Masterclass in Operative Foot and Ankle Surgery: Endoscopic Plantar Fasciotomy and Achilles Tendinopathy
Key Takeaway
The two-portal endoscopic plantar fascia release offers a minimally invasive approach to recalcitrant plantar fasciitis. By utilizing precise portal placement and transillumination, surgeons can safely transect the medial band while protecting neurovascular structures. Concurrently, managing insertional Achilles tendinopathy requires a deep understanding of watershed vascularity, biomechanics, and the safe limits of tendon debridement, allowing up to fifty percent resection without compromising structural integrity.
ENDOSCOPIC PLANTAR FASCIA RELEASE
Recalcitrant plantar fasciitis that fails to respond to an exhaustive regimen of conservative management—including physical therapy, orthoses, corticosteroid injections, and extracorporeal shock wave therapy—may necessitate surgical intervention. The two-portal endoscopic plantar fascia release has emerged as a highly effective, minimally invasive technique. It provides direct visualization of the plantar fascia while minimizing soft tissue morbidity, thereby accelerating postoperative rehabilitation compared to traditional open approaches.
Surgical Anatomy and Biomechanics
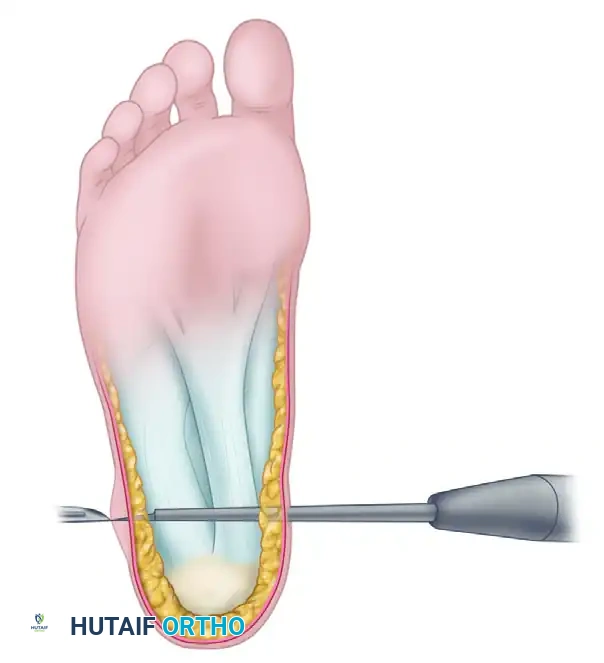
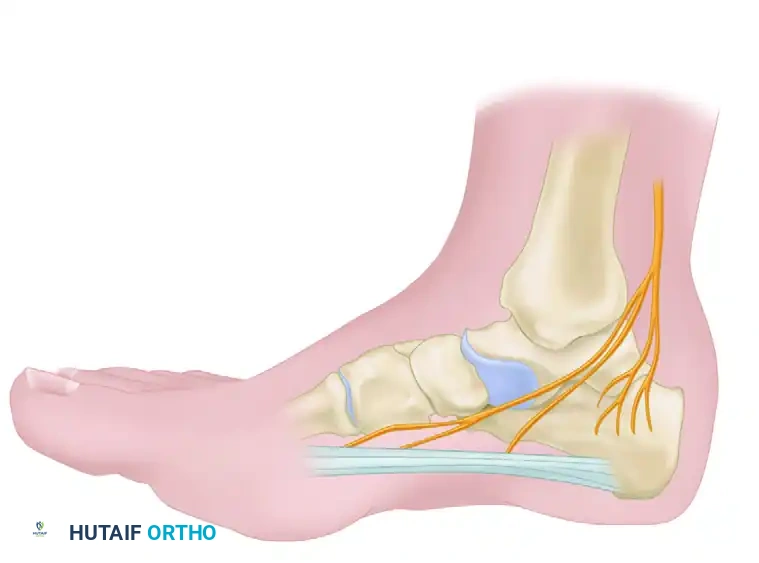
A thorough understanding of the plantar aspect of the foot is paramount to avoid catastrophic neurovascular complications. The plantar fascia is a thickened fibrous aponeurosis originating from the medial tubercle of the calcaneus. It is divided into medial, central, and lateral bands. The central band is the thickest and most commonly implicated in plantar fasciitis.
Surgical Warning: The medial calcaneal nerve and the lateral plantar nerve (specifically the first branch, the nerve to the abductor digiti minimi) are at significant risk during this procedure. Dissection must remain strictly superficial to the intrinsic musculature to prevent iatrogenic nerve injury. Furthermore, transection should be strictly limited to the medial half of the central band; complete release of the plantar fascia severely destabilizes the lateral column of the foot, leading to lateral midfoot pain and acquired flatfoot deformity.
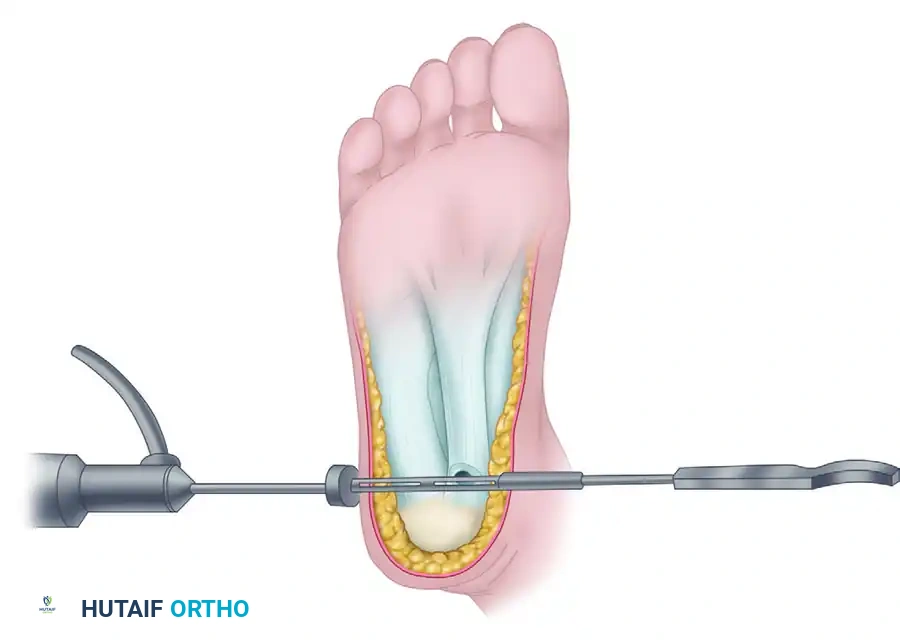
Two-Portal Surgical Technique (Saxena)
The two-portal technique allows for excellent triangulation, transillumination, and precise controlled release of the fascial band.
Step 1: Positioning and Portal Placement
* Place the patient in the supine position with a bump under the ipsilateral hip to allow neutral rotation of the leg.
* Exsanguinate the limb and inflate a thigh or calf tourniquet.
* Identify the medial tubercle of the calcaneus via palpation.
* Make a precise 5-mm incision on the medial aspect of the foot, exactly 1 cm distal to the medial tubercle of the calcaneus, just superior to the junction of the plantar and medial skin.
* Dorsiflex the hallux to place the plantar fascia under tension, making the medial portion easily palpable. The incision should be oriented within the slightly oblique skin lines that run dorsal-proximal to plantar-distal.
Step 2: Dissection and Cannula Insertion
* Utilize a small hemostat to bluntly dissect through the subcutaneous fat down to the superficial surface of the plantar fascia.
* Introduce a fascial elevator to separate the subcutaneous adipose layer from the plantar fascia across the inferior heel.
* Introduce an obturator and slotted cannula assembly from medial to lateral through the pathway created by the elevator. The cannula must remain strictly plantar to the fascia.
Step 3: Endoscopic Visualization and Measurement
* Remove the obturator and insert a 30-degree, 4.0-mm endoscope into the medial portal of the cannula to view the plantar fascia superiorly.
* Withdraw the endoscope and insert a cannulated depth gauge equipped with a stop device. Reintroduce the endoscope alongside the depth gauge from medial to lateral.
* Rotate the slotted cannula 180 degrees to identify the medial half of the central plantar fascia band. Confirm the location externally by observing the transillumination of the endoscope light through the plantar skin of the inferior heel.
* Note the exact measurement on the depth gauge that corresponds to the appropriate level of transection (typically marking 7 to 8 on the gauge).
Step 4: Fascial Transection
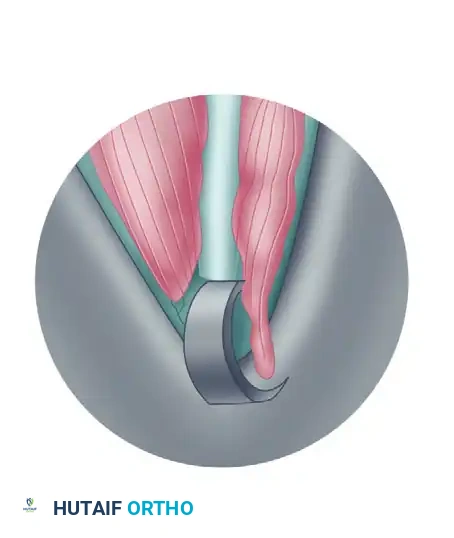
* Withdraw the endoscope and depth gauge. Attach a disposable cannulated hook knife with the stop device set at the previously determined number. This prevents over-penetration and protects the lateral band.
* Reinsert the endoscope. Under direct visualization, use the hook knife to transect the medial half of the central plantar fascia.
* Clinical Pearl: Actively dorsiflexing the toes during this step places the fascia under maximum tension, facilitating a clean, crisp transection.
Step 5: Inspection and Closure
* Following the release, meticulously examine the cut ends of the plantar fascia. The underlying first plantar muscle layer (flexor digitorum brevis) should now be clearly visible.
* If any palpable taut fibers of the medial band remain, use endoscopic scissors to transect them under direct vision.
* Once an adequate fasciotomy is confirmed, remove all instrumentation, thoroughly irrigate the surgical site to remove debris, and close the medial (and lateral, if established) portal with one or two horizontal mattress sutures using non-absorbable monofilament.
Postoperative Care Protocol
- Weeks 0-2: The patient is placed in a short below-knee cast boot and remains strictly non-weight bearing on crutches. Sutures are removed at the 2-week mark.
- Weeks 2-4: Weight bearing is initiated progressively. Patients are strongly advised to utilize a custom or prefabricated foot orthosis with arch support during this transition to protect the midfoot.
- Week 4 and Beyond: Formal physical therapy commences, focusing on aggressive calf stretching, deep tissue massage, ultrasound therapy, and gradual intrinsic foot strengthening.
- Return to Sport: Running and high-impact activities may be resumed only when the patient can tolerate 30 to 40 minutes of continuous, brisk walking without experiencing daily symptoms or post-activity exacerbation.
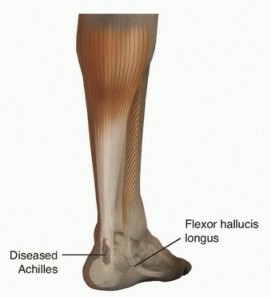
DISORDERS OF THE ACHILLES TENDON
Few conditions in orthopedic surgery are as notoriously frustrating to treat—both conservatively and surgically—as disorders of the Achilles tendon. Achieving a successful clinical outcome demands an extraordinary degree of patience, strict adherence to rehabilitation protocols, and diligence from both the surgeon and the patient.
Anatomy and Biomechanics
The Achilles tendon is the largest, thickest, and most powerful tendon in the human body. It is formed by the confluence of fibers from two distinct muscle units:
1. The Gastrocnemius Muscle: A biarticular muscle originating above the knee joint from the posterior aspect of the medial and lateral femoral condyles. It is most biomechanically effective in plantar flexing the ankle when the knee is fully extended.
2. The Soleus Muscle: A uniarticular muscle originating from the upper posterior tibia, fibula, and interosseous membrane. It is the primary plantar flexor when the knee is flexed.
As these fibers course distally through the superficial posterior compartment of the calf, they undergo a complex 90-degree lateral rotation before inserting into the calcaneal tuberosity. Consequently, the gastrocnemius fibers insert laterally, while the soleus fibers insert medially. This spiral configuration provides immense elastic energy storage during the gait cycle but also creates complex shear forces within the tendon substance.
Vascularity and Pathogenesis
The Achilles tendon lacks a true synovial sheath; instead, it is enveloped by a paratenon that supplies its superficial vascularity. Blood supply is derived from three main sources:
1. Muscular arterial branches proximally (at the musculotendinous junction).
2. Small interosseous vessels distally (at the calcaneal insertion).
3. The paratenon network along the length of the tendon.
Clinical Pearl: There is a well-documented "watershed" zone of relative avascularity located 2 to 6 cm proximal to the calcaneal insertion. While this marginal blood supply is sufficient for normal daily activities, excessive mechanical loading or repetitive microtrauma outpaces the tendon's healing capacity. This leads to mucoid degeneration, fibrosis, and tendinosis, severely prolonging tissue recovery.
Patient Demographics and Comorbidities
Chronic Achilles tendinopathy is rarely an isolated mechanical phenomenon; it is heavily influenced by systemic health. Holmes and Lin demonstrated that 98% of patients presenting with chronic Achilles tendinopathy possessed significant medical comorbidities, including:
* Hypertension
* Diabetes Mellitus
* Obesity
* Prior corticosteroid exposure
* Estrogen therapy
These systemic conditions induce microvascular disease, further diminishing the already tenuous blood supply to the watershed area and drastically reducing the tendon's intrinsic healing potential.
Differential Diagnosis
A comprehensive clinical evaluation must rule out other pathologies that mimic Achilles tendon disorders:
* Posterior tibial tendinitis or dysfunction
* Flexor hallucis longus (FHL) tendinitis (common in dancers)
* Peroneal tendinopathy
* Posterior ankle impingement syndrome (symptomatic os trigonum or enlarged trigonal process)
* Posterior subtalar or tibiotalar arthritis
* L5/S1 Radiculopathy (Sciatica)
* Exertional compartment syndrome of the deep posterior calf
* Tarsal tunnel syndrome
* Systemic arthritides: Seropositive (Rheumatoid arthritis, SLE) and Seronegative spondyloarthropathies (Reiter syndrome, Ankylosing spondylitis, Psoriatic arthritis).
INSERTIONAL ACHILLES TENDINITIS
In the classification of chronic Achilles tendon disorders, it is imperative to distinguish between noninsertional (watershed area) and insertional pathologies, as their surgical management differs entirely.
Pathoanatomy
Insertional Achilles tendinitis is a complex triad of pathologies occurring at the tendon-bone interface:
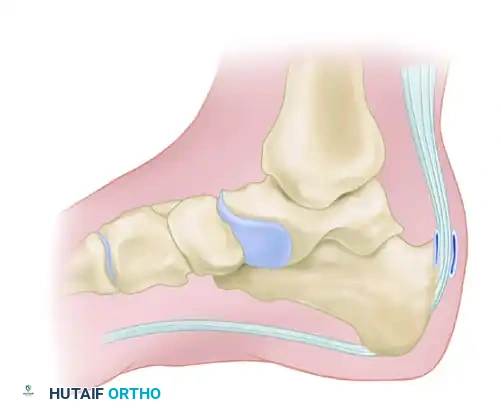
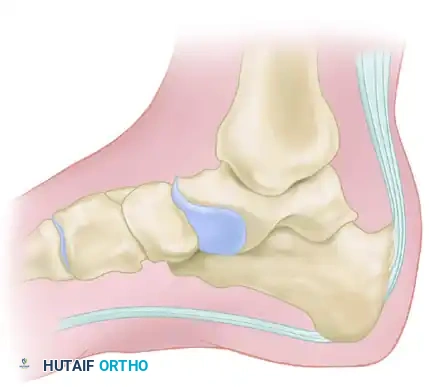
1. Haglund Deformity ("Pump Bump"): A prominent exostosis on the posterosuperior aspect of the calcaneal tuberosity.
2. Retrocalcaneal Bursitis: Inflammation of the bursa that normally acts as a lubricating cushion between the anterior aspect of the Achilles tendon and the posterosuperior calcaneus.
3. Insertional Tendinosis: Intratendinous degenerative tearing, often accompanied by dystrophic calcification or frank ossification within the distal tendon fibers.


Clinical Evaluation
Patients rarely report an acute traumatic event. The classic presentation is a slow, insidious onset of pain and swelling directly at the tendon insertion.
* Symptoms: Progressive inability to wear closed-back shoes due to direct mechanical pressure. Patients frequently report severe "start-up" pain after periods of rest, particularly when taking their first steps in the morning.
* Physical Examination: Direct palpation elicits exquisite tenderness over the retrocalcaneal bursa (anterior to the tendon) or centrally over the tendon insertion. A visible and palpable bony prominence is usually present. In advanced cases, the tendon itself becomes boggy, thickened, and nodular.
* Biomechanical Assessment: Examination almost universally reveals a significant equinus contracture of the gastrocsoleus complex, which is exacerbated when the knee is fully extended (Silfverskiöld test).

Radiographic Evaluation
Standard weight-bearing radiographs of the foot and ankle are mandatory. A standing lateral view of the heel is particularly useful for evaluating:
* The presence and size of a Haglund deformity (posterosuperior calcaneal prominence).
* Intratendinous calcific spurs extending proximally from the insertion.
* Chauveaux-Liet angle or parallel pitch lines to quantify the deformity.

Advanced imaging via Magnetic Resonance Imaging (MRI) is highly valuable for surgical planning. Nicholson et al. demonstrated that MRI findings strongly predict the likelihood of conservative treatment failure. In their review of 70 patients, those exhibiting tenderness at the insertion without superficial inflammation, but who demonstrated confluent areas of intrasubstance signal changes on MRI (Types II and III), were highly unlikely to respond to nonoperative modalities and ultimately required surgical debridement.
Evidence-Based Treatment Strategies
Conservative Management
Prolonged nonoperative treatment (minimum of 3 to 6 months) is the first line of defense.
* Mechanical Unloading: A 1- to 2-cm heel lift placed bilaterally in the shoes decreases tension on the insertion.
* Shoe Modification: Open-backed shoes or protective silicone sleeves alleviate direct pressure on the Haglund prominence.
* Physical Therapy: Eccentric loading exercises (though less tolerated in insertional vs. noninsertional tendinopathy) and aggressive calf stretching.
* Immobilization: In cases of acute, severe inflammatory flares, a short-leg cast or controlled ankle motion (CAM) boot for 4 to 6 weeks may be required.
* Injections: Corticosteroid injections are generally contraindicated within the tendon substance due to the high risk of iatrogenic rupture. However, a highly judicious, ultrasound-guided injection strictly isolated to the retrocalcaneal bursa may provide relief in refractory bursitis.
* Extracorporeal Shock Wave Therapy (ESWT): High-energy ESWT has shown promise in stimulating neovascularization and breaking up calcifications, though literature consensus remains mixed regarding long-term efficacy.
Surgical Principles
When conservative measures fail, surgical intervention involves a central tendon-splitting approach, excision of the retrocalcaneal bursa, resection of the Haglund deformity, and meticulous debridement of all degenerative tendon tissue and calcifications.
Surgical Warning: A critical intraoperative dilemma is determining how much degenerative tendon can be safely resected before the structural integrity of the Achilles is compromised, risking catastrophic postoperative rupture.
Anatomical studies evaluating the Achilles insertion footprint provide vital guidance. The average dimensions of the insertion are:
* Height: 19.8 mm
* Proximal Width: 23.8 mm
* Distal Width: 32.1 mm
Biomechanical data confirms that surgeons can safely detach and resect up to 50% of the tendon insertion (from superior to inferior) to access the Haglund prominence and remove diseased tissue without requiring formal tendon augmentation (e.g., FHL transfer). If more than 50% of the tendon requires detachment or is lost to debridement, suture anchor repair of the remaining tendon to the calcaneal footprint, often augmented with a flexor hallucis longus (FHL) tendon transfer, is strictly indicated to restore plantar flexion power and prevent avulsion.
📚 Medical References
- yields worse results in nonathletic patients, Chin J Sports Med 16:123, 2006.
- Mann RA, ed: Surgery of the foot, 5th ed, St Louis, 1986, Mosby. Mann RA: Flatfoot in adults. In Mann RA, Coughlin MJ, eds: Surgery of the foot and ankle, vol 1, St Louis, 1993, Mosby. Mann RA: Posterior tibial tendon dysfunction. Treatment by fl exor digitorum longus transfer, Foot Ankle Clin 6:77, 2001.
- Mann RA, Beaman DN, Horton GA: Isolated subtalar arthrodesis, Foot Ankle Int 19:511, 1998.
- Mann RA, Specht LH: Posterior tibial tendon ruptures: analysis of eight cases, Foot Ankle 2:350, 1982 (abstract). Mann R, Thompson FM: Rupture of the posterior tibial tendon causing fl at foot, J Bone Joint Surg 67A:556, 1985.
- Markarian GG, Kelikian AS, Brage M, et al: Anterior tibialis tendon ruptures: an outcome analysis of operative versus nonoperative treatment, Foot Ankle Int 19:792, 1998.
- Mason RB, Henderson JP: Traumatic peroneal tendon instability, Am J Sports Med 24:652, 1996.
- McConkey JP, Favero KJ: Subluxation of the peroneal tendons within the peroneal tendon sheath: a case report, Am J Sports Med 15:511, 1987.
- McCormack AP, Varner KE, Marymont JV: Surgical treatment for posterior tibial tendonitis in young competitive athletes, Foot Ankle Int 24:535, 2003.
- Mengiardi B, Pfi rrmann CW, Vienne P, et al:
You Might Also Like