Musculoskeletal Tuberculosis: Diagnosis & Surgical Management
Key Takeaway
Musculoskeletal tuberculosis represents a profound diagnostic and therapeutic challenge, affecting 1% to 8% of patients with extrapulmonary disease. This comprehensive guide details the pathophysiology, clinical presentation, and evidence-based management of osseous tuberculosis. Emphasizing a multidisciplinary approach, it covers advanced imaging, targeted chemoprophylaxis, and joint-specific surgical interventions—ranging from joint-preserving debridement to complex arthrodesis—essential for eradicating infection, preventing deformity, and restoring biomechanical function in affected patients.
Comprehensive Introduction and Patho-Epidemiology
Current estimates indicate that up to one-third of the global population has been exposed to or infected by tuberculosis (TB), an ancient disease that continues to exert a devastating toll on global public health. Despite the advent of modern multidrug chemotherapy and advanced surgical techniques, tuberculosis remains a leading cause of infectious mortality worldwide, secondary only to viral pandemics in recent epidemiological tracking. The highest incidence rates are heavily localized in Southeast Asia, the Indian subcontinent, and sub-Saharan Africa. However, in North America and Western Europe, infection rates witnessed a dramatic and alarming resurgence in the late 1980s and early 1990s. This epidemiological shift was driven largely by the human immunodeficiency virus (HIV) epidemic, rising iatrogenic immunosuppression (such as biologic therapies for rheumatological conditions), and increased global migration from highly endemic regions.
Populations at the highest risk for developing both primary and reactivated tuberculosis include individuals with acquired immunodeficiency syndrome (AIDS), chronic renal failure, severe malnutrition, substance abuse disorders, and those living in densely populated, impoverished, or incarcerated settings. From a demographic standpoint, foreign-born individuals account for over half of all recent cases diagnosed in the United States, with the highest risk of active disease manifesting within the first five years of immigration. Furthermore, the emergence of multidrug-resistant (MDR-TB) and extensively drug-resistant (XDR-TB) strains has severely complicated management paradigms, necessitating highly specialized, prolonged chemotherapeutic regimens and aggressive surgical interventions to prevent catastrophic musculoskeletal morbidity.
Tuberculosis is primarily transmitted via the inhalation of aerosolized Mycobacterium tuberculosis droplets. Following the primary pulmonary infection, which may remain asymptomatic or manifest as a mild respiratory illness, the bacilli can disseminate via lymphogenous or hematogenous routes to virtually any organ system. This dissemination often occurs before the host mounts a robust cell-mediated immune response. Extrapulmonary involvement occurs in approximately 14% to 20% of immunocompetent patients, but this figure rises precipitously in immunocompromised cohorts. Osseous disease manifests in 1% to 8% of all extrapulmonary cases.
Musculoskeletal tuberculosis most frequently targets the axial skeleton, with the spine (Pott disease) accounting for 30% to 50% of all osseous cases. In the appendicular skeleton, the disease demonstrates a profound predilection for major weight-bearing joints, particularly the hip and knee, followed by the foot, ankle, elbow, and hand. The hallmark of osseous tuberculosis is the formation of caseating granulomas containing multinucleated Langhans giant cells, surrounded by a halo of epithelioid macrophages and lymphocytes. Unlike pyogenic arthritis, which rapidly destroys articular cartilage via the release of potent proteolytic enzymes from polymorphonuclear leukocytes, tuberculous arthritis initially spares the cartilage. The infection typically begins in the highly vascularized metaphyseal or subchondral bone, leading to insidious trabecular necrosis, subchondral collapse, and the eventual mechanical detachment of the overlying, yet often biologically viable, articular cartilage.
Detailed Surgical Anatomy and Biomechanics
Understanding the distinct surgical anatomy and biomechanics of musculoskeletal tuberculosis is critical for both accurate diagnosis and the execution of complex reconstructive procedures. The localization of tuberculous lesions is heavily dictated by the vascular anatomy of the developing and mature skeleton. In pediatric patients, the metaphyseal blood vessels frequently penetrate the open physis, allowing the mycobacteria to cross directly into the epiphysis and subsequently invade the joint space. In adults, the infection typically seeds the subchondral bone via terminal arterial arcades. The resulting inflammatory hyperemia leads to severe juxta-articular osteoporosis, a key radiographic hallmark that severely compromises the biomechanical integrity of the bone and complicates surgical fixation.
In the hip joint, the disease frequently begins in the acetabular roof or the superior quadrant of the femoral head. As the caseating granulomas expand, they induce profound osteolysis. The biomechanical forces across the hip joint—specifically the superior and medial vectors generated by the abductor and iliopsoas musculature—exacerbate this bone loss, leading to the classic "wandering acetabulum." This phenomenon results in superior and medial migration of the femoral head, effectively destroying the normal center of rotation and leading to severe abductor weakness, limb length discrepancy, and a profoundly altered gait biomechanic. The capsular anatomy of the hip, which extends down to the intertrochanteric line anteriorly, means that any metaphyseal focus of infection within the femoral neck is inherently intra-articular, facilitating rapid joint contamination.
The knee, being the largest synovial joint in the body, offers a massive surface area for tuberculous synovitis. The disease often presents with a boggy, hypertrophic synovium that fills the suprapatellar pouch and the medial and lateral gutters. Biomechanically, the chronic effusion and pain lead to reflex spasm of the hamstring musculature, rapidly producing a severe flexion contracture. This contracture not only severely limits ambulation but also alters the contact mechanics of the tibiofemoral joint, accelerating posterior subluxation of the tibia and secondary degenerative changes. The cruciate ligaments and menisci are eventually encased in a thick, fibrinous exudate (pannus), leading to their enzymatic and mechanical degradation.
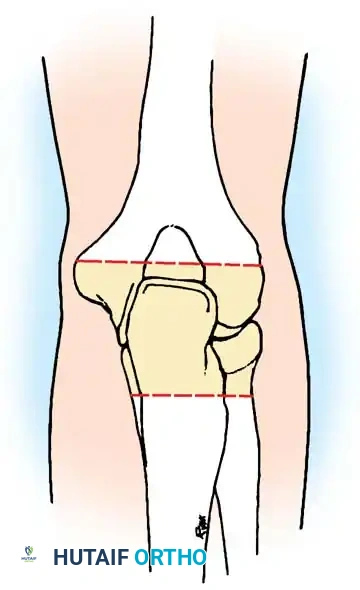
In the foot and ankle, the complex intertarsal articulations provide multiple interconnected synovial cavities through which the infection can rapidly spread. The talonavicular and subtalar joints are critical for hindfoot inversion and eversion; destruction of these joints by tuberculous osteomyelitis leads to a rigid, painful, and often severely deformed planovalgus or equinovarus foot. The calcaneus is frequently involved, presenting with large cystic, lytic lesions that compromise the structural integrity of the Achilles tendon insertion and the plantar fascia origin, fundamentally destroying the windlass mechanism of the foot.

In the upper extremity, the elbow and wrist are the primary targets. The elbow's complex hinge and pivot mechanics are easily disrupted by lytic destruction of the distal humerus or olecranon. The proximity of the ulnar nerve in the cubital tunnel makes it highly susceptible to compression from expanding cold abscesses or granulomatous tissue. In the wrist, the disease often begins as a tenosynovitis within the extensor or flexor retinaculum, mechanically tethering the tendons and leading to attritional ruptures before invading the radiocarpal and intercarpal joints.
Exhaustive Indications and Contraindications
The management of musculoskeletal tuberculosis demands a highly nuanced, multidisciplinary approach. While the cornerstone of treatment is prolonged multidrug antituberculous chemotherapy, surgical intervention is frequently required to address mechanical instability, severe deformity, and medically refractory disease. The decision to proceed with operative management must be carefully weighed against the patient's nutritional status, immune competence, and the local soft-tissue envelope.
| Parameter | Indications for Surgical Intervention | Contraindications for Surgical Intervention |
|---|---|---|
| Medical Response | Failure of clinical improvement after 3-5 months of compliant RIPE therapy; MDR-TB or XDR-TB strains requiring extensive debridement. | Excellent clinical and radiographic response to initial chemotherapy; non-compliance with medical therapy. |
| Neurological Status | Progressive neurological deficit (e.g., cauda equina syndrome, peripheral nerve compression from cold abscess). | Stable or rapidly improving neurological symptoms under medical management alone. |
| Structural Integrity | Impending or actual pathological fracture; severe joint destruction with subchondral collapse; spinal instability. | Early synovial stage disease with preserved articular cartilage and subchondral bone stock. |
| Soft Tissue & Abscess | Large, symptomatic cold abscesses causing mass effect; chronic draining sinus tracts with secondary pyogenic superinfection. | Small, asymptomatic cold abscesses that are resolving on serial imaging. |
| Deformity | Severe, fixed contractures preventing ambulation (e.g., severe knee flexion contracture, wandering acetabulum). | Mild, passively correctable deformities amenable to serial casting or orthotic management. |
| Systemic Factors | Medically optimized patient with isolated musculoskeletal disease. | Active, untreated pulmonary TB (high anesthesia risk); severe malnutrition (Albumin < 3.0 g/dL); profound, uncorrected immunosuppression. |
In modern orthopedic practice, the absolute contraindication of performing total joint arthroplasty in the setting of prior tuberculosis has been revised. Historically, arthroplasty was strictly avoided due to the catastrophic risk of reactivation. However, delayed arthroplasty is now considered a viable indication for patients with severe joint destruction, provided there is a minimum of 6 to 12 months of documented disease eradication via multidrug therapy, normalized inflammatory markers (ESR, CRP), negative intraoperative frozen sections for acute inflammation, and an immunocompetent host.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the bedrock of successful surgical management in musculoskeletal tuberculosis. The insidious nature of the disease often means that patients present with profound anatomical distortion, severe osteopenia, and compromised soft tissues.
The diagnostic and pre-operative workup must include a comprehensive laboratory panel. While the white blood cell (WBC) count is frequently normal, patients often exhibit normochromic or normocytic anemia indicative of chronic disease. Inflammatory markers, such as the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), must be trended to establish a baseline for post-operative monitoring. The gold standard for diagnosis remains the isolation of acid-fast bacilli (AFB) via smear and culture, though GeneXpert MTB/RIF assay is now critical for rapid detection of M. tuberculosis DNA and rifampicin resistance. Because synovial fluid cultures yield positive results in only 50% to 70% of cases, an open or arthroscopic synovial biopsy is highly recommended, increasing diagnostic yield to over 80%.
Advanced radiographic evaluation is mandatory. Plain radiographs should be scrutinized for Phemister's triad: juxta-articular osteoporosis, peripherally located osseous erosions, and gradual narrowing of the joint space. Digital templating must account for the severe juxta-articular osteoporosis, which often necessitates the use of load-sharing devices, intramedullary nails, or locking plate constructs rather than standard non-locking plates. Magnetic Resonance Imaging (MRI) with intravenous gadolinium is the modality of choice for evaluating the extent of soft-tissue involvement, synovial hypertrophy, skip lesions in the medullary canal, and the precise anatomical location of cold abscesses. Computed Tomography (CT) with 3D reconstruction is highly effective in delineating complex bony destruction, identifying sequestrum formation, and planning the trajectory of hardware in distorted anatomy.
Patient positioning is dictated by the specific joint involved and the planned surgical approach. For hip and pelvic debridement or arthroplasty, the patient is typically placed in the lateral decubitus position using a rigid pelvic positioner. The surgeon must ensure that the operative field is draped widely to allow for extensile approaches if a cold abscess extends into the retroperitoneal or thigh spaces. For knee arthrodesis, the patient is positioned supine with a radiolucent table to allow for unhindered intraoperative fluoroscopy from the hip to the ankle, ensuring accurate mechanical alignment of the intramedullary nail. A sterile tourniquet is utilized to minimize blood loss, though it must be released prior to closure to ensure meticulous hemostasis, as postoperative hematomas provide an ideal medium for secondary pyogenic infection. For foot and ankle reconstruction, the patient is positioned supine with an ipsilateral hip bump to internally rotate the leg, bringing the lateral hindfoot into a direct superior orientation for the extended lateral approach.
Step-by-Step Surgical Approach and Fixation Technique
Surgical intervention in musculoskeletal tuberculosis ranges from joint-preserving synovectomy in the early stages to complex arthrodesis or delayed arthroplasty in advanced stages. The overarching goals are the radical debridement of all caseous material, the restoration of mechanical stability, and the prevention of progressive deformity.
Foot and Ankle Reconstruction
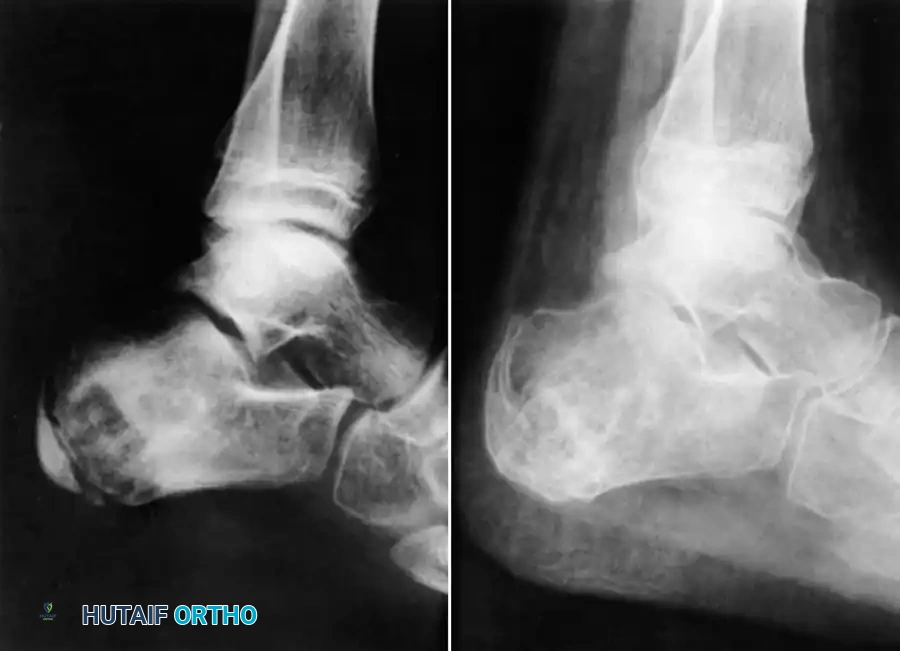
Tuberculosis of the foot and ankle frequently presents with massive midfoot swelling, chronic sinus tract formation, and severe pain upon weight-bearing. The calcaneus and talus are frequently involved, presenting with cystic, lytic lesions that can compromise the structural integrity of the entire hindfoot.
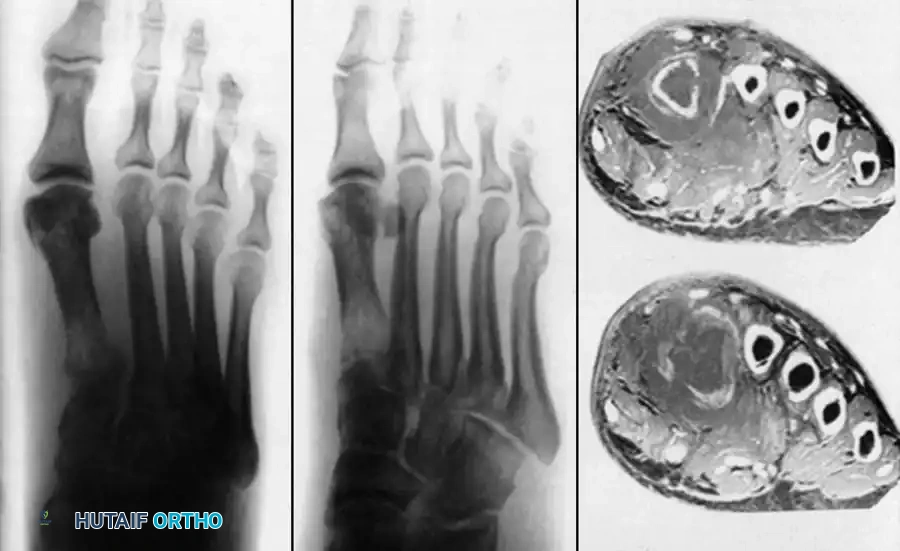
Advanced imaging often reveals extensive midfoot destruction and soft-tissue abscess formation. Surgical management in the early stages involves aggressive tenosynovectomy of the peroneal and posterior tibial tendons, combined with meticulous curettage of lytic lesions within the tarsal bones. Autologous cancellous bone grafting, typically harvested from the proximal tibia or iliac crest, may be required to fill massive cavitary defects in the calcaneus to prevent pathological fracture.
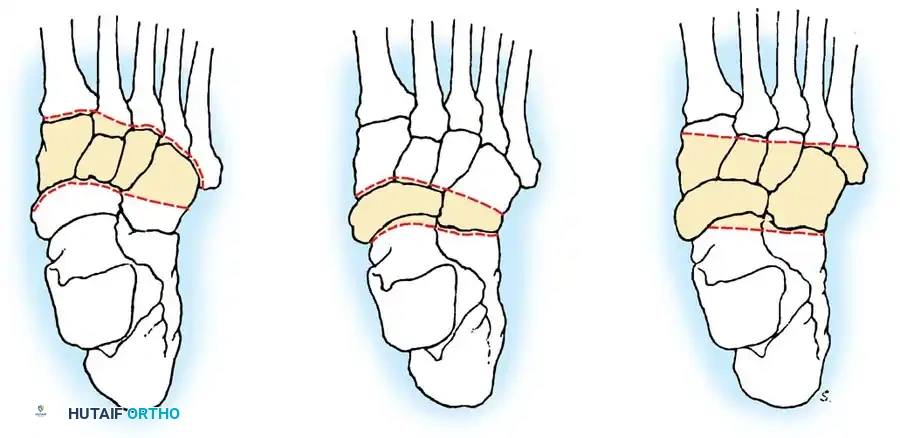
In advanced cases characterized by complete articular collapse and severe deformity, arthrodesis is the definitive treatment of choice. For combined midfoot and hindfoot involvement, a triple arthrodesis or tailored midfoot fusion is performed to restore a plantigrade, stable, and painless foot.
Surgical Technique: Tarsal Arthrodesis
1. Approach: An extended lateral approach (Ollier incision) is utilized to access the subtalar, calcaneocuboid, and talonavicular joints. If medial column destruction is severe, a supplementary medial incision over the talonavicular joint is employed.
2. Debridement: All infected synovium, caseous necrotic material, and devitalized cartilage are meticulously debrided down to healthy, bleeding subchondral bone. The use of a high-speed burr or sharp osteotomes is essential to expose the Haversian canals (fish-scaling) to promote robust osteogenesis.
3. Reduction: The joints are reduced into a highly functional position: neutral dorsiflexion, 5 degrees of hindfoot valgus, and external rotation matching the contralateral limb.
4. Fixation: Rigid stabilization is achieved using large-fragment (6.5mm or 7.3mm) cannulated screws. In osteopenic bone, rigid plate constructs (e.g., a locking calcaneocuboid or talonavicular plate) provide superior biomechanical stability compared to isolated screw fixation.
Knee Arthrodesis and Joint Preservation
The knee is the most commonly affected appendicular joint. Patients typically present with a boggy, swollen joint, severe quadriceps atrophy, and a rigid flexion contracture.

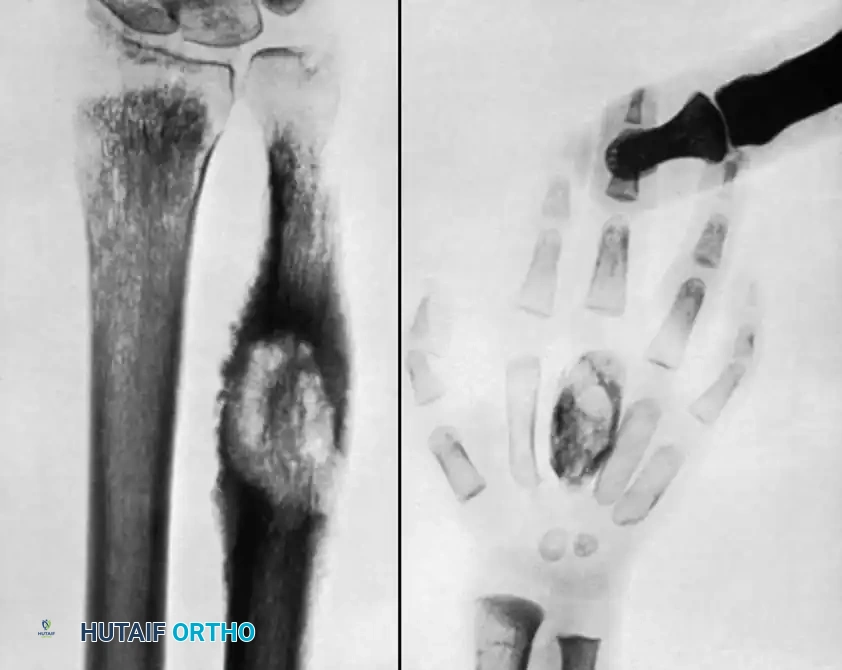
If diagnosed early in the synovial stage, before subchondral collapse occurs, arthroscopic or open synovectomy combined with systemic chemotherapy can successfully preserve joint function. However, once the subchondral bone is compromised and the articular cartilage is destroyed (as demonstrated in the radiograph above), joint preservation is no longer viable. In these scenarios, knee arthrodesis provides a highly stable, painless limb capable of full weight-bearing.
Surgical Management: Knee Arthrodesis
1. Approach: A standard anterior midline incision is made, extending from the distal third of the femur to the tibial tubercle, followed by a medial parapatellar arthrotomy.
2. Debridement: Radical synovectomy is performed, meticulously clearing the suprapatellar pouch and gutters. The menisci, anterior and posterior cruciate ligaments, and all infected bone are excised en bloc.
3. Bone Preparation: Flat, parallel cuts are made on the distal femur and proximal tibia using oscillating saws to ensure maximum cancellous bone contact. The knee must be positioned in 5 to 10 degrees of flexion to facilitate foot clearance during the swing phase of gait, and in neutral mechanical alignment (0 to 5 degrees of valgus).
4. Fixation: An antegrade intramedullary arthrodesis nail is the gold standard for rigid biomechanical stability. The canal is reamed sequentially, and a static locked nail is inserted. In cases where the medullary canal is obliterated or actively infected, a dual-plate construct (medial and anterior locking plates) or a multi-planar external fixator (Ilizarov frame) may be utilized.
Hip and Pelvic Debridement and Reconstruction
Tuberculosis of the hip frequently affects children and young adults. The disease typically begins in the acetabular roof or the femoral head, rapidly progressing to joint space narrowing and severe structural destruction. A classic late-stage presentation is the "wandering acetabulum," where superior and medial migration of the femoral head occurs due to progressive bone loss and the unopposed pull of the abductor musculature.

In cases of severe destruction, nonoperative management inevitably leads to a painful, fibrous ankylosis in a highly non-functional position (flexion, adduction, and internal rotation). Surgical intervention involves radical debridement of the joint. In modern practice, a two-stage total hip arthroplasty (THA) is often favored over traditional hip arthrodesis to maintain mobility and function, provided the infection is medically cleared. The first stage involves resection of the infected femoral head, radical acetabular debridement, and placement of an antibiotic-impregnated cement spacer. The second stage, performed 3 to 6 months later after normalization of inflammatory markers, involves the implantation of definitive THA components, often requiring complex acetabular reconstruction with trabecular metal augments or bone grafting.

Pelvic and sacroiliac (SI) joint tuberculosis often presents insidiously with lower back pain radiating to the gluteal region, closely mimicking sciatica or mechanical spondylosis. Radiographs and CT scans will demonstrate erosions and widening of the SI joint margins. Treatment is primarily medical, but large presacral or iliopsoas abscesses require CT-guided percutaneous drainage. If percutaneous methods fail, open surgical debridement via an anterior retroperitoneal approach or posterior SI approach is mandated to prevent intrapelvic organ compression.
Upper Extremity Arthrodesis
Upper extremity tuberculosis is less common than lower extremity involvement but is highly debilitating due to the critical need for hand and arm function in activities of daily living. The elbow and wrist are the most frequently affected sites.
The Elbow
Elbow tuberculosis often presents with a painful, swollen joint locked in partial flexion. Radiographs reveal extensive lytic destruction of the distal humerus, olecranon, and radial head, often with massive anterior and posterior fat pad signs indicative of a large effusion.

When the joint is irreparably damaged, elbow arthrodesis is indicated to provide a stable fulcrum for the hand, allowing for lifting and pushing activities that a flail or painful joint would preclude.
Surgical Technique: Elbow Arthrodesis
1. Approach: A posterior universal incision is utilized, curving laterally around the olecranon tip. The ulnar nerve must be meticulously identified, mobilized, and protected with a vessel loop to prevent iatrogenic injury or entrapment in the fusion mass.
2. Preparation: The olecranon fossa, trochlea, and capitellum are decorticated. The radial head is often excised if severely destroyed.
3. Positioning for Fusion: The elbow must be fused in a position of maximum function. For unilateral disease, this is typically 90 degrees of flexion with neutral forearm rotation. If the disease is bilateral, one elbow is fused at 110 degrees (to allow the hand to reach the mouth for feeding) and the other at 65 degrees (to facilitate perineal care and pushing off from a chair).
4. Fixation: Rigid fixation is achieved using heavy posterior plating (e.g., a 3.5mm or 4.5mm dynamic compression plate) spanning the posterior humerus to the proximal ulna, supplemented with cancellous bone graft.
The Wrist and Hand
Tuberculosis of the hand often presents as tuberculous dactylitis (spina ventosa), characterized by a painless, fusiform swelling of a phalanx or metacarpal. The bone expands, and the cortex thins dramatically, creating a cystic, "ballooned" appearance on radiographs.
Wrist involvement typically begins as a highly aggressive tenosynovitis of the flexor or extensor compartments before invading the carpal bones. If conservative management fails, extensive tenosynovectomy is required to prevent attritional tendon rupture.
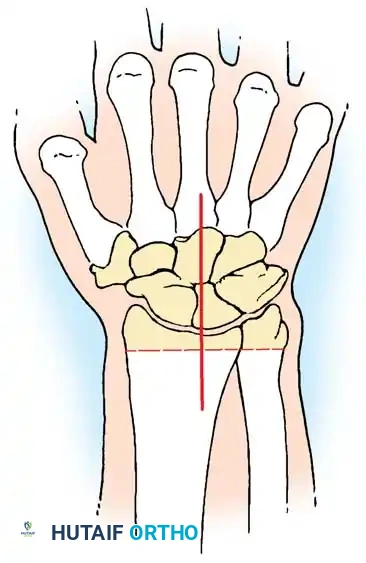
In cases of pan-carpal destruction, a total wrist arthrodesis is performed. The articular surfaces of the radiocarpal, midcarpal, and carpometacarpal joints are denuded of all cartilage and fibrous tissue. The wrist is fused in 10 to 15 degrees of extension to maximize grip strength, utilizing a dorsal spanning plate extending from the distal radius to the third metacarpal.
Complications, Incidence Rates, and Salvage Management
The surgical management of musculoskeletal tuberculosis is fraught with potential complications, largely due to the compromised host immune status, poor local tissue vascularity, and the inherently destructive nature of the mycobacterium.
| Complication | Estimated Incidence | Pathophysiology & Risk Factors | Salvage Management & Intervention |
|---|---|---|---|
| Reactivation of Infection | 5% - 10% | Inadequate duration of RIPE therapy; retained caseous necrotic tissue; severe immunosuppression (e.g., uncontrolled HIV). | Resume intensive phase RIPE therapy; aggressive repeat surgical debridement; removal of loose hardware. |
| Nonunion of Arthrodesis | 10% - 15% | Severe juxta-articular osteoporosis; inadequate rigid fixation; smoking; poor nutritional status (Albumin < 3.0). | Revision arthrodesis with robust autologous bone grafting (iliac crest); optimization of nutrition; use of bone stimulators. |
| Chronic Sinus Tract Formation | 8% - 12% | Incomplete excision of cold abscesses; superficial hardware prominence; secondary pyogenic superinfection (e.g., S. aureus). | Excision of the entire sinus tract; targeted antibiotic therapy for superinfection; local muscle flap coverage for soft-tissue defects. |
| Hardware Failure | 5% - 8% | Load-bearing prior to radiographic union; use of non-locking plates in osteopenic bone; patient non-compliance. | Revision internal fixation using load-sharing devices (intramedullary nails) or locking plate constructs; prolonged immobilization. |
| Neurological Deficit | 2% - 5% | Iatrogenic injury during extensive debridement (e.g., ulnar nerve in elbow, peroneal nerve in knee); compression from expanding cold abscess. | Immediate surgical decompression if secondary to abscess/hematoma; nerve exploration and neurolysis; physical therapy and orthotics. |
Salvage management requires a highly individualized approach. In catastrophic cases where revision arthrodesis fails, chronic osteomyelitis ensues, or the limb becomes a flail, painful appendage that severely diminishes the patient's quality of life, amputation (e.g., below-knee or above-knee amputation) may be indicated as a life-saving and function-restoring measure.
Phased Post-Operative Rehabilitation Protocols
Postoperative management of musculoskeletal tuberculosis requires a delicate, highly structured balance between protecting the surgical fixation to ensure bony union and preventing adjacent joint stiffness. The rehabilitation protocol is divided into distinct, closely monitored phases.
Phase 1: Acute Protection and Infection Control (Weeks 0-6)
Anti-tuberculous chemotherapy must be continued uninterrupted postoperatively. The total duration of therapy is typically 12 to 18 months for osseous involvement, guided strictly by clinical response and the normalization of inflammatory markers (ESR/CRP). During this acute phase, the operative limb is immobilized in a rigid cast or custom orthosis. For arthrodesis procedures, strict non-weight-bearing status is enforced. Deep vein thrombosis (DVT) prophylaxis is mandatory, given the prolonged immobility and systemic inflammatory state.
Phase 2: Early Mobilization of Adjacent Joints (Weeks 6-12)
Once early soft-tissue healing is confirmed and the acute postoperative pain subsides, active and active-assisted range of motion (ROM) exercises are initiated for all non-fused adjacent joints. For example, following a knee arthrodesis, aggressive hip and ankle ROM exercises are critical to prevent capsular contractures. Radiographs are obtained at the 6-week and 12-week marks to assess for early callus formation and hardware stability. Weight-bearing status is slowly advanced based on radiographic evidence of consolidation.
Phase 3: Strengthening and Proprioception (Months 3-6)
Once clinical and radiographic union is achieved, a phased, aggressive physical therapy program is initiated. The focus shifts to strengthening the musculature surrounding the fused or reconstructed joint to compensate for the altered biomechanics. Gait training with assistive devices is optimized, and proprioceptive drills are incorporated to improve balance and prevent falls
