Unusual Musculoskeletal Infections: Comprehensive Surgical Management
Key Takeaway
Atypical musculoskeletal infections, including nontuberculous mycobacteria, brucellosis, Lyme disease, and fungal osteomyelitis, present significant diagnostic and therapeutic challenges. These insidious pathogens often mimic common bacterial infections or neoplastic processes. Successful management requires a high index of suspicion, precise histopathological and microbiological identification, and a multidisciplinary approach. Surgical intervention—ranging from radical debridement and synovectomy to complex arthrodesis—is frequently necessary to eradicate chronic osteoarticular involvement and restore functional biomechanics.
Comprehensive Introduction and Patho-Epidemiology
While Staphylococcus aureus and standard pyogenic organisms account for the vast majority of osteoarticular infections, orthopaedic surgeons must maintain a high index of suspicion for atypical pathogens. The landscape of musculoskeletal infections has evolved significantly over the past several decades, driven by expanding immunocompromised populations, global travel, and increased exposure to endemic environmental niches. These unusual infections—ranging from nontuberculous mycobacteria (NTM) and zoonotic bacteria to endemic dimorphic fungi and spirochetes—often present with an insidious onset, frequently lacking the classic systemic signs of acute sepsis such as profound leukocytosis, high-grade fever, or elevated acute-phase reactants. Delayed diagnosis is the hallmark of these pathologies, often leading to devastating joint destruction, chronic osteomyelitis, and severe functional impairment before targeted therapy is initiated. Management mandates a synergistic, multidisciplinary approach combining prolonged, highly specific antimicrobial chemotherapy with meticulous surgical debridement, extensive synovectomy, and complex structural reconstruction.
Nontuberculous mycobacterial (NTM) infections have seen a marked increase in incidence since the mid-1980s. To date, the orthopaedic literature implicates at least fifteen different species of Mycobacterium in osteoarticular and tenosynovial infections. The most frequently isolated causative organisms include Mycobacterium avium complex (MAC), Mycobacterium marinum, and Mycobacterium kansasii. These organisms are ubiquitous in soil and water sources. M. marinum, for instance, is classically associated with aquatic environments, leading to the pathognomonic "fish tank granuloma" following minor penetrating trauma. Clinically, radiographically, and histopathologically, NTM infections are virtually indistinguishable from true musculoskeletal tuberculosis. They provoke a robust granulomatous inflammatory response, leading to chronic, progressive swelling, profound erythema, and restricted range of motion. The intracellular survival of these mycobacteria within macrophages allows them to evade standard host immune responses, leading to chronic, smoldering tissue destruction characterized by the formation of hypertrophic, avascular granulomatous tissue and characteristic "rice bodies" within synovial sheaths.
Zoonotic and spirochetal infections represent another critical category of atypical musculoskeletal pathology. Brucellosis, caused by a gram-negative coccobacillus, remains the most common zoonotic infection worldwide. Brucella melitensis (endemic in goats and sheep) and Brucella abortus (cattle) are transmitted via ingestion of unpasteurized dairy or direct contact with infected tissues. Approximately 66% of patients with brucellosis present with musculoskeletal symptoms, with spinal involvement (Brucella spondylitis) being the most common and dangerous manifestation. The organism demonstrates a profound tropism for the highly vascularized superior vertebral endplates, leading to localized osteomyelitis that frequently mimics tuberculous discitis. Similarly, Lyme disease, caused by the spirochete Borrelia burgdorferi and transmitted by Ixodes ticks, progresses to a late arthritic stage in up to 60% of untreated patients. Chronic Lyme arthritis triggers an aggressive, immune-mediated synovial hypertrophy and pannus formation, leading to cartilage degradation that closely mirrors rheumatoid arthritis in its destructive biomechanical consequences.
Endemic fungal infections of the musculoskeletal system, including Coccidioidomycosis, Blastomycosis, and Histoplasmosis, develop insidiously via hematogenous dissemination from primary pulmonary foci. Coccidioides immitis, endemic to the southwestern United States, causes granulomatous osseous lesions in approximately 15% of disseminated cases, typically targeting the metaphyses of tubular bones and bony prominences. Blastomyces dermatitidis exhibits a unique propensity to localize within the epiphysis of long bones, frequently extending directly into the adjacent joint space to cause a destructive, suppurative arthritis. Histoplasma capsulatum, while typically causing self-limiting pulmonary disease, can remain dormant in the bone marrow for decades before reactivating to cause profound lytic destruction of the carpus or other complex articulations. Because definitive diagnosis of these fungal osteomyelitides relies on specific fungal stains (e.g., Gomori methenamine silver, Periodic acid-Schiff) and prolonged cultures, the orthopaedic surgeon must suspect the diagnosis clinically based on geographic history, chronicity, and failure to respond to empiric antibacterial therapies.
Detailed Surgical Anatomy and Biomechanics
The surgical anatomy relevant to atypical musculoskeletal infections is dictated by the specific tropism of the causative organisms. Nontuberculous mycobacteria exhibit a profound affinity for the tenosynovial sheaths of the hand and wrist. The flexor tendon sheaths, specifically the radial and ulnar bursae, provide an enclosed, poorly vascularized environment ideal for mycobacterial proliferation. The visceral and parietal layers of the tenosynovium become drastically hypertrophied, producing fibrinous exudates that coalesce into macroscopic "rice bodies." Biomechanically, this massive synovial proliferation increases the volume within the rigid, unyielding constraints of the carpal tunnel and the digital fibro-osseous canals. This results in secondary median nerve compression (median neuropathy) and profound restriction of tendon excursion. Furthermore, the avascular nature of the granulomatous tissue prevents systemic antibiotics from achieving minimum inhibitory concentrations (MIC) at the site of infection, rendering medical management alone futile. Surgical anatomy in this region demands meticulous navigation of the palmar cutaneous branch of the median nerve, the recurrent motor branch, and the critical annular pulleys (A2 and A4) which must be preserved to prevent bowstringing and catastrophic loss of digital flexion biomechanics.
In the axial skeleton, Brucella and Salmonella species exhibit distinct anatomical predilections. Brucella spondylitis most frequently affects the lower lumbar spine. The vascular anatomy of the vertebral body, characterized by nutrient arteries that terminate in complex capillary loops immediately adjacent to the cartilaginous endplate, serves as the primary entry point for hematogenous seeding. Unlike pyogenic S. aureus spondylodiscitis, which rapidly destroys the intervertebral disc via proteolytic enzymes, Brucella often begins as an anterior endplate lesion. This creates a characteristic "parrot beak" osteophytic configuration on plain radiographs due to reactive periosteal bone formation. As the infection progresses, it compromises the structural integrity of the anterior column, leading to progressive kyphotic deformity. The biomechanical failure of the anterior column shifts axial loads to the posterior elements, exacerbating pain and instability. Furthermore, extension of the infection into the epidural space via Batson’s venous plexus can result in epidural abscesses that perfectly mimic the neurological presentation of a herniated nucleus pulposus, compressing the traversing nerve roots or the cauda equina.
The knee joint is the primary anatomical battleground for late-stage Lyme arthritis. The synovial membrane of the knee is the largest in the human body, featuring extensive recesses including the suprapatellar pouch, the medial and lateral gutters, and the posterior compartments. Borrelia burgdorferi induces a massive localized immune response, resulting in villous hypertrophy of the synovium and the formation of a destructive pannus. Biomechanically, the hypertrophic pannus physically impedes terminal extension and full flexion, while its enzymatic activity degrades the articular cartilage matrix. The surgical anatomy of the knee dictates that an arthroscopic synovectomy must be comprehensive; failure to access and clear the posterior compartments via posteromedial and posterolateral portals will leave a reservoir of infected, hypertrophic tissue that will inevitably lead to recurrent symptoms and progressive joint destruction.
Fungal osteomyelitis presents unique anatomical challenges, particularly when involving complex multi-articulating regions such as the carpus. The carpal bones are covered extensively by articular cartilage, leaving only small, non-articular surfaces for vascular penetration (e.g., the dorsal ridge of the scaphoid). This tenuous blood supply makes the carpus highly susceptible to avascular necrosis and rapid destruction once infiltrated by organisms like Histoplasma capsulatum or Coccidioides immitis. The biomechanical consequences of fungal carpal osteomyelitis are severe; destruction of the radiocarpal or midcarpal articulations leads to carpal collapse, loss of carpal height, and profound weakness in grip strength. Surgical intervention in this anatomical zone requires a delicate balance between radical debridement of necrotic, infected bone and the preservation of sufficient structural stock to allow for eventual arthrodesis or reconstructive salvage procedures.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention in the setting of atypical musculoskeletal infections requires a nuanced understanding of the pathogen's behavior, the efficacy of available antimicrobial agents, and the degree of structural compromise. Unlike acute pyogenic infections where emergent surgical debridement is universally mandated, atypical infections often allow for a trial of targeted medical therapy. However, when medical therapy fails or structural integrity is threatened, definitive surgical management becomes imperative.
| Pathogen / Disease State | Primary Surgical Indications | Relative & Absolute Contraindications |
|---|---|---|
| Nontuberculous Mycobacteria (NTM) | - Failure of 3-6 months of targeted multidrug therapy. - Progressive tenosynovitis with impending tendon rupture. - Severe compressive neuropathy (e.g., acute carpal tunnel syndrome). - Extensive "rice body" formation visible on MRI. |
- Relative: Early, mild disease responsive to initial antimicrobial therapy. - Absolute: Medically unstable patient unable to tolerate prolonged anesthesia. |
| Brucella Spondylitis | - Progressive neurological deficit (cauda equina or root compression). - Severe spinal instability or progressive kyphotic deformity. - Large, refractory psoas or epidural abscesses causing mechanical compression. |
- Relative: Isolated endplate changes without instability or neurological deficit (treat medically). - Absolute: Active, untreated systemic brucellosis without prior initiation of appropriate antibiotics (risk of dissemination). |
| Lyme Arthritis (Late Stage) | - Chronic monoarticular/oligoarticular arthritis refractory to 2-3 months of appropriate IV/oral antibiotics. - Massive synovial hypertrophy causing mechanical block to motion. - Impending cartilage destruction documented on serial imaging. |
- Relative: Acute inflammatory phase prior to completion of standard antibiotic protocols. - Absolute: Advanced degenerative joint disease (osteoarthritis) where synovectomy will not alter the natural history (consider arthroplasty post-clearance). |
| Fungal Osteomyelitis (e.g., Histoplasmosis, Coccidioidomycosis) | - Progressive lytic destruction threatening joint integrity. - Formation of large intra-osseous abscesses or sequestra. - Failure of prolonged systemic antifungal therapy (e.g., Amphotericin B, Itraconazole). - Need for definitive tissue diagnosis via open biopsy. |
- Relative: Small, asymptomatic, heavily sclerotic lesions without joint extension. - Absolute: Disseminated, uncontrolled fungemia in a profoundly immunocompromised host where surgical stress may precipitate multi-organ failure. |
| Syphilitic Osteitis / Charcot Arthropathy | - Severe instability in a neuropathic joint requiring arthrodesis. - Impending pathological fracture in tertiary syphilis. |
- Relative: Active, untreated Treponema pallidum infection. - Absolute: Standard internal fixation techniques without robust augmentation (due to universal failure in neuropathic bone). |
Surgical intervention in these scenarios is not merely for source control; it is fundamentally reconstructive. For instance, in NTM tenosynovitis, the indication for surgery is often driven by the mechanical threat to the flexor tendons. The hypertrophic synovium infiltrates the tendon substance, leading to attritional rupture. Therefore, surgery is indicated before rupture occurs, as reconstructing a ruptured flexor tendon in a bed of chronic mycobacterial infection carries a dismal prognosis. Conversely, operating too early on a suspected fungal osteomyelitis without establishing a definitive tissue diagnosis and initiating appropriate antifungal therapy can lead to catastrophic local dissemination and wound breakdown.
Contraindications are primarily related to the timing of the intervention and the physiological status of the host. In Brucella spondylitis, isolated anterior endplate destruction without kyphosis or neurological compromise is a strict contraindication to surgery; these patients respond exceptionally well to prolonged courses of doxycycline and rifampin. Operating on such lesions exposes the patient to unnecessary surgical morbidity and the risk of hardware superinfection. Similarly, in late-stage Lyme arthritis, arthroscopic synovectomy is contraindicated until the patient has exhausted a full course of disease-modifying antibiotic therapy, as premature surgical intervention fails to address the underlying systemic spirochetal burden and often results in rapid recurrence of the pannus.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the cornerstone of successful surgical management for atypical musculoskeletal infections. The diagnostic workup must be exhaustive. Because standard cultures are frequently negative, the orthopaedic surgeon must explicitly communicate with the microbiology laboratory. For suspected NTM infections, the laboratory must be instructed to incubate cultures at specific temperatures; for example, M. marinum requires incubation at 30ºC to 33ºC, and standard 37ºC incubation will yield false-negative results. Furthermore, specialized media such as Lowenstein-Jensen or Middlebrook agar, and extended incubation periods (up to 6 to 8 weeks), are mandatory. Advanced molecular diagnostics, including polymerase chain reaction (PCR) and next-generation sequencing of synovial fluid or tissue biopsies, have become indispensable tools for rapid pathogen identification and should be planned for during the initial diagnostic aspiration or biopsy.
Advanced imaging is critical for surgical templating and approach selection. Magnetic Resonance Imaging (MRI) with and without intravenous gadolinium contrast is the modality of choice for evaluating the extent of synovial hypertrophy, tenosynovial involvement, and epidural extension. In NTM infections of the hand, T2-weighted MRI sequences will classically demonstrate extensive fluid within the tendon sheaths interspersed with multiple small, low-signal-intensity nodules representing "rice bodies." Computed Tomography (CT) is essential for evaluating bony architecture, particularly in Brucella spondylitis and fungal osteomyelitis. CT accurately delineates the extent of vertebral body destruction, the presence of sequestra, and the degree of kyphotic deformity, allowing the surgeon to template the size of structural allografts or titanium mesh cages required for anterior column reconstruction.
Patient positioning and operating room setup must be meticulously planned to facilitate extensile exposures and complex reconstructions. For radical tenosynovectomy of the hand and wrist in NTM infections, the patient is positioned supine with the affected extremity extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm, and the limb is exsanguinated to ensure an absolutely bloodless field, which is critical for identifying and preserving the digital nerves and annular pulleys amidst the dense granulomatous tissue. Fluoroscopy should be available to confirm the integrity of the bony structures if concurrent osteomyelitis is suspected.
For the surgical management of Brucella spondylitis, positioning depends on the selected approach. Anterior debridement and corpectomy of the lumbar spine typically require the patient to be in the lateral decubitus position for a retroperitoneal approach. The patient is secured with rigid bean bags and adhesive taping, ensuring the iliac crest is accessible if autologous structural bone grafting is planned. Intraoperative neuromonitoring (somatosensory evoked potentials and motor evoked potentials) is established prior to positioning and monitored continuously, particularly when decompressing epidural Brucella abscesses. For arthroscopic synovectomy in Lyme arthritis, the patient is positioned supine with the operative leg in a standard leg holder, allowing for full flexion and manipulation of the knee to access the posterior compartments. A thigh tourniquet is utilized, and an arthroscopic fluid management system is essential to maintain joint distension and clear the visual field of hypertrophic debris.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution for atypical infections requires a radical approach to debridement, akin to oncologic resection, balanced with meticulous preservation of essential biomechanical structures. The following details the specific surgical techniques for the most commonly encountered atypical pathogens.
Radical Tenosynovectomy for Nontuberculous Mycobacteria (NTM)
The operative principles for NTM infections of the hand and wrist mirror those of musculoskeletal tuberculosis. Medical management alone is insufficient due to poor antibiotic penetration into hypertrophic, avascular granulomatous tissue.
- Incision and Exposure: Utilize an extensile volar approach. Begin with a longitudinal incision over the carpal tunnel, extending proximally into the distal forearm via a Brunner zigzag pattern across the wrist flexion creases to prevent postoperative contractures. Distally, the incision can be extended into the affected digits using mid-axial or volar zigzag incisions.
- Neurological Protection: Identify the median nerve proximally in the forearm between the flexor digitorum superficialis (FDS) and flexor carpi radialis (FCR). Trace it distally, carefully dissecting it free from the surrounding hypertrophic synovium. The transverse carpal ligament is routinely and completely released to decompress the carpal tunnel. Identify and protect the recurrent motor branch of the median nerve.
- Radical Debridement: Perform a meticulous, radical tenosynovectomy. Exise all hypertrophic, "rice body"–laden synovium from the radial and ulnar bursae. The granulomatous tissue often tenaciously adheres to the epitenon; use tenotomy scissors and blunt dissection to peel the diseased tissue away from the FDS and flexor digitorum profundus (FDP) tendons.
- Pulley Preservation: As the dissection proceeds distally into the digits, it is absolutely critical to preserve the A2 (proximal phalanx) and A4 (middle phalanx) annular pulleys. If the synovium is densely adherent beneath the pulleys, a small pediatric feeding tube or a dilator can be passed beneath the pulley to protect it while the synovium is stripped from the tendon.
- Closure and Drainage: Copious irrigation with pulsatile lavage is performed. The wound is closed primarily if tension-free. If severe skin compromise or massive edema exists, the wound is left open, dressed with a non-adherent interface, and scheduled for delayed primary closure or split-thickness skin grafting.
Anterior Debridement and Corpectomy for Brucella Spondylitis
When Brucella spondylitis causes progressive neurological deficit or structural collapse, anterior column reconstruction is mandated.
- Approach: A left-sided retroperitoneal approach is standard for the lumbar spine. The external oblique, internal oblique, and transversus abdominis muscles are divided in line with the incision. The peritoneum is swept medially, exposing the psoas muscle and the anterior longitudinal ligament.
- Vascular Mobilization: The aorta, inferior vena cava, and segmental vessels are carefully identified. Segmental vessels over the infected vertebral bodies are ligated and divided to allow complete mobilization of the great vessels away from the operative field.
- Corpectomy and Decompression: The infected intervertebral discs above and below the involved vertebra are excised. A radical corpectomy is performed using osteotomes, rongeurs, and a high-speed burr. All necrotic, infected bone and granulomatous tissue are removed until healthy, bleeding cancellous bone is encountered. The posterior longitudinal ligament is resected if necessary to completely decompress the epidural space and the traversing nerve roots.
- Structural Reconstruction: The resultant anterior column defect must be reconstructed. Autologous iliac crest bone graft (tricortical strut) or a titanium mesh cage packed with local healthy autograft/allograft is gently impacted into the defect.
- Instrumentation: To provide immediate biomechanical stability and promote fusion, an anterior locking plate system is applied, securing the construct to the healthy vertebral bodies adjacent to the corpectomy site. Supplemental posterior pedicle screw instrumentation may be required in cases of severe multi-level instability.
Arthroscopic Synovectomy for Refractory Lyme Arthritis
For chronic Lyme arthritis of the knee refractory to systemic antibiotics, complete eradication of the inflammatory pannus is required.
- Portal Placement: Standard anterolateral (viewing) and anteromedial (working) portals are established. However, due to the massive synovial hypertrophy, superomedial and superolateral portals are routinely required for complete access to the suprapatellar pouch.
- Anterior Synovectomy: Utilizing a motorized shaver (4.5mm or 5.5mm aggressive blade) and a radiofrequency ablation wand, a comprehensive anterior synovectomy is performed. The suprapatellar pouch, medial and lateral gutters, and the intercondylar notch must be meticulously cleared of all villous tissue. Care is taken not to damage the underlying articular cartilage.
- Posterior Compartment Clearance: The arthroscope is passed through the intercondylar notch (Gillquist maneuver) to visualize the posteromedial and posterolateral compartments. Accessory posteromedial and posterolateral portals are established under direct visualization. A shaver is introduced to resect the posterior pannus, which is often the source of recurrent disease if left untreated.
- Lavage and Closure: The joint is thoroughly irrigated with several liters of normal saline. The portals are closed with simple sutures, and a compressive dressing is applied.
Surgical Eradication of Fungal Osteomyelitis
Fungal osteomyelitis, such as that caused by Histoplasma capsulatum or Coccidioides immitis, requires aggressive osseous debridement.
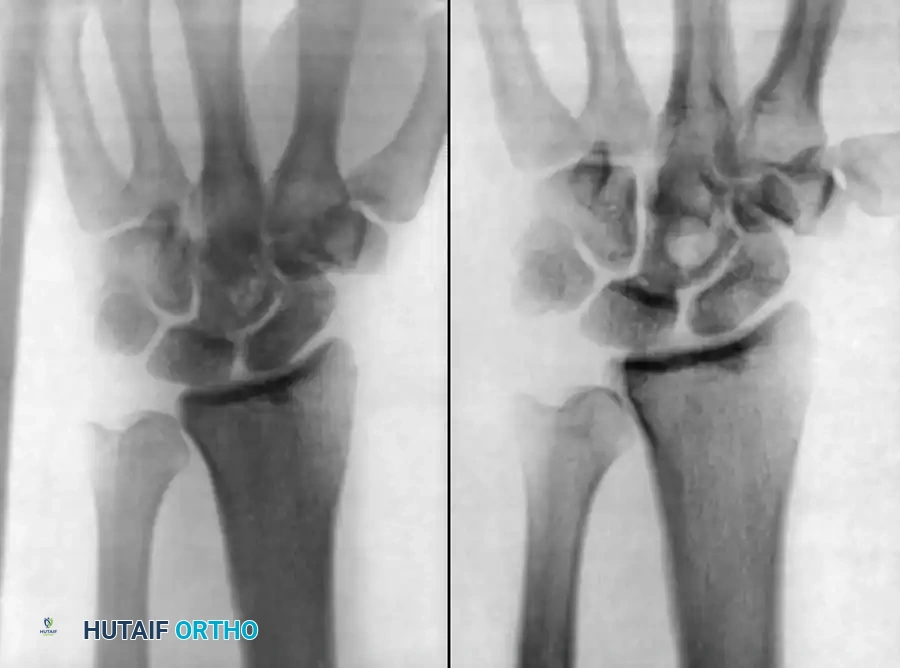
Figure 18-10: Radiographic presentation of recurrent Histoplasmosis in the wrist, demonstrating profound lytic destruction of the carpal rows and distal radius articular surface.
- Approach to the Carpus: For fungal carpal osteomyelitis (as depicted in Figure 18-10), a dorsal longitudinal approach to the wrist is utilized, centered over the Lister tubercle.
- Exposure: The third extensor compartment is opened, and the extensor pollicis longus (EPL) is transposed radially. The second and fourth compartments are elevated subperiosteally to expose the dorsal joint capsule, which is incised longitudinally.
- Radical Carpectomy/Saucerization: Grossly infected, necrotic, and lytic carpal bones are excised completely. In cases of severe histoplasmosis destruction, a proximal row carpectomy or complete carpectomy is often necessary. If the distal radius is involved, the lytic lesions are unroofed (saucerized) with a high-speed burr until healthy, bleeding cancellous bone is reached, eliminating all dead space.
- Staged Reconstruction: Immediate arthrodesis in the presence of active fungal infection is contraindicated. An antibiotic-impregnated cement spacer (loaded with heat-stable antifungals if formulated specifically, though standard practice often relies on systemic therapy) may be placed. Once the fungal burden is definitively cleared via prolonged systemic antifungals (e.g., prolonged itraconazole), a delayed total wrist arthrodesis using a dorsal spanning plate and robust iliac crest autograft is performed.
Complications, Incidence Rates, and Salvage Management
The surgical management of atypical musculoskeletal infections is fraught with potential complications, driven by the compromised state of the local tissues, the chronicity of the disease, and the complex nature of the required reconstructions.
| Complication | Associated Infection | Estimated Incidence | Salvage Management / Mitigation Strategy |
|---|---|---|---|
| Recurrent Infection / Incomplete Eradication | Fungal Osteomyelitis, NTM | 15% - 25% | Requires repeat radical debridement, optimization of systemic antimicrobial/antifungal therapy, and potentially prolonged suppressive therapy. Ensure no dead space remains. |
| Tendon Rupture (Post-operative) | NTM Tenosynovitis | 5% - 10% | Two-stage tendon reconstruction using a silicone Hunter rod, followed by free tendon grafting (e.g., palmaris longus) once the infection is definitively eradicated and soft tissue envelope is stable. |
| Hardware Failure / Nonunion | Syphilitic Charcot Arthropathy | 30% - 50% | Neuropathic bone has virtually no healing potential without massive augmentation. Salvage requires revision to rigid, dual-plate constructs or intramedullary nails, supplemented with massive autogenous bone grafting and prolonged immobilization (often >6 months). |
| Progressive Kyphosis / Cage Subsidence | Brucella Spondylitis | 10% - 15% | Revision surgery involving extension of the posterior instrumentation construct, aggressive posterior column osteotomies (e.g., PSO) to correct sagittal balance, and revision of the anterior structural support. |
| Iatrogenic Nerve Injury | NTM (Median Nerve), Brucella (Nerve Roots) | 2% - 5% | Meticulous microsurgical dissection and intraoperative neuromonitoring are preventative. If transection occurs, immediate primary epineural repair or nerve grafting is indicated. |
Recurrent infection remains the most daunting complication, particularly in fungal osteomyelitis and NTM infections. The avascular nature of the residual scar tissue limits the efficacy of postoperative antibiotics. When recurrence occurs, the surgeon must be prepared to execute even more aggressive debridement. In the appendicular skeleton, if repeated debridements fail to control a fungal or mycobacterial osteomyelitis, or if the resulting bone loss precludes functional reconstruction, definitive salvage via amputation must be considered. Amputation, while drastic, is occasionally the only definitive method to eradicate a life-threatening, disseminated atypical infection and allow the patient to return to functional mobility via prosthetics.
In the context of Syphilitic Charcot arthropathy, the complication of nonunion and hardware failure is exceptionally high. The loss of proprioception and deep pain sensation leads to repetitive microtrauma that overwhelms standard internal fixation. Salvage management for failed arthrodesis in these neuropathic joints requires a paradigm shift: the surgeon must employ "mega-constructs" that span multiple segments, utilizing a combination of robust intramedullary devices and locking plates, coupled with an extended period of strict non-weight-bearing.
Phased Post-Operative Rehabilitation Protocols
Rehabilitation following surgical intervention for atypical infections must be carefully phased, balancing the need to protect complex structural reconstructions with the imperative to prevent debilitating stiffness and adhesions, particularly in the hand and knee.
Phase I: Immediate Post-Operative Period (Weeks 0-2)
The primary goals during this phase are wound healing, edema control, and the initiation of safe, protected motion.
* NTM Hand/Wrist: Following radical tenosynovectomy, the hand is immobilized in a bulky, intrinsic-plus splint for 24 to 48 hours to allow for initial hemostasis. By post-operative day 2 or 3, the splint is removed, and a certified hand therapist initiates early active and active-assisted range of motion protocols. This early motion is absolutely critical to prevent the denuded flexor tendons from adhering to the surrounding soft tissues or the retained annular pulleys.
* Brucella Spine: Patients are mobilized out of bed on post-operative day 1 or 2. A custom-molded Thoracolumbosacral Orthosis (TLSO) is mandatory when out of bed to protect the
