Surgical Management of Haglund Deformity, Retrocalcaneal Bursitis, and Achilles Tendinosis

Key Takeaway
Haglund deformity, often presenting with retrocalcaneal bursitis and insertional Achilles tendinosis, requires meticulous surgical intervention when conservative measures fail. Operative management typically involves a calcaneal osteotomy to resect the posterosuperior prominence. In cases of severe chronic tendinosis with significant tendon compromise, an adjunctive flexor hallucis longus (FHL) transfer is indicated to restore plantar flexion strength and provide vascularized tissue to the deficient Achilles insertion.
Comprehensive Introduction and Patho-Epidemiology
Haglund deformity, colloquially referred to within the clinical lexicon as a "pump bump," represents a prominent posterosuperior calcaneal tuberosity that precipitates mechanical impingement against the anterior aspect of the Achilles tendon. This osseous prominence, when combined with the repetitive ankle dorsiflexion inherent in the human gait cycle, creates a complex pathologic triad universally recognized as Haglund syndrome. This triad consists of insertional Achilles tendinopathy, retrocalcaneal bursitis, and the physical manifestations of the Haglund deformity itself. The interplay of these three elements generates a self-perpetuating cycle of inflammation, structural degeneration, and profound clinical morbidity that can debilitate both high-level athletes and sedentary individuals alike.
The pathophysiology of this condition is rooted in chronic mechanical attrition. The retrocalcaneal bursa, strategically situated between the anterior aspect of the Achilles tendon and the superior bare area of the posterosuperior calcaneus, serves as a vital friction-reducing structure under normal physiological conditions. However, in the presence of an enlarged calcaneal prominence, this bursa becomes the focal point of intense mechanical shear forces. Consequently, it undergoes severe inflammatory changes, becoming hyperemic, hypertrophic, and fibrotic. Over time, this localized inflammatory milieu, combined with direct mechanical impingement, leads to profound structural compromise of the adjacent Achilles tendon. Pathoanatomical evaluation of the tendon frequently reveals extensive intrasubstance degeneration, characterized by mucoid degeneration, disruption of the highly ordered type I collagen architecture, and the insidious formation of intratendinous calcifications or macroscopic osteophytes at the tendinous insertion site.
Epidemiologically, Haglund syndrome exhibits a bimodal distribution, frequently afflicting young to middle-aged active individuals, particularly endurance runners, as well as older patients with cumulative degenerative changes. There is a noted predilection for female patients, largely attributed to the prolonged utilization of rigid-heeled, restrictive footwear (such as high heels or dress shoes), which directly compresses the superficial retro-Achilles bursa and exacerbates the underlying impingement. Patients typically present with insidious, progressive posterior heel pain that is markedly exacerbated by walking up inclines, running, or donning rigid-heeled footwear. Clinical examination invariably reveals a palpable, exquisitely tender prominence at the posterolateral aspect of the heel, frequently accompanied by localized erythema, soft tissue swelling, and palpable crepitus during active ankle range of motion.
The natural history of untreated Haglund syndrome is progressive functional decline. As the intrasubstance degeneration of the Achilles tendon advances, the tensile strength of the tendon is critically compromised, exposing the patient to an elevated risk of spontaneous partial or complete tendon rupture. Furthermore, the chronic pain alters the patient's biomechanical gait mechanics, often leading to secondary compensatory pathologies in the ipsilateral knee, hip, or contralateral lower extremity. Therefore, a profound understanding of the underlying patho-epidemiology is an absolute prerequisite for the orthopedic surgeon tasked with formulating an effective, long-term management strategy.
Detailed Surgical Anatomy and Biomechanics
A masterful command of the surgical anatomy and biomechanics of the posterior hindfoot is paramount to the successful surgical execution of a calcaneal osteotomy and Achilles tendon debridement. The footprint of the Achilles tendon is a complex, three-dimensional structure that dictates the limits of safe osseous resection. The tendon inserts into the middle third of the posterior calcaneal tuberosity. This insertion is distinctly crescent-shaped, being significantly wider distally and medially, and tapering proximally and laterally. Crucially, the superior third of the posterior calcaneus is entirely devoid of tendinous attachments; this "bare area" is covered by the retrocalcaneal bursa and is the primary anatomical site of the Haglund prominence.
During a calcaneal osteotomy, the surgeon's primary anatomical objective is to resect this superior bare area without compromising the structural integrity of the distal Achilles insertion. However, because the Achilles tendon possesses an extensive insertion that wraps around the posterior and extends into the plantar aspect of the tuberosity, achieving an adequate bony resection frequently necessitates the deliberate elevation of a 1- to 2-cm long portion of the tendon from its proximal footprint. The vascular supply to the Achilles tendon is notoriously tenuous, particularly in the watershed area located 2 to 6 cm proximal to its insertion. However, insertional tendinopathy associated with Haglund deformity involves the distal-most aspect of the tendon, which receives its vascular supply primarily from the underlying periosteum and the surrounding paratenon. Preservation of the paratenon during surgical exposure is therefore a critical step in optimizing postoperative tissue healing.
Biomechanically, the Achilles tendon functions as the primary dynamic stabilizer and plantar flexor of the ankle joint, capable of withstanding forces up to ten times the patient's body weight during explosive athletic activities. The posterosuperior prominence of the calcaneus acts as a fulcrum during extreme dorsiflexion, increasing the mechanical advantage of the gastroc-soleus complex but simultaneously concentrating immense compressive and shear forces on the anterior fibers of the tendon. The surgical resection of the Haglund deformity fundamentally alters this biomechanical relationship by decompressing the retrocalcaneal space, thereby eliminating the pathological fulcrum and restoring linear tension to the tendon fibers.
In cases requiring augmentation due to severe tendinous degeneration, the Flexor Hallucis Longus (FHL) tendon serves as the premier anatomical and biomechanical substitute. The FHL is an in-phase synergist to the gastroc-soleus complex, firing simultaneously during the push-off phase of the gait cycle. Anatomically, the FHL muscle belly is the most posterior and lateral structure within the deep posterior compartment of the leg, extending distally to the level of the tibiotalar joint. Its robust, low-lying, highly vascularized muscle belly provides a critical biological advantage when transferred, as it introduces a rich, neo-vascular blood supply directly into the relatively avascular, degenerative zone of the reconstructed Achilles tendon, thereby profoundly enhancing the biological healing environment.
Exhaustive Indications and Contraindications
Surgical intervention for Haglund syndrome and insertional Achilles tendinopathy is strictly reserved for patients who have demonstrated recalcitrant symptoms despite a rigorous, exhaustively documented trial of conservative management. The decision to proceed with operative intervention must be highly individualized, taking into account the patient's physiological age, functional demands, medical comorbidities, and inherent expectations regarding postoperative recovery.
Nonoperative modalities must be aggressively pursued for a minimum of 6 to 12 months prior to considering surgical intervention. This conservative regimen should encompass comprehensive activity modification, the judicious use of nonsteroidal anti-inflammatory drugs (NSAIDs), the implementation of customized heel lifts or orthotics to functionally plantarflex the ankle and relieve tension, and the utilization of open-backed footwear to eliminate direct posterior compression. Physical therapy is the cornerstone of conservative management, with a specific, heavily supervised focus on eccentric stretching and strengthening protocols of the gastroc-soleus complex. In highly recalcitrant cases, temporary immobilization in a controlled ankle motion (CAM) boot may be utilized to break the inflammatory cycle. It is imperative to note that corticosteroid injections within or adjacent to the retrocalcaneal bursa are highly controversial, universally discouraged by major orthopedic societies, and represent a profound medicolegal risk due to the extensively documented, catastrophic complication of iatrogenic Achilles tendon rupture.
When conservative measures unequivocally fail, surgical resection of the Haglund prominence (via calcaneal osteotomy or exostectomy) combined with aggressive debridement of the retrocalcaneal bursa and the diseased, necrotic portions of the Achilles tendon is indicated.
Surgical Warning: Managing Patient Expectations
Preoperative counseling is arguably the most critical, yet frequently underappreciated, step in the management of Haglund deformity. The literature consistently demonstrates a discrepancy between surgical success and early patient satisfaction. Brunner et al. reported that a significant subset of patients (16.6%) who underwent calcaneal osteotomy were dissatisfied with their outcomes in the early postoperative period, primarily due to the unexpectedly prolonged and arduous recovery trajectory. Surgeons must explicitly, unequivocally warn patients—particularly young, active females seeking to return to wearing stylish, rigid-heeled shoes—that the recovery period is exceptionally lengthy, typically ranging between 6 months and 2 years. Patients must be meticulously informed that it may require 3 to 6 months before they can comfortably transition into standard footwear, and there exists no absolute guarantee that they will ever be able to wear rigid, stylish shoes without experiencing some degree of residual discomfort or swelling.
| Category | Specific Criteria | Clinical Rationale / Considerations |
|---|---|---|
| Absolute Indications | Failure of >6 months of targeted conservative therapy | Ensures natural healing potential is exhausted before altering biomechanics. |
| MRI-confirmed severe intrasubstance tearing/necrosis | Indicates irreversible structural damage requiring mechanical debridement. | |
| Impending or acute-on-chronic tendon rupture | Requires immediate structural repair and potential FHL augmentation. | |
| Relative Indications | Profound functional limitation in high-demand athletes | May accelerate surgical timeline to preserve athletic career viability. |
| Intractable pain strictly localized to the retrocalcaneal bursa | Exostectomy alone may suffice if tendon integrity is completely preserved. | |
| Absolute Contraindications | Active systemic or localized hindfoot infection | High risk of deep space infection and catastrophic osteomyelitis. |
| Severe Peripheral Arterial Disease (PAD) / Ischemia | Posterior heel skin envelope will predictably fail, leading to amputation. | |
| Medical non-compliance or inability to adhere to NWB protocols | Early weight-bearing will result in catastrophic failure of the tendon repair. | |
| Relative Contraindications | Poorly controlled Diabetes Mellitus (HbA1c > 8.0%) | Significantly elevated risk of wound dehiscence and delayed union. |
| Active smoking / Nicotine dependence | Microvascular compromise heavily impairs the tenuous posterior skin healing. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock of a successful surgical outcome in the management of Haglund deformity. This phase requires meticulous radiographic analysis to quantify the extent of the osseous deformity and advanced imaging to evaluate the structural integrity of the Achilles tendon. Weight-bearing orthogonal radiographs of the foot and ankle are mandatory. The lateral radiograph is the primary workhorse for templating the calcaneal osteotomy. The surgeon must evaluate several radiographic parameters, including the Fowler-Philip angle, the parallel pitch lines, and the Chauveaux-Liet angle. While these angles have variable sensitivity and specificity, they collectively provide a critical geometric framework for understanding the magnitude of the posterosuperior prominence relative to the longitudinal axis of the calcaneus and the plantar surface of the foot.
Magnetic Resonance Imaging (MRI) without contrast is considered the gold standard for preoperative soft tissue evaluation. The MRI allows the surgeon to meticulously map the extent of the retrocalcaneal bursitis, quantify the volume of intrasubstance mucoid degeneration within the Achilles tendon, and identify the presence of intratendinous osteophytes. Crucially, the MRI dictates the surgical strategy: if the axial and sagittal sequences demonstrate that greater than 50% of the cross-sectional area of the Achilles tendon is necrotic or structurally compromised, the surgeon must preoperatively plan, template, and consent the patient for an adjunctive Flexor Hallucis Longus (FHL) tendon transfer.
Anesthesia and Patient Positioning
The procedure is typically performed under general anesthesia, although regional anesthesia (such as a spinal block or a continuous popliteal sciatic nerve block) is an excellent alternative that provides profound postoperative analgesia and reduces the requirement for systemic opioids.
The patient is meticulously positioned in the prone position on a radiolucent operating table. Proper positioning is critical to avoid peripheral nerve compression; all bony prominences, including the anterior superior iliac spines, patellae, and contralateral foot, must be heavily padded. The operative lower extremity is prepped and draped in a standard sterile fashion, allowing for visualization and manipulation of the foot up to the proximal third of the leg. A well-padded pneumatic tourniquet is applied to the proximal thigh, rather than the calf, to ensure an entirely bloodless surgical field without tethering the proximal excursion of the gastroc-soleus complex or the FHL muscle belly during tensioning. Fluoroscopy should be positioned on the contralateral side of the table, ensuring orthogonal lateral views of the calcaneus can be obtained effortlessly throughout the procedure to confirm the trajectory and depth of the osseous resection.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution demands meticulous soft tissue handling, precise osseous resection, and robust biomechanical reconstruction. The primary surgical objective is to decompress the retrocalcaneal space by excising the inflamed bursa, resecting the posterosuperior calcaneal prominence, and aggressively debriding any calcified, mucoid, or necrotic portions of the Achilles tendon.
Incision and Superficial Dissection
Make a longitudinal lateral incision approximately 1 cm lateral to the lateral border of the Achilles tendon. The incision should extend distally from 3 to 4 cm proximal to the superior tuberosity of the calcaneus, down to 2 to 3 cm distal to the superior tuberosity. Deepen the incision through the subcutaneous tissues with extreme caution. Take meticulous care to identify, mobilize, and protect the sural nerve. The sural nerve crosses the lateral border of the Achilles tendon approximately 10 cm proximal to its insertion and courses distally along the lateral hindfoot; it is highly vulnerable to iatrogenic transection or traction neuropraxia during this approach.
Deep Dissection and Exposure
Plantar flex the ankle joint to relieve tension on the Achilles tendon. By a combination of sharp and blunt dissection, identify the lateral border of the Achilles tendon and enter the retrocalcaneal space. Excise the hypertrophic retrocalcaneal bursa entirely to expose the underlying superior bare area of the calcaneus. Place a right-angle or Hohmann retractor between the anterior aspect of the Achilles tendon and the posterior/superior borders of the calcaneal tuberosity. With the foot held in plantar flexion, this maneuver usually affords sufficient exposure to access the superior border of the calcaneal tuberosity. While the goal is to leave the Achilles insertion undisturbed, the extensive footprint often dictates that raising a 1- to 2-cm long portion of the tendon from the posterior and plantar aspect of the tuberosity is necessary to achieve an adequate, unimpeded bony resection.
Resection of the Haglund Prominence and Tendon Debridement
Remove the superior aspect of the tuberosity (the Haglund lesion) using a microsagittal saw or a sharp, wide osteotome. Placing several drill holes along the proposed osteotomy site from lateral to medial significantly facilitates this resection and prevents the catastrophic, inadvertent propagation of the osteotomy into the posterior facet of the subtalar joint. The saw cut should be angled from posterosuperior to anteroinferior, effectively removing the entire prominence that impinges on the tendon during dorsiflexion. Following the osteotomy, utilize a rasp to meticulously smooth all sharp osseous edges.
Inspect the anterior aspect of the Achilles tendon. If an area of intratendinous ossification or severe tendinosis remains, split the Achilles tendon longitudinally in a coronal plane. Elevate the anterior third or half of the tendon distally to free up enough tissue to completely excise the calcified and necrotic tendon matrix until robust, healthy, parallel collagen fibers are visualized.
Adjunctive Flexor Hallucis Longus (FHL) Transfer
In cases of chronic, severe insertional or noninsertional Achilles tendinosis associated with Haglund deformity, extensive debridement may leave the Achilles tendon critically deficient. If more than 50% of the tendon insertion is resected, or if the remaining tendon is severely degenerated, augmentation is absolutely required to prevent postoperative rupture and restore plantar flexion power.
Step 1: Exposure of the Defect
Following the resection of the Haglund prominence and aggressive debridement of the diseased Achilles tendon, assess the remaining defect. In chronic cases, a massive void is often present, necessitating structural augmentation.
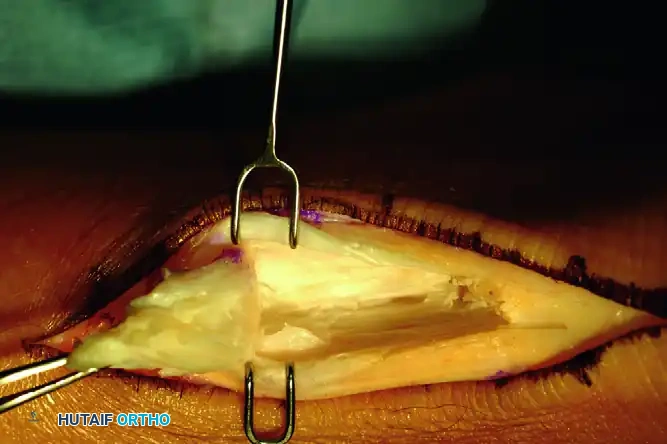
FIGURE A: Exposure of the involved portion of the tendon, demonstrating the extensive defect following debridement of chronic tendinosis.
Step 2: Identification and Harvest of the FHL
The FHL can be harvested through the same posterior incision. Deepen the dissection medially, anterior to the Achilles tendon and posterior to the deep posterior compartment fascia. Identify the FHL muscle belly, which is the most posterior and lateral structure in the deep posterior compartment. Trace the FHL tendon distally as it enters the fibro-osseous tunnel beneath the sustentaculum tali. Harvest the tendon as distally as possible. While a double-incision technique can yield a longer graft, a single posterior incision usually provides sufficient length to bridge the Achilles defect and anchor into the calcaneus.

FIGURE B: Harvest and mobilization of the flexor hallucis longus (FHL) tendon. Note the robust, low-lying muscle belly.
Step 3: Fixation and Muscle Belly Interposition
Drill a bone tunnel or utilize a biotenodesis screw system in the superior aspect of the calcaneus, positioned just anterior to the remaining Achilles footprint. Tension the harvested FHL tendon into the calcaneal tunnel with the ankle held rigidly in 15 to 20 degrees of plantar flexion to match the resting tension of the native Achilles complex. Secure the fixation. Subsequently, suture the robust FHL muscle belly directly into the Achilles tendon defect. This step is biologically critical, as the highly vascular muscle belly provides a rich blood supply to the avascular zone of the Achilles, significantly enhancing the biologic healing potential of the construct.
FIGURE C: The flexor hallucis longus muscle belly is meticulously sutured into the Achilles tendon defect, providing both biomechanical augmentation and vascular enhancement.
Wound Closure
Meticulous hemostasis is absolutely mandatory upon tourniquet deflation to prevent postoperative hematoma formation, which can severely compromise wound healing in this high-risk anatomical area. Copiously lavage the wound with sterile saline to remove all microscopic bone debris generated from the osteotomy. If the Achilles tendon was split or partially detached, repair it using heavy, nonabsorbable polyblend sutures (e.g., #2 FiberWire) utilizing a Krackow or similar locking stitch configuration. Utilize suture anchors if robust reattachment to the calcaneus is required. Close the paratenon meticulously if viable, followed by the subcutaneous tissues and the skin in a layered, tension-free fashion. A closed-suction drain may be placed deep to the fascial layer at the surgeon's discretion to evacuate residual hematoma.
Complications, Incidence Rates, and Salvage Management
Surgical management of Haglund deformity and Achilles tendinosis is fraught with potential complications, largely driven by the tenuous vascularity of the posterior heel skin envelope and the high mechanical demands placed on the reconstructive construct. The surgeon must possess a deep understanding of these pitfalls and be prepared to execute complex salvage procedures when required.
Wound dehiscence and superficial or deep infections represent the most frequent and feared complications. The posterior heel relies on a fragile subdermal vascular plexus. Excessive intraoperative retraction, overly tight skin closure, or premature postoperative mobilization can rapidly induce skin necrosis, wound breakdown, and subsequent deep infection. Meticulous soft tissue handling, full-thickness flaps, and strict postoperative elevation are non-negotiable tenets of prevention. Inadequate bone resection is another common pitfall; failure to aggressively remove the posterosuperior prominence will invariably result in persistent mechanical impingement and recurrent clinical symptoms, necessitating revision osteotomy.
Achilles tendon avulsion or catastrophic postoperative rupture is a devastating complication. This typically occurs secondary to over-resection of the calcaneus that inadvertently violates the distal Achilles footprint, or from a failure to augment a severely degenerated tendon (where >50% of the cross-sectional area was debrided). Surgeons must maintain a very low threshold to perform an FHL transfer if the macroscopic integrity of the tendon is remotely questionable. Furthermore, iatrogenic injury to the sural nerve during the lateral surgical approach can result in painful, debilitating neuromas and permanent lateral foot numbness.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage Management / Treatment Strategy |
|---|---|---|---|
| Wound Dehiscence / Necrosis | 5% - 15% | Tenuous vascularity, excessive retraction, smoking, diabetes, early ROM. | Local wound care, Vacuum-Assisted Closure (VAC). Severe cases require sural artery fasciocutaneous flap coverage. |
| Deep Space Infection | 1% - 3% | Progression of superficial dehiscence, hematoma formation, immunocompromise. | Urgent aggressive surgical I&D, hardware removal if uninfected union is not achieved, targeted IV antibiotics, VAC therapy. |
| Achilles Tendon Rupture | 2% - 5% | Over-resection of footprint, failure to augment >50% defect, non-compliance with NWB. | Revision surgery with V-Y advancement flap, FHL transfer, or allograft reconstruction (e.g., Achilles or semitendinosus). |
| Recurrent Impingement | 5% - 10% | Inadequate resection angle, failure to remove medial/lateral flares of the tuberosity. | Revision calcaneal osteotomy ensuring resection is parallel to the posterior facet of the subtalar joint. |
| Sural Nerve Neuroma | 3% - 7% | Iatrogenic transection, aggressive retraction, entrapment in scar tissue. | Initial trial of gabapentinoids and targeted injections. Refractory cases require surgical neuroma excision and proximal burying into muscle. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol following Haglund resection and Achilles reconstruction is a delicate, meticulously phased balancing act. The primary directive is to protect the structural integrity of the osseous and tendinous repairs while simultaneously preventing debilitating arthrofibrosis and soft tissue contractures. Patient compliance with this protracted protocol is the ultimate determinant of surgical success.
Phase 1: Maximum Protection and Immobilization (Weeks 0–3)
Immediately postoperatively in the operating theater, the patient is placed into a well-padded, short-leg, non–weight-bearing (NWB) plaster or fiberglass cast. The ankle must be strictly immobilized in approximately 15 to 20 degrees of plantar flexion. This specific positioning is mechanically critical; it minimizes tension across the Achilles repair site, protects the FHL transfer from premature loading, and prevents tension on the posterior skin incision. During this phase, strict, continuous elevation of the operative extremity above the level of the heart is mandatory to manage postoperative edema and protect the tenuous microvascular perfusion of the posterior skin envelope. Deep vein thrombosis (DVT) prophylaxis should be administered according to the patient's individualized risk stratification.
Phase 2: Transition and Early Range of Motion (Weeks 3–6)
At the 3-week postoperative mark, the cast is bivalved, and the skin sutures are meticulously removed. While sutures may be removed earlier if clinically indicated by wound assessment, the NWB status must remain absolute for the full 3 weeks. Following suture removal, the patient is transitioned into a removable controlled ankle motion (CAM) weight-bearing cast boot. This boot must be fitted with customized heel wedges (typically three 1-cm wedges) to maintain the ankle in slight plantar flexion. The patient is instructed to initiate active plantar flexion and gentle active dorsiflexion exercises strictly to the neutral position. Passive dorsiflexion stretching is absolutely prohibited at this stage, as it places catastrophic tension on the healing tendon insertion. Weight-bearing is gradually progressed in the CAM boot, utilizing crutches, as tolerated by the patient.
Phase 3: Strengthening and Normalization of Gait (Weeks 6–12)
During this critical transition phase, the primary goal is the normalization of the gait cycle and the initiation of tendon loading. The heel wedges are gradually removed from the CAM boot over a period of 2 to 3 weeks (typically one wedge every 5 to 7 days) to slowly, progressively stretch the Achilles-gastrocsoleus complex. By week 8 to 10, the patient is typically transitioned out of the CAM boot and into regular, supportive athletic footwear equipped with a slight, temporary heel lift. Formal, supervised physical therapy is initiated. The protocol focuses initially on isometric strengthening of the plantar flexors, progressing methodically to concentric loading, and eventually, late in the phase, to strictly controlled eccentric loading of the gastroc-soleus complex. Modalities such as cross-friction massage and ultrasound may be utilized to manage scar tissue formation.
Phase 4: Return to Activity and Sport-Specific Training (Months 3–6+)
This final phase focuses on dynamic stabilization, proprioceptive neuromuscular training, and the gradual reintroduction of sport-specific activities. Plyometric exercises, agility drills, and progressive running programs are initiated only when the patient demonstrates symmetrical, pain-free single-leg heel raises. As emphatically emphasized during the preoperative counseling phase, patients must be continuously reminded that complete resolution of microscopic soft tissue swelling and the ability to wear rigid, stylish, or restrictive footwear comfortably may take up to 6 to 12 months. Furthermore, maximal medical improvement (MMI) and the complete remodeling of the tendon construct may not be reached until 1 to 2 years postoperatively.
Summary of Landmark Literature and Clinical Guidelines
The surgical management of Haglund deformity and insertional Achilles tendinopathy is heavily guided by a robust body of orthopedic literature and evolving clinical guidelines. A synthesis of landmark studies provides the evidence-based foundation for the surgical techniques and protocols detailed in this chapter.
The foundational understanding of the clinical outcomes following calcaneal osteotomy is heavily informed by the work of Brunner et al. Their landmark retrospective analysis highlighted the critical disconnect between objective surgical success and subjective early patient satisfaction. By reporting that nearly 17% of patients were dissatisfied primarily due to the prolonged recovery timeline, this study established the absolute necessity of aggressive, realistic preoperative counseling regarding the 6- to 24-month recovery trajectory. This finding has been universally adopted into modern clinical guidelines as a mandatory component of the informed consent process.
The utilization of the Flexor Hallucis Longus (FHL) tendon for the augmentation of massive Achilles defects was popularized and validated by the seminal works of Wapner and later, Wilcox et al. These studies biomechanically and clinically demonstrated that the FHL, due to its in-phase synergistic firing pattern and its robust, highly vascularized muscle belly, provides superior clinical outcomes compared to other transfer options (such as the peroneus brevis) when greater than 50% of the Achilles tendon requires debridement. The literature conclusively supports that interposing the FHL muscle belly directly into the avascular defect significantly reduces the incidence of postoperative re-rupture and accelerates biologic incorporation.
Furthermore, biomechanical studies focusing on the geometry of the calcaneal osteotomy have fundamentally shaped modern surgical technique. Research evaluating the Fowler-Philip and Chauveaux-Liet angles has demonstrated that while preoperative templating is useful, the intraoperative execution of the osteotomy must prioritize a resection plane that is perfectly parallel to the posterior facet of the subtalar joint. Failure to achieve this specific trajectory, as documented in multiple revision cohorts, is the primary driver of recurrent mechanical impingement and surgical failure. Collectively, these landmark studies and established guidelines dictate a surgical approach that is aggressive in its osseous resection, meticulous in its soft tissue handling, and biologically respectful in its reconstructive augmentation.
This academic synthesis is based on established protocols from Hutaiforth
---
