Introduction to Musculoskeletal Tuberculosis
Current estimates indicate that up to one-third of the global population has been exposed to or infected by tuberculosis (TB). Despite advances in modern medicine, tuberculosis remains a leading cause of infectious mortality worldwide. The highest incidence rates are localized in Southeast Asia and sub-Saharan Africa. In North America, infection rates saw a dramatic resurgence in the late 1980s and early 1990s, driven largely by the human immunodeficiency virus (HIV) epidemic, rising immunosuppression, and increased immigration from endemic regions.
Populations at the highest risk include individuals with acquired immunodeficiency syndrome (AIDS), chronic renal failure, substance abuse disorders, and those living in densely populated or incarcerated settings. Foreign-born individuals account for over half of recent cases in the United States, with the highest risk of active disease occurring within the first five years of immigration.
Pathophysiology and Musculoskeletal Involvement
Tuberculosis is primarily transmitted via the inhalation of aerosolized Mycobacterium tuberculosis droplets. Following primary pulmonary infection, the bacilli can disseminate via lymphogenous or hematogenous routes to virtually any organ system. Extrapulmonary involvement occurs in approximately 14% of patients, with osseous disease manifesting in 1% to 8% of these cases.
Musculoskeletal tuberculosis most frequently targets the spine (Pott disease), accounting for 30% to 50% of osseous cases. In the appendicular skeleton, the disease demonstrates a strong predilection for major weight-bearing joints, particularly the hip and knee, followed by the foot, ankle, elbow, and hand.
Pathological Pearl: The hallmark of osseous tuberculosis is the formation of caseating granulomas containing multinucleated Langhans giant cells. Unlike pyogenic arthritis, which rapidly destroys articular cartilage via proteolytic enzymes, tuberculous arthritis initially spares the cartilage. The infection typically begins in the metaphyseal or subchondral bone, leading to gradual trabecular necrosis, subchondral collapse, and eventual detachment of the overlying articular cartilage.
Clinical Presentation and Diagnostic Evaluation
The clinical presentation of musculoskeletal tuberculosis is notoriously insidious, often leading to delayed diagnosis. Patients typically present with chronic, progressive joint pain, swelling, and a gradual loss of range of motion. Constitutional symptoms such as low-grade fever, night sweats, and weight loss may be present but are frequently absent in isolated osseous disease.
Peripheral joint involvement often mimics other rheumatological conditions, such as rheumatoid arthritis, gout, or pigmented villonodular synovitis (PVNS). A high index of suspicion must be maintained, particularly in immunocompromised patients, children under five, and the elderly.
Laboratory Findings
Routine laboratory tests are often nonspecific. The white blood cell (WBC) count is frequently normal, though patients may exhibit normochromic or normocytic anemia. Inflammatory markers, such as the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP), may be elevated but can also remain within normal limits.
The gold standard for diagnosis is the isolation of acid-fast bacilli (AFB) via smear and culture from synovial fluid or bone biopsy. Because synovial fluid cultures yield positive results in only 50% to 70% of cases, an open or arthroscopic synovial biopsy is highly recommended, increasing diagnostic yield to over 80%.
Advanced Imaging
Radiographic evaluation is critical for staging the disease and planning surgical intervention. The classic radiographic presentation of tuberculous arthritis is described by Phemister's triad:
1. Juxta-articular osteoporosis.
2. Peripherally located osseous erosions.
3. Gradual narrowing of the joint space.
Magnetic Resonance Imaging (MRI) is the modality of choice for evaluating soft-tissue extension, synovial hypertrophy, and the presence of "cold abscesses." Computed Tomography (CT) is highly effective in delineating bony destruction, sequestrum formation, and guiding percutaneous biopsies.
Nonoperative Management and Pharmacotherapy
The primary objectives in treating musculoskeletal tuberculosis are eradicating the infection, preventing or limiting deformity, maintaining joint mobility, and alleviating pain. A multidisciplinary approach involving orthopedic surgeons, infectious disease specialists, and physical therapists is paramount.
Approximately 90% of patients can be successfully managed with a prolonged course of multidrug chemotherapy, relative rest, and guided rehabilitation. The standard pharmacological regimen involves an intensive initial phase utilizing a combination of Isoniazid, Rifampin, Pyrazinamide, and Ethambutol (RIPE therapy) for 2 months, followed by a continuation phase of Isoniazid and Rifampin for an additional 7 to 10 months.
Adjunctive splinting is crucial during the acute phase to prevent contractures. If joint destruction is severe and spontaneous ankylosis is anticipated, the extremity must be immobilized in a functional position. Although the use of systemic corticosteroids to reduce the inflammatory response and prevent severe complications such as arachnoiditis or constrictive pericarditis remains controversial, it is often considered in cases of profound neurological deficit or miliary dissemination.
Principles of Operative Treatment
Surgical intervention is indicated when there is a failure of medical therapy, progressive neurological deficit, severe joint destruction, impending instability, or the presence of a large, symptomatic cold abscess. The goals of surgery range from joint-preserving synovectomy and debridement in early stages to arthrodesis or resection arthroplasty in advanced stages.
Surgical Warning: Total joint arthroplasty in the setting of active tuberculosis is historically contraindicated due to the high risk of persistent infection. However, in modern practice, delayed arthroplasty may be considered after a minimum of 6 to 12 months of documented disease eradication via multidrug therapy, provided the patient is immunocompetent.
The Foot and Ankle
Tuberculosis of the foot and ankle often presents with midfoot swelling, sinus tract formation, and severe pain upon weight-bearing. The calcaneus and talus are frequently involved, presenting with cystic, lytic lesions that can compromise the structural integrity of the hindfoot.
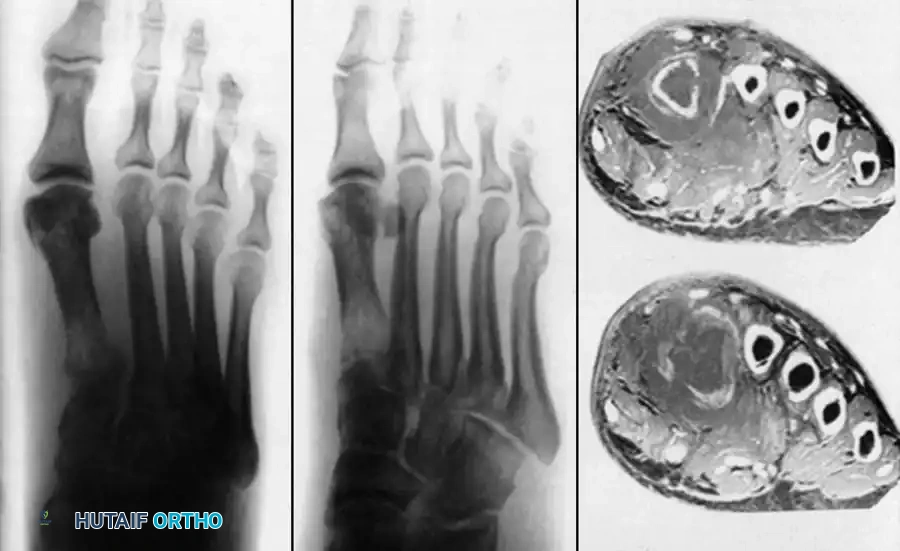
Advanced imaging, as seen above, often reveals extensive midfoot destruction and soft-tissue abscess formation. Surgical management in the early stages involves aggressive tenosynovectomy and curettage of lytic lesions. Bone grafting may be required to fill cavitary defects in the calcaneus.
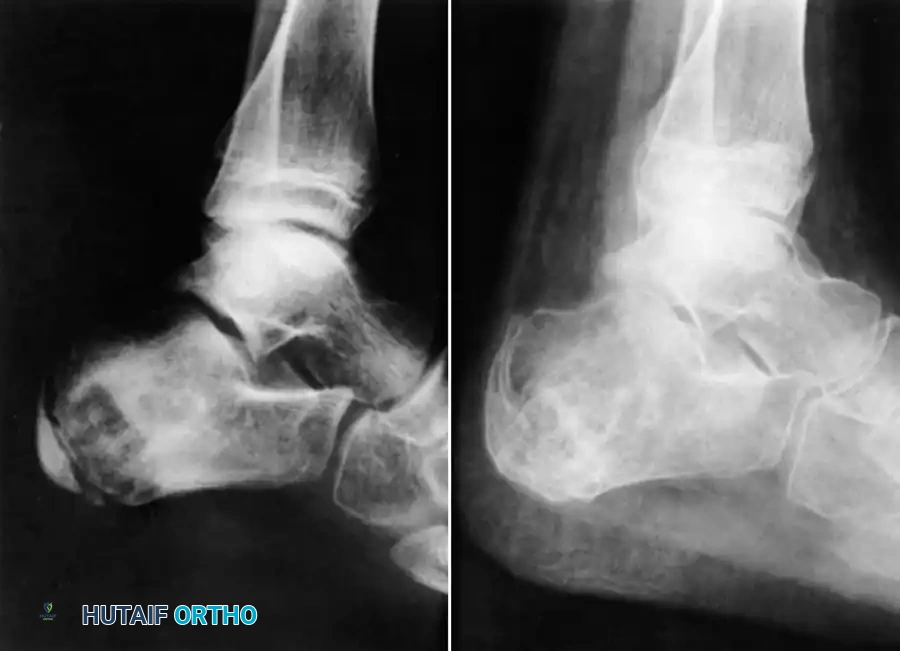
In advanced cases with articular collapse, arthrodesis is the treatment of choice. For midfoot and hindfoot involvement, a triple arthrodesis or tailored midfoot fusion is performed to restore a plantigrade, stable foot.
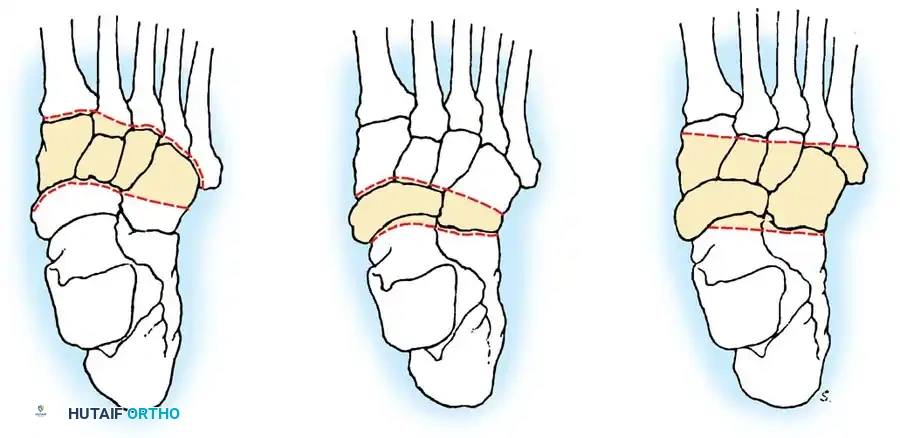
Surgical Technique: Tarsal Arthrodesis
1. Positioning: Supine with a bump under the ipsilateral hip to internally rotate the leg.
2. Approach: An extended lateral approach is utilized to access the subtalar, calcaneocuboid, and talonavicular joints.
3. Preparation: All infected synovium, caseous material, and necrotic cartilage are meticulously debrided down to bleeding subchondral bone.
4. Fixation: The joints are reduced into a functional position (neutral dorsiflexion, 5 degrees of valgus) and stabilized using large-fragment cannulated screws or rigid plate constructs.
The Knee
The knee is the most commonly affected appendicular joint. Patients present with a boggy, swollen joint, severe quadriceps atrophy, and a flexion contracture.

If diagnosed early (synovial stage), arthroscopic synovectomy combined with chemotherapy can preserve joint function. However, once the subchondral bone is compromised and the articular cartilage is destroyed (as demonstrated in the radiograph above), joint preservation is no longer viable.
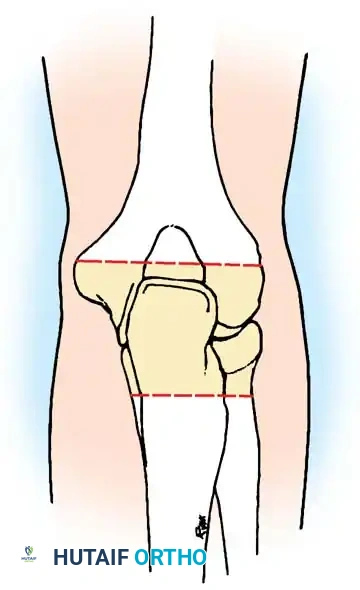
Surgical Management: Knee Arthrodesis
For advanced destruction, knee arthrodesis provides a stable, painless limb.
1. Approach: A standard anterior midline incision with a medial parapatellar arthrotomy.
2. Debridement: Radical synovectomy and excision of the menisci, cruciate ligaments, and infected bone.
3. Bone Cuts: Flat cuts are made on the distal femur and proximal tibia to ensure maximum cancellous bone contact. The knee is positioned in 5 to 10 degrees of flexion and neutral mechanical alignment.
4. Fixation: An intramedullary nail or dual-plate construct is utilized for rigid biomechanical stability.
The Hip and Pelvis
Tuberculosis of the hip frequently affects children and young adults. The disease begins in the acetabular roof or the femoral head, rapidly progressing to joint space narrowing and severe destruction. A classic late-stage presentation is the "wandering acetabulum," where superior and medial migration of the femoral head occurs due to progressive bone loss.

In cases of severe destruction, nonoperative management leads to painful, fibrous ankylosis in a non-functional position (flexion, adduction, and internal rotation). Surgical intervention involves radical debridement. In modern practice, a two-stage total hip arthroplasty (THA) is often favored over hip arthrodesis to maintain mobility, provided the infection is medically cleared.

Pelvic and sacroiliac (SI) joint tuberculosis often presents with lower back pain radiating to the gluteal region, mimicking sciatica. Radiographs and CT scans will show erosions of the SI joint margins. Treatment is primarily medical, but large presacral or iliopsoas abscesses require CT-guided percutaneous drainage or open surgical debridement.
The Upper Extremity: Shoulder, Elbow, and Wrist
Upper extremity tuberculosis is less common but highly debilitating. The elbow and wrist are the most frequently affected sites in the arm.
The Elbow
Elbow tuberculosis often presents with a painful, swollen joint locked in partial flexion. Radiographs reveal extensive lytic destruction of the distal humerus, olecranon, and radial head.

When the joint is irreparably damaged, elbow arthrodesis is indicated to provide a stable fulcrum for the hand.
Surgical Technique: Elbow Arthrodesis
1. Positioning: Lateral decubitus or supine with the arm draped across the chest.
2. Approach: A posterior universal incision. The ulnar nerve must be identified, mobilized, and protected.
3. Preparation: The olecranon fossa and trochlea are decorticated.
4. Positioning for Fusion: The elbow must be fused in a position of maximum function. For unilateral disease, this is typically 90 degrees of flexion. If bilateral, one elbow is fused at 110 degrees (to reach the mouth) and the other at 65 degrees (for perineal care).
5. Fixation: Rigid fixation is achieved using posterior plating spanning the humerus and ulna.
The Wrist and Hand
Tuberculosis of the hand often presents as tuberculous dactylitis (spina ventosa), characterized by a painless, fusiform swelling of a phalanx or metacarpal. The bone expands, and the cortex thins, creating a cystic appearance.
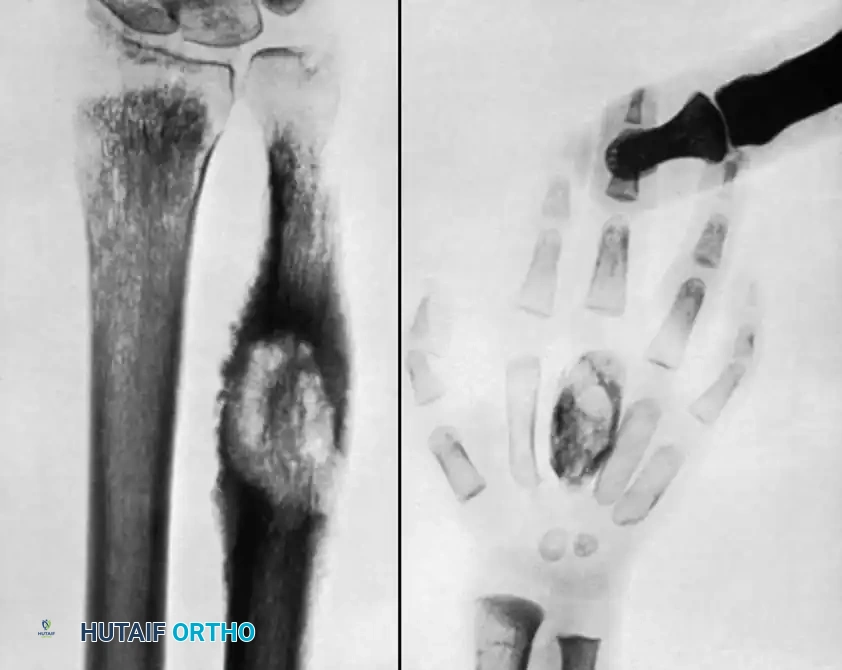
Wrist involvement typically begins as a tenosynovitis of the flexor or extensor compartments before invading the carpal bones. If conservative management fails, extensive tenosynovectomy is required to prevent tendon rupture.
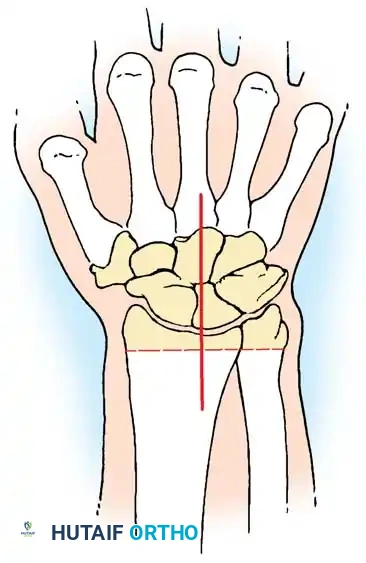
In cases of pan-carpal destruction, a total wrist arthrodesis is performed. The articular surfaces of the radiocarpal and intercarpal joints are denuded. The wrist is fused in 10 to 15 degrees of extension to maximize grip strength, utilizing a dorsal spanning plate from the distal radius to the third metacarpal.
Postoperative Protocols and Rehabilitation
Postoperative management of musculoskeletal tuberculosis requires a delicate balance between protecting surgical fixation and preventing adjacent joint stiffness.
- Infection Control: Anti-tuberculous chemotherapy must be continued uninterrupted postoperatively. The total duration of therapy is typically 12 to 18 months for osseous involvement, guided by clinical response and normalization of inflammatory markers (ESR/CRP).
- Immobilization: For arthrodesis procedures, the limb is immobilized in a rigid cast or orthosis for 8 to 12 weeks until radiographic evidence of bony union is observed.
- Rehabilitation: Once clinical union is achieved, a phased physical therapy program is initiated. Focus is placed on strengthening the musculature surrounding the fused joint and maximizing the compensatory range of motion in adjacent joints.
- Surveillance: Long-term follow-up is mandatory, as reactivation of latent tuberculosis can occur years after apparent clinical cure. Serial radiographs and clinical examinations should be conducted annually.
Associated Surgical & Radiographic Imaging

