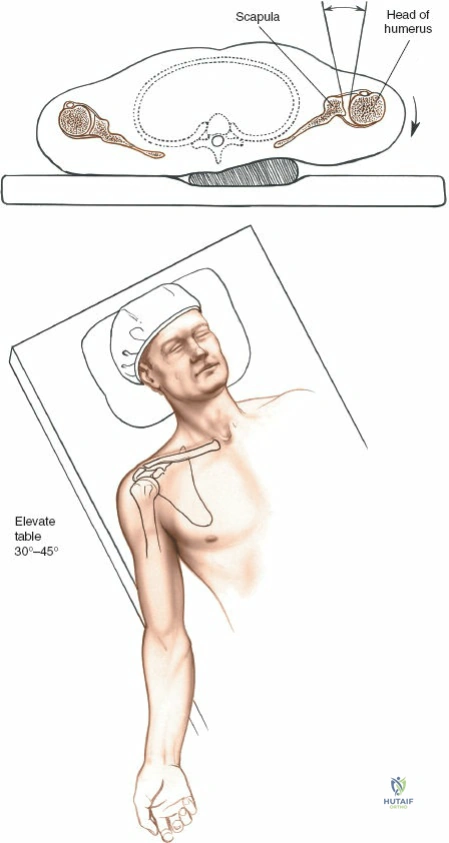
Proper patient positioning dictates the ease of the surgical approach. Place the patient in a supine or modified beach-chair position on the operating table. It is imperative to wedge a sandbag or a specialized scapular bump under the spine and the medial border of the scapula. This maneuver pushes the affected side forward while allowing the arm to fall backward, effectively extending the shoulder and opening up the anterior aspect of the joint.
Elevate the head of the operating table 30 to 45 degrees. This specific elevation is critical to reduce venous pressure, which directly decreases intraoperative bleeding from the cephalic vein and the extensive subcutaneous venous plexus. Furthermore, this incline allows blood to drain away from the operative field, maintaining a pristine view of the deep anatomy. If a headrest is utilized, ensure it is padded meticulously to prevent the development of occipital pressure sores.
The arm must be draped free, utilizing a sterile extremity drape, as it will need to be dynamically manipulated—abducted, adducted, internally, and externally rotated—throughout the procedure to sequentially bring different anatomical structures into the surgical window. If image intensification (fluoroscopy) is anticipated, particularly for fracture fixation or anchor placement verification, the C-arm must be brought in prior to prepping and draping to confirm that unobstructed orthogonal views of the proximal humerus and glenoid can be obtained.
Step-by-Step Surgical Approach and Fixation Technique
The execution of the anterior approach requires a systematic, layered dissection, respecting the fascial planes and neurovascular boundaries.
Incision and Superficial Dissection
The anterior aspect of the shoulder can be approached through two primary skin incisions, dictated by the patient's body habitus, the required extensility of the procedure, and cosmetic considerations.
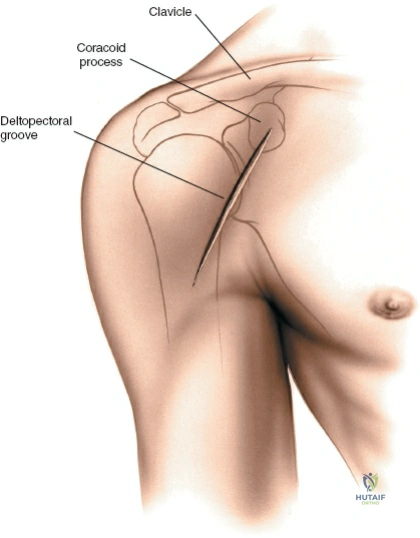
The Standard Anterior Incision: Make a 10- to 15-cm straight or gently curved incision, precisely following the line of the deltopectoral groove. The incision should commence just superior to the coracoid process and extend distally toward the deltoid tuberosity. This provides the most direct and extensile access to the anterior humerus and is the preferred incision for fracture fixation and arthroplasty.
The Axillary Incision: For procedures strictly involving the LHB, isolated subscapularis repair, or cosmetic sensitivity, an axillary incision is highly advantageous. With the patient supine, abduct the shoulder to 90 degrees and rotate it externally. Mark the anterior axillary skin fold with a sterile surgical pen. Make a vertical incision 8 to 10 cm long, starting at the midpoint of the anterior axillary fold and extending posteriorly into the axilla. The skin flaps must be undermined extensively with a finger or blunt dissecting scissors, particularly superiorly in the area of the deltopectoral groove. Use the cephalic vein as a deep guide to ensure correct positioning in the vertical plane. Retract the skin flaps cephalad and laterally so that the mobile window comes to lie directly over the deltopectoral groove.
The axillary incision offers a profound cosmetic advantage as the resulting scar is hidden within the axillary fold and covered by hair. Furthermore, the suture line remains free from tension during healing, minimizing scar hypertrophy. However, this incision is contraindicated in extremely muscular or obese patients where the skin flaps cannot be mobilized adequately, and it is strictly avoided in complex fracture fixation where extensile distal exposure is mandatory.
Managing the Cephalic Vein and Internervous Plane
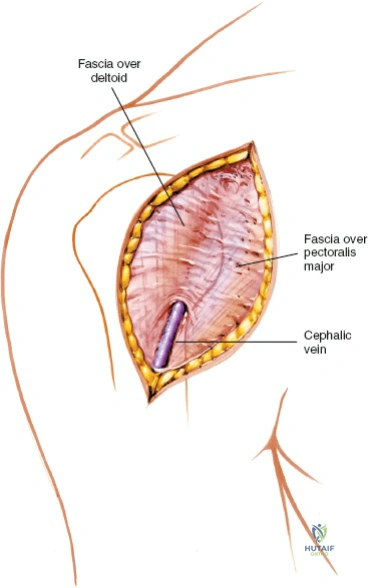
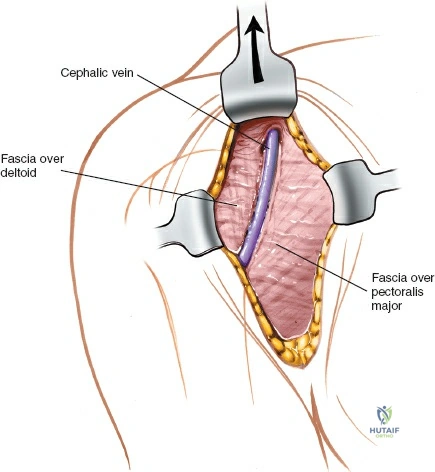
Once the subcutaneous fat is incised, locate the deltopectoral groove. The cephalic vein is the absolute landmark for this interval. It may be difficult to visualize initially as it is often enveloped in a distinct layer of adipose tissue, which paradoxically acts as a reliable guide to its location.
Develop the groove between the fascia overlying the pectoralis major and the fascia overlying the deltoid. The cephalic vein must be mobilized and retracted. The classic debate dictates whether to retract the vein laterally with the deltoid or medially with the pectoralis major. Retracting it laterally takes advantage of the fact that the majority of its venous tributaries originate from the deltoid; thus, lateral retraction minimizes the tearing of these branches. Taking a small, 2-mm cuff of deltoid muscle with the vein can further protect it and reduce the number of bleeding tributaries requiring ligation, though this leaves a microscopic amount of denervated muscle. Regardless of the direction of retraction, the surgeon must strive to preserve the cephalic vein to mitigate postoperative upper extremity venous congestion and edema.
Deep Dissection and Coracoid Management
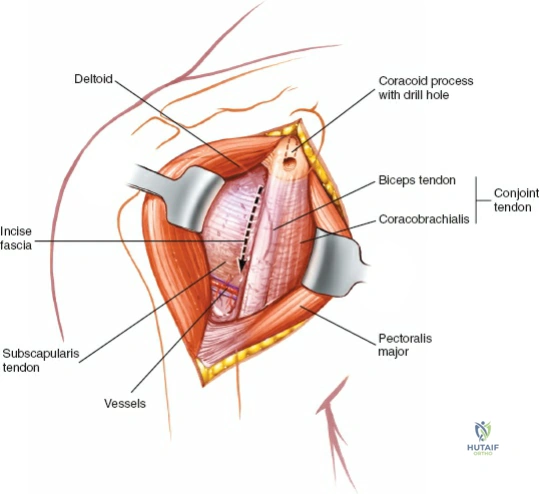
Retract the pectoralis major medially and the deltoid laterally, utilizing self-retaining retractors (e.g., Gelpi or Kolbel retractors). This exposes the clavipectoral fascia. Incise this fascia lateral to the conjoined tendon (the short head of the biceps and the coracobrachialis).
These muscles must be displaced medially to gain access to the anterior aspect of the shoulder joint. For procedures such as LHB tenodesis, subscapularis repair, or standard arthroplasty, simple medial retraction with a Richardson or Hohmann retractor is sufficient.
Historically, and in cases requiring massive exposure (e.g., complex tumor resections or the classic Magnuson-Stack and Putti-Platt procedures), the conjoined tendon was detached via a coracoid osteotomy. If this is deemed necessary, the tip of the coracoid process must be pre-drilled and tapped before the osteotomy is performed with a sharp osteotome. Failure to pre-drill will result in the small bone fragment splitting during subsequent reattachment, making anatomic reduction exceedingly difficult.
Crucially, the axillary artery and the cords of the brachial plexus lie directly posterior to the pectoralis minor muscle and medial to the coracoid. Abduction of the arm places these neurovascular structures under tension, bringing them dangerously close to the tip of the coracoid and the operative field. Therefore, the arm must be kept strictly adducted while dissecting around the coracoid process to protect the axillary sheath.
Divide the fascia that fans out from the conjoined tendon on the lateral side of the coracobrachialis. This is the "safe side" of the muscle, as the musculocutaneous nerve enters the coracobrachialis on its medial aspect. Apply gentle medial retraction; overzealous downward or medial retraction with a rigid instrument can easily cause a traction neurapraxia of the musculocutaneous nerve.
Subscapularis Takedown and Joint Exposure
Beneath the conjoined tendon lie the transversely oriented fibers of the subscapularis muscle, the primary anterior dynamic stabilizer of the glenohumeral joint. As the muscle crosses the anterior glenoid rim, a bursa separates it from the joint capsule.
To expose the LHB and the joint, the arm is externally rotated. This maneuver stretches the subscapularis, bringing its tendinous insertion on the lesser tuberosity into prominent view and increasing the distance between the inferior border of the muscle and the axillary nerve. The inferior border is reliably identified by the aforementioned "three sisters" (anterior circumflex humeral vessels), which run transversely and must be meticulously ligated or coagulated with bipolar electrocautery. The superior border of the subscapularis is less distinct, blending intimately with the coracohumeral ligament and the anterior edge of the supraspinatus tendon, forming the rotator interval.
For access to the joint, the subscapularis can be managed in several ways: a vertical tenotomy 1-2 cm medial to its insertion, a subscapularis peel directly off the lesser tuberosity, or a lesser tuberosity osteotomy (LTO). If a tenotomy is performed, tag the medial tendon edge with heavy non-absorbable stay sutures immediately to prevent it from retracting medially out of the surgical field. Pass a blunt instrument (e.g., a Kelly clamp or elevator) between the capsule and the subscapularis, moving from inferior to superior, to separate the layers if a capsule-preserving approach is desired.
Long Head of the Biceps Tenodesis and Repair
With the subscapularis managed and the rotator interval opened, the bicipital groove is fully exposed. The LHB is identified within the groove, held in place by the transverse humeral ligament.
To perform the tenodesis, the transverse humeral ligament is incised longitudinally. The LHB is elevated from the groove using a right-angle clamp. The tendon is inspected for hypertrophy, partial tearing, and synovitis. The tendon is then tagged with a locking whipstitch (e.g., Krackow technique) using high-tensile strength suture. The proximal portion of the tendon is sharply excised at its origin on the superior glenoid tubercle (if not already torn).
The surgeon must then choose between a suprapectoral or subpectoral tenodesis. For a suprapectoral tenodesis within the anterior approach, the bicipital groove is decorticated to a bleeding bone bed. A pilot hole is drilled in the floor of the groove. The whipstitched tendon is tensioned appropriately (restoring the physiologic length-tension relationship) and secured into the osseous socket using a biocomposite interference screw or cortical button fixation.
Following the tenodesis, the subscapularis must be meticulously repaired to its anatomic footprint. If a tenotomy was performed, a robust tendon-to-tendon or tendon-to-bone repair utilizing suture anchors is executed. The arm is taken through a full range of motion to confirm the security of the tenodesis and the subscapularis repair, ensuring no impingement or undue tension exists.
Complications, Incidence Rates, and Salvage Management
Despite its ubiquity, the anterior approach carries inherent risks. A profound knowledge of potential complications is mandatory for the operating surgeon.
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| Musculocutaneous Nerve Palsy | 1% - 3% | Prevention: Avoid rigid, prolonged medial retraction of the conjoined tendon. Release retractors periodically. Management: Typically a traction neurapraxia that resolves spontaneously over 3-6 months. Baseline EMG at 6 weeks if no clinical improvement. |
| Axillary Nerve Injury | < 1% | Prevention: Identify the inferior border of the subscapularis accurately. Keep dissection superior to the "three sisters." Management: Intraoperative primary repair if transected. Postoperative observation for neuropraxia; nerve grafting/transfer if no recovery by 3-6 months. |
| Cephalic Vein Thrombosis/Laceration | 5% - 10% | Prevention: Careful mobilization, taking a small cuff of deltoid. Management: If lacerated, ligate proximally and distally. Postoperative edema is usually transient and managed with elevation and compression. |
| Subscapularis Failure | 2% - 8% | Prevention: Robust, anatomic repair using high-strength sutures and anchors. Strict adherence to postoperative internal rotation and passive external rotation limits. Management: Revision repair, pectoralis major transfer, or reverse total shoulder arthroplasty depending on patient age and joint status. |
| "Popeye" Deformity (Failed Tenodesis) | 3% - 5% | Prevention: Secure cortical or interference screw fixation. Proper tensioning of the LHB prior to fixation. Management: Often cosmetic with minimal functional deficit. Revision tenodesis is rarely indicated unless accompanied by severe cramping pain. |
| Hematoma Formation | 2% - 4% | Prevention: Meticulous hemostasis of the anterior circumflex vessels and deltoid branches prior to closure. Use of a closed suction drain if oozing persists. Management: Evacuation if expanding or causing neurological compromise; otherwise, conservative observation. |
Phased Post-Operative Rehabilitation Protocols
The rehabilitation following an anterior approach for LHB tenodesis and concomitant subscapularis repair must delicately balance tissue healing with the prevention of glenohumeral stiffness. The protocol is heavily dictated by the security of the subscapularis repair.
Phase I: Maximal Protection (Weeks 0-4)
The patient is immobilized in a sling with an abduction pillow. The primary goal is protection of the subscapularis repair and the biceps tenodesis. Active internal rotation and active elbow flexion/supination are strictly prohibited. Passive forward elevation is allowed in the scapular plane up to 90 degrees. Passive external rotation is strictly limited to neutral (0 degrees) to prevent catastrophic tension on the subscapularis footprint.
Phase II: Moderate Protection and Active Motion (Weeks 4-8)
The sling is gradually discontinued. Active-assisted range of motion (AAROM) is initiated. External rotation is slowly progressed by 10-15 degrees per week, guided by the intraoperative safe zone determined by the surgeon. Light, active elbow flexion and supination can commence, but resisted biceps activity remains contraindicated. Isometrics for the deltoid and intact rotator cuff are introduced.
Phase III: Early Strengthening (Weeks 8-12)
Once full, painless passive range of motion is achieved, active internal rotation strengthening begins. Isotonic strengthening of the rotator cuff and periscapular stabilizers (rhomboids, serratus anterior, trapezius) is initiated using low-resistance elastic bands. Biceps strengthening (light curls) can be incorporated, monitoring for any pain at the bicipital groove.
Phase IV: Advanced Strengthening and Return to Activity (Weeks 12-24+)
The focus shifts to dynamic stabilization, plyometrics, and sport-specific or work-specific functional training. Heavy lifting and overhead athletic activities are gradually reintroduced. Full return to contact sports or heavy manual labor is typically cleared between 5 and 6 months postoperatively, contingent upon symmetrical strength and the absence of apprehension or pain.
Summary of Landmark Literature and Clinical Guidelines
The evolution of the anterior approach and the management of LHB pathology is deeply rooted in landmark orthopedic literature.
Historically, the anatomic descriptions by Henry (1957) established the internervous planes that remain the foundation of the deltopectoral approach. Regarding the management of the subscapularis during this approach, Gerber et al. (2005) demonstrated the critical importance of anatomic subscapularis repair, showing that failure to restore the footprint leads to profound kinematic alterations and anterior instability. The shift toward lesser tuberosity osteotomy (LTO) in arthroplasty was championed by Gerber and others, demonstrating superior bone-to-bone healing rates compared to soft-tissue tenotomy, though recent meta-analyses show excellent outcomes with both techniques when performed meticulously.
In the realm of LHB pathology, the debate between tenotomy and tenodesis was heavily influenced by Boileau et al. (2007), who found that while both effectively relieve pain, tenodesis prevents the cosmetic "Popeye" deformity and fatigue cramping associated with tenotomy, making it the preferred procedure in younger, active patients. Furthermore, biomechanical studies by Mazzocca et al. (2005) validated the pull-out strength of subpectoral interference screw fixation, establishing it as a biomechanically superior construct for maintaining the length-tension relationship of the biceps muscle belly.
Clinical guidelines currently dictate that the anterior approach remains the gold standard for open LHB tenodesis, particularly when concomitant subscapularis pathology or massive rotator cuff tearing necessitates open mobilization and structural repair. The mastery of this approach is not merely a surgical requirement but an art form that defines the proficient shoulder surgeon.
