Chronic Osteomyelitis: Comprehensive Surgical Management and Reconstruction
Key Takeaway
Chronic osteomyelitis is characterized by infected, necrotic bone within a compromised soft-tissue envelope. Eradication requires aggressive surgical debridement, complete sequestrectomy, and meticulous dead space management. This comprehensive guide details the Cierny-Mader classification, advanced diagnostic imaging, and step-by-step surgical techniques, including local muscle flaps and the Papineau technique, essential for achieving a viable, vascularized environment and preventing recurrence.
Comprehensive Introduction and Patho-Epidemiology
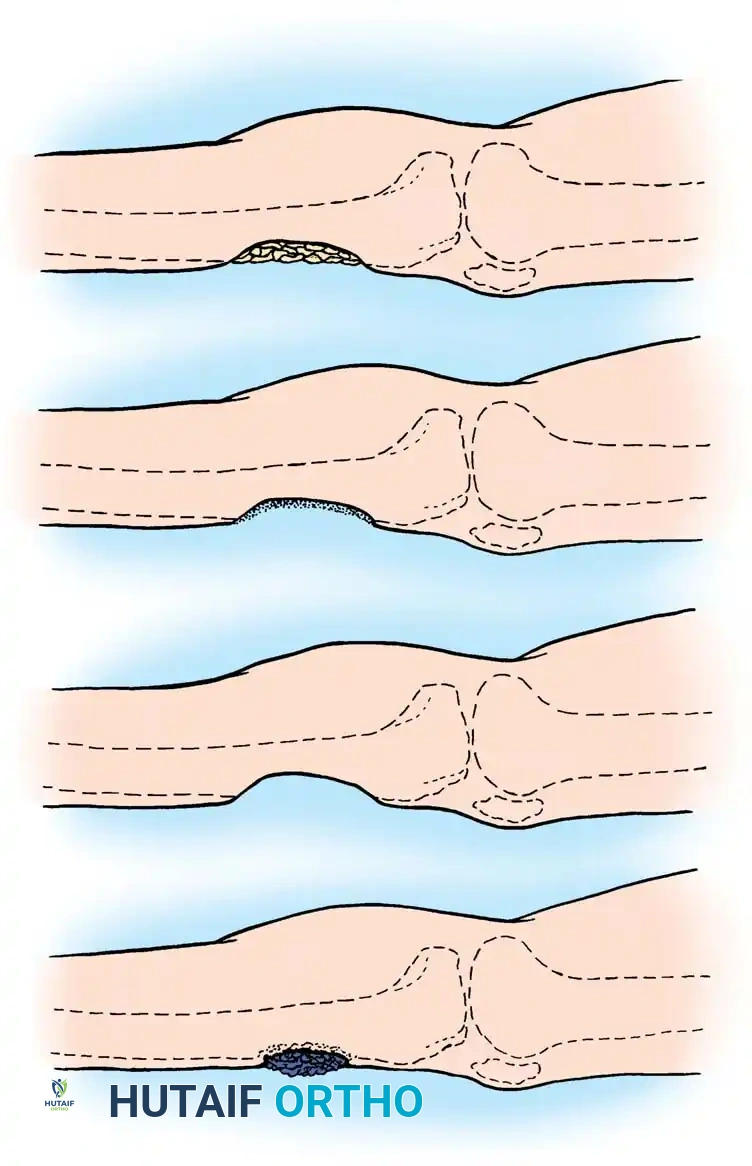
Chronic osteomyelitis remains one of the most formidable and persistently challenging pathologies encountered in orthopedic surgery. Unlike acute hematogenous osteomyelitis, which typically presents with a florid systemic inflammatory response and is often amenable to prompt antimicrobial therapy, chronic osteomyelitis is characterized by a protracted, indolent course punctuated by intermittent acute exacerbations. These exacerbations may span years or even decades, temporarily responding to suppressive antibiotic therapy and rest, only to recur with devastating local tissue destruction. The hallmark of this disease is the presence of non-viable, infected osseous tissue—the sequestrum—which acts as an impervious nidus for persistent bacterial colonization. This sequestrum is typically encased within a severely compromised, avascular soft-tissue envelope and surrounded by an involucrum of sclerotic, reactive bone.

At the molecular and microbiological level, the pathophysiology of chronic osteomyelitis is driven by the phenotypic transition of bacteria from a free-floating, planktonic state to a sessile, surface-attached state. This transition culminates in the formation of a complex glycocalyx biofilm—a slimy, extracellular polymeric substance composed of polysaccharides, proteins, and extracellular DNA. This biofilm confers profound evolutionary advantages to the offending pathogens, primarily Staphylococcus aureus, including methicillin-resistant (MRSA) strains. The biofilm acts as a formidable mechanical and physiological barrier, protecting the bacterial colony from host phagocytic cells, antibodies, and systemic antimicrobial agents. Furthermore, bacteria deep within the biofilm enter a metabolically dormant state, rendering them highly recalcitrant to bactericidal antibiotics that rely on active cellular division for efficacy. Consequently, the minimum inhibitory concentration (MIC) required to eradicate biofilm-encased bacteria can be up to 1,000 times higher than that required for their planktonic counterparts, a concentration impossible to achieve systemically without lethal host toxicity.
The epidemiological profile of chronic osteomyelitis is inextricably linked to high-energy trauma, complex open fractures, and the exponential rise of severe metabolic derangements such as diabetes mellitus and peripheral vascular disease. Post-traumatic osteomyelitis accounts for the vast majority of cases in adults, frequently resulting from severe open fractures (Gustilo-Anderson Type IIIB and IIIC) where the periosteal blood supply is stripped, and the zone of injury is contaminated with environmental debris. In the diabetic population, chronic osteomyelitis often presents as a contiguous spread from an infected neuropathic ulcer, complicated by macrovascular and microvascular ischemia. This creates a physiological environment where host immune cells and systemic antibiotics cannot physically reach the site of infection. Secondary polymicrobial infections are ubiquitous in these scenarios, and superficial sinus tract cultures notoriously fail to correlate with deep bone biopsy cultures, underscoring the absolute necessity for deep, operative sampling.
To navigate the immense complexity of this disease, the Cierny-Mader classification system remains the undisputed gold standard. Unlike traditional classifications based solely on etiology or duration, the Cierny-Mader system dynamically combines the anatomical extent of the osseous lesion with the physiological status of the host. Anatomically, lesions are categorized as Type I (Medullary), Type II (Superficial), Type III (Localized, full-thickness but mechanically stable), or Type IV (Diffuse, mechanically unstable). Physiologically, hosts are stratified into Class A (normal, immunocompetent), Class B (compromised locally or systemically), and Class C (prohibitive hosts where surgical morbidity outweighs potential benefits). This dual-axis system dictates that a Type III lesion in a diabetic, smoking patient (Stage IIIB-S) requires a vastly different, more cautious, and multidisciplinary approach compared to the same anatomical lesion in a young, healthy athlete (Stage IIIA).
Detailed Surgical Anatomy and Biomechanics
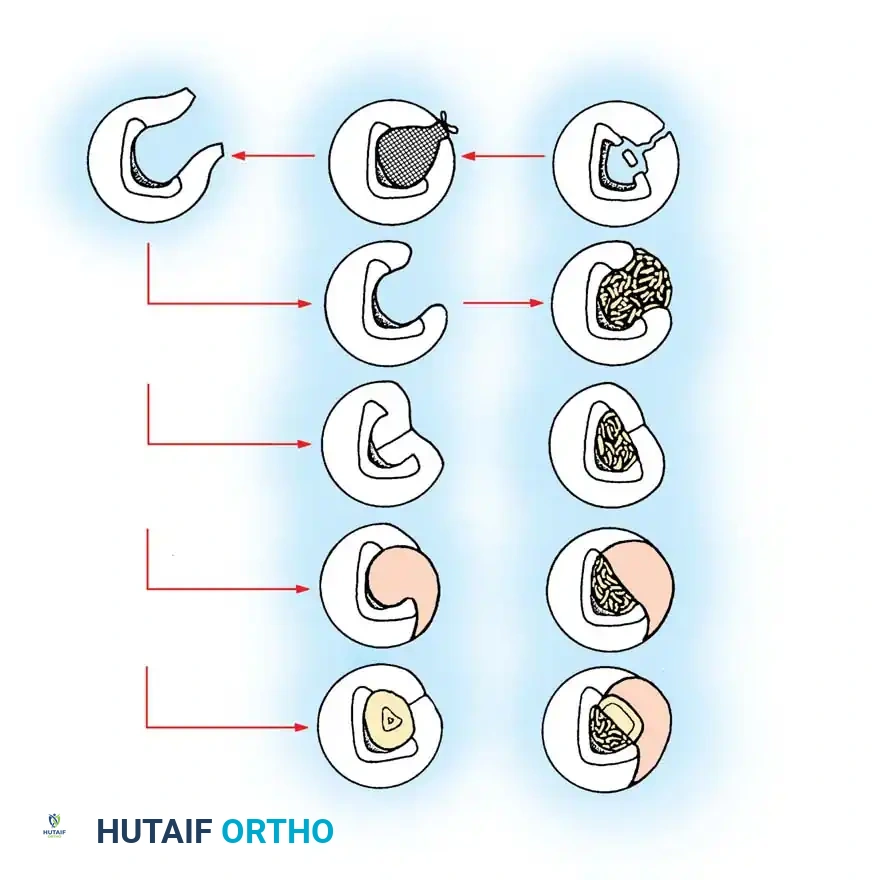
A profound understanding of osseous microvascular anatomy and macroscopic biomechanics is paramount when undertaking the surgical management of chronic osteomyelitis. Normal diaphyseal bone receives its blood supply via a dual system: the high-pressure nutrient artery system, which supplies the inner two-thirds of the cortex via the medullary canal, and the low-pressure periosteal system, which supplies the outer one-third of the cortex. In the setting of trauma or severe infection, this delicate vascular equilibrium is profoundly disrupted. Periosteal stripping during a high-energy injury or subsequent surgical exposure deprives the outer cortex of its blood supply. Simultaneously, intramedullary infection leads to suppurative thrombosis of the medullary vessels. The consequence is a segment of cortical bone completely devoid of perfusion—the genesis of the sequestrum.
As the host immune system attempts to wall off this necrotic, infected focus, osteoclastic resorption occurs at the junction of living and dead bone, physically separating the sequestrum. Concurrently, the surviving periosteum mounts a vigorous osteoblastic response, laying down a thick, irregular layer of reactive bone known as the involucrum. While the involucrum represents an attempt to restore structural integrity, it is highly sclerotic, poorly vascularized, and often incomplete, leaving defects known as cloacae through which purulent material and small osseous fragments are extruded into the surrounding soft tissues, eventually forming cutaneous sinus tracts. This avascular envelope of scar tissue and sclerotic bone creates a physiological dead space—an environment entirely isolated from systemic immune surveillance and antimicrobial penetration.
The biomechanical implications of chronic osteomyelitis and its subsequent surgical management are equally critical. The diaphyseal cortex functions as a hollow tubular structure, providing immense torsional and bending strength while minimizing mass. The presence of a localized cortical defect, whether created by the infectious process itself (cavitation) or by the surgeon during radical debridement (saucerization), drastically alters the stress distribution within the bone. A cortical window acts as a significant stress riser. According to the principles of solid mechanics, the torsional strength of a tubular bone is proportional to the polar moment of inertia. Even a relatively small, eccentrically placed cortical defect can reduce the torsional load to failure by over 50%.
Therefore, when an orthopedic surgeon converts a Type III (localized) lesion into a Type IV (diffuse) lesion via aggressive resection, the biomechanical stability of the limb is fundamentally compromised. The remaining cortical bridge, often composed of brittle, sclerotic involucrum, is highly susceptible to pathological fracture under physiological loading. This mandates a proactive approach to stabilization, often necessitating the application of rigid external fixation, such as an Ilizarov circular frame, which bypasses the zone of structural weakness and allows for early, protected weight-bearing while the reconstructed osseous defect undergoes consolidation and remodeling according to Wolff's Law.
Exhaustive Indications and Contraindications
The decision to embark on the surgical eradication of chronic osteomyelitis is one of the most complex judgments in orthopedic surgery. The surgeon must meticulously balance the absolute necessity of eradicating the infection against the severe morbidity of radical bone resection, prolonged immobilization, and the psychological toll on the patient. The primary indication for surgical intervention is the presence of symptomatic, active chronic osteomyelitis in a patient who possesses the physiological reserve to tolerate multiple complex reconstructive procedures. Symptoms dictating intervention include intractable osseous pain, persistent purulent drainage via sinus tracts, recurrent episodes of systemic sepsis originating from the osseous focus, and the impending or actual pathological fracture of the compromised bone.
Another critical, albeit less common, indication for radical surgical intervention is the malignant transformation of a chronic, draining sinus tract into a squamous cell carcinoma, known as a Marjolin's ulcer. This phenomenon, which typically occurs decades after the onset of the initial infection, represents an aggressive malignancy with a high propensity for metastasis. The presence of a Marjolin's ulcer mandates an immediate, aggressive oncological approach, frequently culminating in proximal amputation rather than limb salvage, to ensure clear margins and prevent systemic dissemination. Furthermore, the failure of prolonged suppressive antibiotic therapy to control symptoms or prevent the progressive destruction of the joint or osseous architecture serves as a definitive indication for surgical debridement.
Conversely, the contraindications to complex limb-salvage surgery for chronic osteomyelitis are primarily dictated by the physiological status of the host, aligning with the Cierny-Mader Class C designation. Absolute contraindications include severe, uncorrectable arterial insufficiency where the local vascular bed is incapable of supporting wound healing or the integration of vascularized tissue transfers. Patients with profound, irreversible systemic compromise—such as end-stage renal disease, severe malnutrition, or advanced terminal illness—are not candidates for radical, multi-stage reconstruction. In these scenarios, the physiological burden of repeated surgeries, prolonged anesthesia, and massive blood loss vastly outweighs any potential benefit.
Below is an exhaustive matrix detailing the indications and contraindications for the surgical management of chronic osteomyelitis:
| Category | Specific Parameter | Clinical Rationale and Surgical Implications |
|---|---|---|
| Absolute Indications | Intractable Pain and Sepsis | Persistent, debilitating pain or recurrent systemic sepsis originating from the osseous focus mandates immediate radical debridement to remove the necrotic nidus. |
| Absolute Indications | Marjolin's Ulcer | Squamous cell carcinoma arising in a chronic sinus tract requires aggressive oncological resection, frequently necessitating proximal amputation to prevent metastasis. |
| Relative Indications | Persistent Draining Sinus | While a draining sinus may be managed with suppressive antibiotics, surgical excision is required for definitive cure and to prevent progressive bone destruction. |
| Relative Indications | Impending Pathological Fracture | Progressive osteolysis threatening the structural integrity of the diaphysis requires debridement and prophylactic stabilization (e.g., Ilizarov frame). |
| Absolute Contraindications | Cierny-Mader Class C Host | The patient's physiological reserve is so depleted that the morbidity of the required surgery outweighs the potential for cure. Palliative care or amputation is indicated. |
| Absolute Contraindications | Uncorrectable Ischemia | Severe peripheral arterial disease not amenable to endovascular or open bypass. The lack of perfusion guarantees failure of flaps, bone grafts, and wound healing. |
| Relative Contraindications | Active Tobacco Abuse | Nicotine causes profound microvascular vasoconstriction, drastically increasing the risk of flap failure and non-union. Surgery should be delayed until cessation is confirmed. |
| Relative Contraindications | Uncontrolled Diabetes Mellitus | HbA1c > 8.0% significantly impairs leukocyte function and wound healing. Optimization of glycemic control is mandatory prior to elective complex reconstruction. |
Pre-Operative Planning, Templating, and Patient Positioning
The successful eradication of chronic osteomyelitis demands exhaustive, multidisciplinary preoperative planning. The surgical team must typically include an orthopedic surgeon specializing in trauma or bone infection, a plastic surgeon highly skilled in microvascular tissue transfer, and an infectious disease specialist. The diagnostic workup must be comprehensive, beginning with a meticulous physical examination to assess the integrity of the soft-tissue envelope, map areas of induration and tenderness, and document the neurovascular status of the extremity. Laboratory studies, while often non-specific, are essential baselines. The Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP) are typically elevated and serve as vital markers for monitoring the response to treatment postoperatively.
Imaging is the cornerstone of preoperative templating. No single modality is entirely comprehensive; therefore, a multimodal approach is mandatory. High-quality orthogonal plain radiographs are the initial step, identifying gross cortical destruction, periosteal reaction, and the presence of radiopaque sequestra. If an active cutaneous sinus tract is present, sinography—the injection of a radiopaque contrast medium under fluoroscopy—can brilliantly delineate the tortuous course of the tract and pinpoint the deep osseous focus of the infection.

Advanced cross-sectional imaging is critical for precise surgical mapping. Computed Tomography (CT) provides unparalleled, high-resolution definition of the cortical bone architecture. It is the absolute superior modality for identifying small, occult sequestra hidden within sclerotic involucrum and for geometrically planning the exact margins of the required cortical resection. Magnetic Resonance Imaging (MRI), particularly T1 and fat-suppressed T2 sequences, is the modality of choice for evaluating the proximal and distal extent of intramedullary marrow edema and adjacent soft-tissue abscesses. The classic "rim sign"—a well-defined rim of high signal intensity surrounding an active disease focus—is highly suggestive of a chronic abscess. Nuclear medicine, specifically Indium-111-labeled leukocyte scans combined with Technetium-99m sulfur colloid marrow scans, offers high specificity for differentiating active infection from neuropathic osteoarthropathy or sterile post-traumatic inflammation.
Patient positioning and operating room setup must be meticulously orchestrated to facilitate both the radical extirpation of infected tissue and the subsequent complex reconstruction. The patient is typically positioned on a radiolucent Jackson table or a flat Jackson top to allow for unimpeded, multi-planar intraoperative fluoroscopy. Twenty-four hours prior to the surgical intervention, the cutaneous sinus tracts should be injected with sterile methylene blue dye. This technique effectively stains the fibrotic, infected epithelial tract, rendering it highly visible during surgery and ensuring its complete, en bloc excision. While a pneumatic tourniquet is frequently applied to the proximal limb to minimize blood loss during the initial, arduous exposure and soft-tissue dissection, it is an absolute imperative that the tourniquet be deflated prior to the final osseous debridement. The surgeon must be able to visualize the "Paprika sign"—punctate, bright red bleeding from healthy Haversian canals—which is the only reliable intraoperative clinical indicator of viable, adequately perfused bone.
Step-by-Step Surgical Approach and Fixation Technique
The surgical eradication of chronic osteomyelitis is predicated on a single, uncompromising principle: radical, oncological-style surgical debridement. Antibiotics, regardless of route or concentration, cannot sterilize a necrotic sequestrum or penetrate a mature bacterial biofilm. The surgeon must physically transform a necrotic, hypoxic, and infected environment into a viable, highly vascularized bed capable of supporting tissue regeneration and delivering systemic immune mediators. Inadequate debridement is the primary, overwhelming cause of disease recurrence. Landmark studies by Simpson et al. have definitively demonstrated that wide resection margins (greater than 5 mm of visibly healthy, bleeding bone) yield a near 0% recurrence rate, whereas marginal or intralesional resections result in unacceptably high failure rates, particularly in compromised hosts.
Exposure, Tract Excision, and Cortical Windowing
The surgical approach must be extensile, utilizing internervous and intermuscular planes to preserve the remaining vascular supply to the soft-tissue envelope. The incision typically incorporates the prior traumatic scars or surgical approaches, excising the compromised skin edges. The methylene blue-stained sinus tracts are meticulously dissected and excised en bloc down to their osseous origin. Upon reaching the bone, the indurated, thickened, and often infected periosteum is sharply incised. It is elevated minimally—typically 1.3 to 2.5 cm on each side of the lesion—just enough to expose the underlying sclerotic involucrum. Overzealous periosteal stripping must be strictly avoided, as it will further devascularize the underlying cortex and propagate the zone of necrosis.
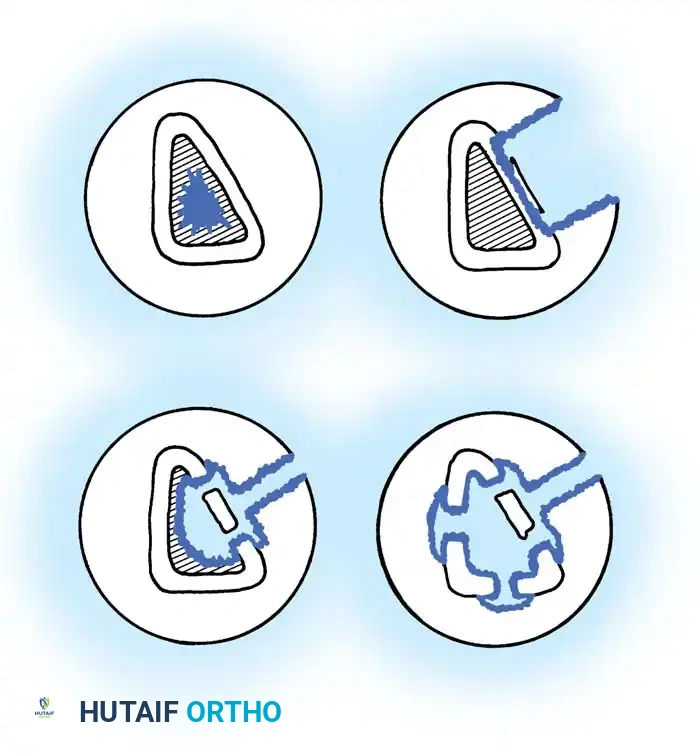
Once the involucrum is exposed, the surgeon utilizes a high-speed, water-cooled burr to outline a cortical window directly over the suspected intramedullary abscess or sequestrum, as mapped on the preoperative CT scan. The cortical window is then carefully elevated and removed using sharp, curved osteotomes. This exposes the medullary canal, revealing the purulent exudate, scarred intramedullary tissue, and the necrotic sequestrum.
Radical Curettage and Saucerization
The core of the procedure is the radical curettage and saucerization of the osseous defect. All macroscopic sequestra, purulent material, and fibrotic marrow must be aggressively evacuated using large curettes and pituitary rongeurs. If the medullary cavity is sealed off by sclerotic, avascular bone, the canal must be opened both proximally and distally using sequential reamers or high-speed burrs until healthy, bleeding marrow is encountered. Following the removal of all gross infection, the bone must be saucerized. This involves using a high-speed burr to bevel the overhanging cortical edges, transforming a deep, cavernous hole into a shallow, open saucer. This critical step prevents the formation of an inaccessible dead space where postoperative hematoma can accumulate, acting as a perfect culture medium for recurrent infection. The endpoint of debridement is the visualization of the "Paprika sign"—diffuse, punctate bleeding from the cortical Haversian canals and robust bleeding from the cancellous marrow.
Dead Space Management and Osseous Stabilization
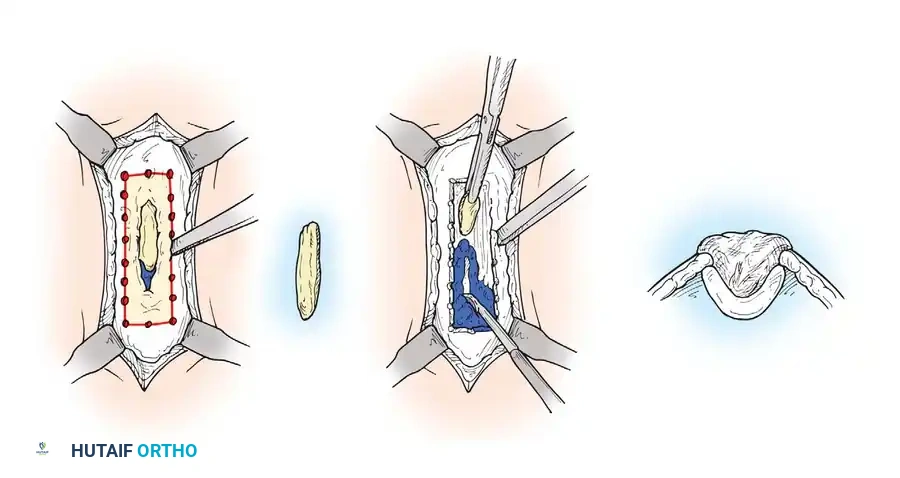
Radical debridement inevitably creates a massive osseous dead space that must be immediately and effectively managed. The primary technique for temporary dead space obliteration and local antimicrobial delivery is the utilization of antibiotic-impregnated polymethyl methacrylate (PMMA) beads. Heat-stable antibiotics, most commonly Vancomycin and Tobramycin, are thoroughly mixed with the PMMA polymer powder prior to the addition of the liquid monomer. This ensures an even distribution of the drug. The beads are molded and strung onto a heavy, non-absorbable suture or surgical stainless steel wire to facilitate straightforward removal during the subsequent reconstructive stage.
These PMMA beads serve a dual, synergistic purpose: they physically occupy the dead space, preventing hematoma accumulation, and they elute massive local concentrations of antibiotics directly into the surrounding tissue. Local tissue concentrations can reach levels 100 times the systemic minimum inhibitory concentration (MIC), effectively eradicating residual microscopic biofilm without inducing systemic renal or ototoxicity. The wound is then typically closed over the beads, or covered with a semi-permeable membrane (the "bead pouch" technique), creating a closed, high-concentration local environment.
Definitive reconstruction of the dead space occurs in a staged fashion, typically 3 to 6 weeks after the initial debridement, once the local environment is deemed sterile. The Papineau technique remains a classic, highly effective method for managing contained defects. It relies on the inherent infection resistance of highly vascularized granulation tissue and autogenous cancellous bone. Following the removal of the PMMA beads, the defect is densely packed with copious amounts of autogenous cancellous bone graft, ideally harvested from the anterior or posterior iliac crest using a Reamer-Irrigator-Aspirator (RIA) system to maximize volume and osteogenic potential.
If the radical debridement compromises the structural integrity of the diaphysis, converting a localized lesion into a diffuse, mechanically unstable Type IV lesion, rigid stabilization is absolutely mandatory. Internal fixation (plates and intramedullary nails) is generally contraindicated in the setting of active chronic infection due to the high risk of biofilm formation on the metallic implants. Therefore, an Ilizarov-type circular external fixator is the stabilization method of choice. Tensioned fine wires and half-pins are placed well outside the zone of infection, providing unparalleled biomechanical stability while avoiding the introduction of foreign hardware into the compromised bed. For massive segmental defects, the Ilizarov frame facilitates distraction osteogenesis (bone transport), allowing the surgeon to resect massive segments of infected bone and regenerate pristine, healthy osseous tissue through mechanical distraction, simultaneously addressing the infection and the structural deficit.
Complications, Incidence Rates, and Salvage Management
The surgical management of chronic osteomyelitis is fraught with severe, limb-threatening complications. Despite meticulous technique and modern antimicrobial regimens, the nature of the disease dictates a high baseline risk of failure. The most devastating complication is the recurrence of infection, which can manifest months, years, or even decades after an apparent clinical cure. Recurrence is almost universally the result of inadequate initial surgical debridement, where microscopic foci of infected, avascular bone or residual biofilm are left behind.
Another profound complication is the occurrence of a pathological fracture through the site of saucerization or cortical windowing. The mechanical weakening of the diaphysis, combined with the brittle nature of the surrounding sclerotic involucrum, creates a massive stress riser. If the patient is allowed to bear weight prematurely, or if the limb is inadequately protected with an external fixator or custom orthosis, catastrophic failure of the remaining cortical bridge can occur. Furthermore, the massive soft-tissue dissection required for radical exposure can lead to flap necrosis, wound dehiscence, and the exposure of the underlying bone or bone graft, necessitating emergent return to the operating room for further debridement and increasingly complex microvascular free tissue transfer.
When complications arise, salvage management must be aggressive and decisive. Recurrent infection demands a complete repetition of the surgical staging process: removal of all previously placed bone graft or hardware, radical re-debridement to bleeding bone, and the placement of new antibiotic PMMA beads. In cases of massive segmental bone loss complicated by recurrent infection or flap failure, the surgeon and patient must have a frank discussion regarding the limits of limb salvage. A proximal amputation (e.g., transtibial or transfemoral) may ultimately provide the patient with a faster return to functional mobility, eradication of systemic inflammatory burden, and a higher quality of life compared to endless, failing reconstructive procedures.
Below is a detailed matrix of common complications, their approximate incidence rates, and established salvage strategies:
| Complication | Estimated Incidence | Pathophysiology | Salvage Management Strategy |
|---|---|---|---|
| Recurrent Infection | 15% - 30% | Inadequate resection margins; retained sequestrum; failure to eradicate complex biofilm; compromised host immunity. | Radical re-debridement, removal of all grafts/hardware, new PMMA antibiotic beads, optimization of host physiology (Cierny-Mader Class B to A). |
| Pathological Fracture | 5% - 15% | Premature weight-bearing on a mechanically compromised diaphysis (stress riser from saucerization/cortical window). | Application of a circular external fixator (Ilizarov) to bypass the fracture, combined with autogenous bone grafting of the defect. |
| Flap Necrosis / Dehiscence | 10% - 20% | Microvascular thrombosis in free flaps; excessive tension on local rotational flaps; underlying hematoma or recurrent infection. | Emergent surgical exploration, evacuation of hematoma, revision of microvascular anastomoses, or utilization of a secondary, more proximal free flap. |
| Non-Union of Bone Graft | 10% - 25% | Avascular recipient bed; inadequate rigid stabilization; persistent low-grade infection; smoking/nicotine use. | Revision of fixation to increase mechanical stability, decortication of the non-union site, and application of highly osteogenic autogenous graft (e.g., RIA graft from femur). |
| Systemic Toxicity (Local Abx) | < 1% | Massive elution of aminoglycosides (Tobramycin) from PMMA beads leading to transient acute kidney injury or ototoxicity. | Immediate removal of the PMMA bead pouch, aggressive intravenous hydration, and consultation with nephrology. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation of a patient following radical reconstruction for chronic osteomyelitis is a protracted, highly phased process that requires rigorous compliance and close multidisciplinary monitoring. The immediate postoperative phase (Weeks 0-3) is intensely focused on wound healing, flap survival, and the optimization of systemic antimicrobial therapy. The operated limb is typically strictly elevated to minimize edema and venous congestion, particularly if a microvascular free flap has been utilized. The plastic surgery team will monitor the flap meticulously using clinical observation and handheld Doppler ultrasound. During this phase, weight-bearing is absolutely contraindicated. The patient is mobilized out of bed to a chair, and aggressive deep vein thrombosis (DVT) prophylaxis is instituted, as these patients are at high risk due to prolonged operative times and subsequent immobility.
The intermediate phase (Weeks 3-12) marks the transition to dead space reconstruction and the initiation of protected mechanical loading. If the patient was managed with a temporary PMMA bead pouch, they are returned to the operating room for bead removal and definitive autogenous bone grafting or the initiation of bone transport. Once the definitive reconstruction is stable, physical therapy focuses on maintaining the range of motion of the adjacent joints (knee and ankle) to prevent debilitating arthrofibrosis. If the limb is stabilized in an Ilizarov circular frame, the patient may begin touch-down to partial weight-bearing, as the axial micro-motion provided by the wire-based frame actually stimulates osteogenesis and graft incorporation. Serial radiographs are obtained every 4 weeks to monitor the incorporation of the cancellous graft or the consolidation of the regenerate bone in transport cases.
The late phase (Months 3-12+) is dedicated to functional restoration and the vigilant surveillance for disease recurrence. Weight-bearing is progressively advanced based on definitive radiographic evidence of cortical bridging and graft consolidation. Once full consolidation is achieved, external fixators are removed in the clinic or operating room, and the limb is often protected in a custom-molded functional orthosis for an additional 2 to 3 months to prevent refracture through the pin tracts. The orthopedic surgeon must maintain lifelong surveillance of these patients. Clinical examinations and laboratory markers (ESR, CRP) are evaluated at 6-month, and eventually annual, intervals. Any unexplained elevation in inflammatory markers, or the onset of new localized pain, must be treated with the highest degree of suspicion for recurrent osteomyelitis, prompting immediate advanced imaging.
Summary of Landmark Literature and Clinical Guidelines
The modern surgical management of chronic osteomyelitis is built upon a foundation of several landmark studies and evolving clinical guidelines that have fundamentally shifted orthopedic paradigms. The seminal work by Cierny and Mader in the 1980s revolutionized the approach to the disease by proving that the physiological status of the host is equally, if not more, predictive of surgical success than the anatomical extent of the bone lesion. Their classification system remains the universally accepted framework for preoperative planning and outcome reporting, establishing the absolute necessity of optimizing systemic factors (smoking cessation, glycemic control, nutritional repletion) prior to undertaking complex reconstruction.
In the realm of surgical technique, the concept of oncological-style margins in bone infection was definitively established by Simpson et al. Their critical analysis of resection margins demonstrated that a marginal resection (less than 5 mm of healthy bone) was associated with an unacceptably high recurrence rate of 28%, whereas a wide resection (greater than 5 mm of healthy, bleeding bone) reduced the recurrence rate to 0%. This literature mandates the aggressive use of high-speed burrs and the reliance on the intraoperative "Paprika sign" to ensure all microscopic biofilm and necrotic tissue are eradicated, fundamentally changing the tolerance for conservative debridement in chronic cases.
The management of the massive dead space created by these wide resections was revolutionized by the Masquelet technique (induced membrane technique). Alain Masquelet's landmark papers described a two-stage procedure: the initial placement of a PMMA cement spacer to maintain the dead space and induce a highly vascularized, osteoinductive foreign-body membrane, followed weeks later by the removal of the spacer and the packing of the defect with autogenous cancellous bone. This technique has largely supplanted older methods for massive diaphyseal defects, proving that the induced membrane secretes critical growth factors (VEGF, TGF-beta) that prevent the resorption of the massive bone graft and promote rapid corticalization.
Finally, the paradigm of postoperative antimicrobial therapy has been recently challenged and refined by the OVIVA (Oral Versus Intravenous Antibiotics
