Mastering Orthopaedic Infections and HIV Management in Surgical Practice
Key Takeaway
Effective management of orthopaedic infections demands a synergistic approach of targeted antimicrobial therapy and meticulous surgical debridement. This comprehensive guide details the principles of local antibiotic delivery, dead space management, and the complex orthopaedic manifestations of HIV. It provides evidence-based protocols for treating osteomyelitis and HIV-related myopathies, alongside critical occupational safety measures for the practicing orthopaedic surgeon.
Comprehensive Introduction and Patho-Epidemiology
The treatment of orthopaedic infections, particularly in the context of immunocompromised hosts such as those infected with the Human Immunodeficiency Virus (HIV), represents one of the most intellectually and technically demanding paradigms in modern musculoskeletal medicine. Successful eradication of deep osseous and periprosthetic infections requires a rigorous, dual-pronged approach: highly targeted antimicrobial therapy coordinated with aggressive, often radical, surgical intervention. The modern orthopaedic surgeon must possess a profound understanding of microbiology, pharmacology, and host immune responses to navigate these catastrophic complications. As antimicrobial resistance escalates globally, the reliance on meticulous surgical debridement and innovative local drug delivery systems has never been more paramount.
The pathophysiology of orthopaedic infections is inextricably linked to the formation of bacterial biofilms. When planktonic (free-floating) bacteria adhere to avascular bone, necrotic tissue, or orthopaedic implants, they undergo a phenotypic shift, secreting an extracellular polymeric substance (EPS) composed of polysaccharides, proteins, and extracellular DNA. This glycocalyx creates a formidable physical barrier against both host immune cells and systemic antimicrobial agents. Within the biofilm, bacteria communicate via quorum sensing and enter a sessile, metabolically dormant state. Because most systemic antibiotics target actively dividing cells (e.g., inhibiting cell wall synthesis), these dormant, sessile bacteria can survive antibiotic concentrations up to 1,000 times higher than their planktonic counterparts, mandating physical surgical excision for true eradication.
Concurrently, the global pandemic of HIV and Acquired Immunodeficiency Syndrome (AIDS) profoundly alters the patho-epidemiology of musculoskeletal infections. HIV is an RNA retrovirus that utilizes reverse transcriptase to integrate into the host genome, demonstrating a high tropism for the CD4 surface receptors of T-lymphocytes and macrophages. The subsequent progressive destruction of CD4 cells leads to a profound deregulation of cell-mediated immunity. When the absolute CD4 cell count falls below 200 cells/mm³, the patient crosses the clinical threshold into AIDS, becoming highly susceptible to opportunistic pathogens and atypical presentations of standard orthopaedic infections. Orthopaedic surgeons frequently encounter HIV-positive patients in trauma bays, elective clinics, and operating theaters, necessitating a comprehensive grasp of the virus's impact on healing.
In the HIV-infected population, the incidence and severity of specific musculoskeletal syndromes are markedly amplified. While primary hematogenous osteomyelitis remains relatively rare, osseous infections frequently result from direct extension of adjacent septic joints, neglected soft tissue ulcerations, or open fractures. Furthermore, HIV-positive patients exhibit a higher prevalence of reactive arthritis, idiopathic polymyositis, and pyomyositis—a deep bacterial infection of skeletal muscle almost exclusively caused by Staphylococcus aureus. As the life expectancy of HIV patients has normalized due to Highly Active Antiretroviral Therapy (HAART), surgeons are increasingly performing total joint arthroplasties in this demographic, encountering a significantly elevated risk for late hematogenous periprosthetic joint infections (PJI) as immunosuppression fluctuates.
Detailed Surgical Anatomy and Biomechanics
The microvascular anatomy of bone dictates its susceptibility to infection and its response to surgical debridement. Cortical bone is perfused by a complex network of Haversian systems and Volkmann canals, while the medullary cavity relies on the nutrient artery system. In the presence of acute infection, the localized inflammatory response increases intraosseous pressure, leading to the thrombosis of these delicate microvascular networks. This ischemic cascade results in localized bone death. The devitalized cortical segment, known as a sequestrum, becomes physically separated from the surrounding viable bone and serves as an avascular nidus for relentless biofilm propagation. The periosteum, stimulated by the inflammatory milieu, may form a reactive shell of new bone, termed the involucrum, which can paradoxically encase the infection and hinder the penetration of systemic antibiotics.
From a biomechanical perspective, infected bone and the subsequent surgical debridement create profound structural vulnerabilities. Chronic osteomyelitis induces significant osteolysis, creating stress risers that dramatically reduce the bone's torsional and bending strength, predisposing the patient to pathological fractures. When the surgeon performs an aggressive debridement—unroofing the medullary canal and excising the sequestrum—the resulting cortical defect fundamentally alters the load-bearing capacity of the diaphysis. The management of this resulting "dead space" is not merely a biological imperative to prevent hematoma formation and recurrent infection, but a biomechanical necessity. The surgeon must carefully balance the radical excision required for source control with the preservation of structural integrity, often necessitating the use of external fixation or specialized internal stabilization techniques that bypass the infected zone.
The biomechanics of local antibiotic delivery systems play a critical role in managing this dead space. Polymethyl methacrylate (PMMA) cement, when utilized as a vehicle for local drug delivery, must be carefully formulated. The addition of antibiotic powder to the PMMA monomer-polymer mixture alters its mechanical properties. High doses of antibiotics (e.g., greater than 10% by weight) significantly decrease the compressive and tensile strength of the cement. While this is acceptable for non-structural PMMA beads or temporary spacer blocks, it is a critical consideration if the antibiotic-loaded cement is intended for definitive structural fixation in a revision arthroplasty. Furthermore, the elution kinetics of PMMA are highly dependent on the surface area-to-volume ratio; thus, smaller beads or deeply grooved spacers are biomechanically designed to maximize the release of the impregnated pharmacological agents.
At the cellular level, the pathophysiology of HIV introduces unique biomechanical and structural challenges to the skeletal system. HIV infection and long-term HAART exposure are independently associated with altered bone turnover, characterized by a decoupling of osteoblast and osteoclast activity. The chronic systemic inflammatory state, driven by viral proteins such as Vpr and Tat, upregulates RANKL expression, driving excessive osteoclastogenesis. This results in accelerated bone mineral density loss, osteopenia, and osteoporosis, significantly increasing the risk of fragility fractures. Furthermore, the compromised microvascular environment in HIV-positive patients increases the incidence of avascular necrosis (AVN), particularly of the femoral head, presenting the surgeon with mechanically compromised bone that complicates both internal fixation and arthroplasty procedures.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention in the setting of orthopaedic infections requires a nuanced synthesis of clinical, laboratory, and radiographic data. The primary philosophy of management dictates that surgery is not universally required for all infections; early, uncomplicated acute osteomyelitis in a pediatric patient or a superficial cellulitis may occasionally be completely eradicated with targeted, culture-directed systemic antimicrobial therapy. However, the threshold for surgical intervention is rapidly crossed when medical management fails to yield clinical improvement within 48 to 72 hours. The fundamental purpose of surgery is the mechanical augmentation of the host's immune response: rapidly reducing the bacterial inoculum, dismantling the protective biofilm, and excising the avascular substrate upon which pathogens thrive.
Absolute indications for surgical debridement are well-established in the orthopaedic literature. The presence of gross purulence on joint aspiration (septic arthritis) constitutes a surgical emergency to prevent rapid, irreversible chondrolysis mediated by bacterial metalloproteinases and host lysosomal enzymes. Radiographic or advanced imaging evidence of chronic osteomyelitis—specifically the identification of a sequestrum, a mature involucrum, or an intraosseous abscess (Brodie's abscess)—mandates surgical excision, as systemic antibiotics cannot penetrate these avascular zones. Furthermore, in the setting of periprosthetic joint infection (PJI), surgical intervention is absolute, ranging from Debridement, Antibiotics, and Implant Retention (DAIR) in acute presentations (less than 4 weeks post-op or less than 3 weeks of symptoms) to complex two-stage revision arthroplasty for chronic, mature biofilm infections.
Contraindications to surgical intervention must be carefully weighed, particularly in patients with severe medical comorbidities or advanced immunodeficiency. Absolute contraindications are rare but include patients who are hemodynamically unstable to the point where anesthetic induction poses an imminent threat to life, or those with an entirely un-reconstructable soft tissue envelope where any incision would lead to catastrophic necrosis and amputation is refused. Relative contraindications include profound neutropenia, severe malnutrition (albumin < 3.0 g/dL), or poorly controlled diabetes mellitus (HbA1c > 8.0%), all of which exponentially increase the risk of postoperative wound failure and superinfection. In these scenarios, a period of medical optimization and suppressive antibiotic therapy may be required before definitive surgical debridement can be safely executed.
In the HIV-positive population, surgical indications and contraindications are heavily influenced by the patient's immune status, quantified by the absolute CD4 count and viral load. Elective orthopaedic procedures, such as total joint arthroplasty for AVN or hardware removal, are relatively contraindicated in patients with a CD4 count below 200 cells/mm³ or an unsuppressed viral load, due to the unacceptably high risk of postoperative opportunistic infections and wound dehiscence. Conversely, urgent or emergent procedures—such as the drainage of a pyomyositis abscess, irrigation of a septic joint, or stabilization of an open fracture—must proceed regardless of the CD4 count. In advanced AIDS patients with terminal prognoses and chronic osteomyelitis, aggressive limb salvage may be contraindicated in favor of chronic suppressive antibiotic therapy or palliative amputation to maximize the remaining quality of life.
| Clinical Scenario | Primary Indications for Surgery | Contraindications (Absolute & Relative) | Special Considerations in HIV/AIDS |
|---|---|---|---|
| Acute Septic Arthritis | Purulent aspirate, positive Gram stain, WBC > 50,000 in native joint, failure of 24h medical therapy. | Absolute: Hemodynamic instability precluding anesthesia. Relative: Severe coagulopathy. |
Emergent surgery required regardless of CD4 count. High suspicion for atypical organisms. |
| Chronic Osteomyelitis | Radiographic sequestrum, draining sinus tract, intractable pain, pathological fracture risk. | Absolute: Un-reconstructable soft tissue (requires amputation). Relative: Severe malnutrition, profound immunosuppression. |
Optimize HAART pre-operatively. Avoid massive structural allografts if CD4 < 200. |
| Periprosthetic Joint Infection | Sinus tract communicating with prosthesis, positive deep cultures, elevated synovial alpha-defensin. | Absolute: Patient medically unfit for major revision surgery. Relative: Lack of available bone stock for reconstruction. |
Higher failure rates of 2-stage revisions in advanced AIDS. Consider suppressive therapy. |
| Pyomyositis | Loculated intramuscular abscess on MRI/Ultrasound, failure of percutaneous aspiration. | Relative: Diffuse, early-stage myositis without discrete abscess formation (treat medically). | Extremely common in HIV. Often multiple/bilateral. Requires broad-spectrum IV coverage. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for orthopaedic infections demands a meticulous, multidisciplinary approach, integrating the expertise of orthopaedic surgeons, infectious disease specialists, and plastic surgeons. The foundation of this phase relies on accurate diagnostics. If the patient is hemodynamically stable and not exhibiting signs of systemic sepsis, it is a cardinal rule of orthopaedic oncology and infection management to withhold empiric systemic antibiotics until deep, representative intraoperative tissue cultures are obtained. Premature administration of antibiotics frequently sterilizes the local tissue cultures, rendering the infectious disease team unable to determine the Minimum Inhibitory Concentration (MIC) and Serum Bactericidal Concentration (SBC), thereby forcing the prolonged use of broad-spectrum, highly toxic empiric regimens.
Advanced imaging is non-negotiable for precise surgical templating. Standard orthogonal radiographs are utilized to assess for hardware loosening, periosteal reactions, and gross osteolysis, but they lack the sensitivity required for soft tissue and intramedullary mapping. Magnetic Resonance Imaging (MRI) with intravenous gadolinium contrast is the gold standard; it delineates the extent of osseous necrosis, identifies skip lesions within the medullary canal, and maps complex soft tissue abscesses and sinus tracts via rim enhancement. In cases where MRI is contraindicated (e.g., incompatible pacemakers or severe retained hardware artifact), Computed Tomography (CT) with contrast is essential for identifying cortical sequestra and planning the precise osteotomies required for unroofing the infected bone. Nuclear medicine modalities, such as Indium-111 labeled white blood cell scans combined with Technetium-99m sulfur colloid marrow scans, are reserved for diagnosing PJI in the setting of complex hardware where standard imaging is equivocal.
For the HIV-positive patient, pre-operative planning includes rigorous serological and immunological staging. The surgeon must understand the "Window Period"—the critical phase immediately following viral transmission where the patient is highly infectious but has not yet produced detectable antibodies, potentially yielding a false-negative ELISA. Confirmatory testing via Western Blot or Nucleic Acid Testing (NAT) is essential. Pre-operative laboratory workup must include a current absolute CD4 count, HIV viral load, complete blood count (to assess for AZT-induced leukopenia or anemia), and a comprehensive metabolic panel to evaluate renal and hepatic function, which may be compromised by long-term HAART or the impending use of nephrotoxic antibiotics like vancomycin and aminoglycosides.
Patient positioning and operating room setup must facilitate extensile surgical approaches and strict adherence to universal precautions. The patient should be positioned on a radiolucent table to allow for unrestricted intraoperative fluoroscopy. While a pneumatic tourniquet may be applied to the extremity to minimize blood loss during the initial exposure and soft tissue dissection, it is an absolute technical requirement to deflate the tourniquet prior to the final osseous debridement. The surgeon must be able to visualize punctate cortical bleeding—the "paprika sign"—to accurately differentiate between viable, vascularized bone and necrotic tissue requiring further excision. Furthermore, the surgical team must employ rigorous occupational risk prevention strategies: mandatory double-gloving to reduce viral inoculum during accidental percutaneous injuries, the use of impervious surgical gowns, full-coverage surgical helmets or protective eyewear to prevent conjunctival splashing, and the strict use of a neutral zone for passing sharp instruments.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of osteomyelitis debridement and infection eradication is predicated on the principles of oncologic resection. The approach begins with an extensile incision that incorporates and elliptically excises all previous traumatic scars and draining sinus tracts. Sinus tracts are lined with a dense, fibrotic, and heavily infected pseudomembrane that must be removed entirely to prevent recurrence. The soft tissue dissection proceeds systematically, radically excising all necrotic, fibrotic, and poorly perfused fascia and muscle. The surgeon must rely on visual and tactile feedback: healthy muscle should appear beefy red, bleed briskly when incised, and contract when stimulated by electrocautery. Any tissue that is gray, friable, or avascular must be aggressively debrided back to bleeding margins, regardless of the resulting soft tissue defect.
Osseous debridement is the most critical phase of the procedure. Utilizing high-speed burrs, rongeurs, and sharp osteotomes, the surgeon must unroof the medullary canal, creating a cortical window large enough to access the entire extent of the intramedullary infection. All sequestra must be meticulously extracted. The debridement of the cortical and cancellous bone continues until the "paprika sign" is achieved—a diffuse, punctate bleeding from the Haversian canals indicating healthy, vascularized bone. In chronic cases, the intramedullary canal must be reamed or burred until the sclerotic, avascular inner cortex is removed, exposing viable marrow elements. Once the mechanical debridement is complete, the surgical field is subjected to copious irrigation. Low-pressure pulsatile lavage or gravity flow with 6 to 9 liters of normal saline is utilized to mechanically wash away planktonic bacteria, residual bone dust, and microscopic debris.
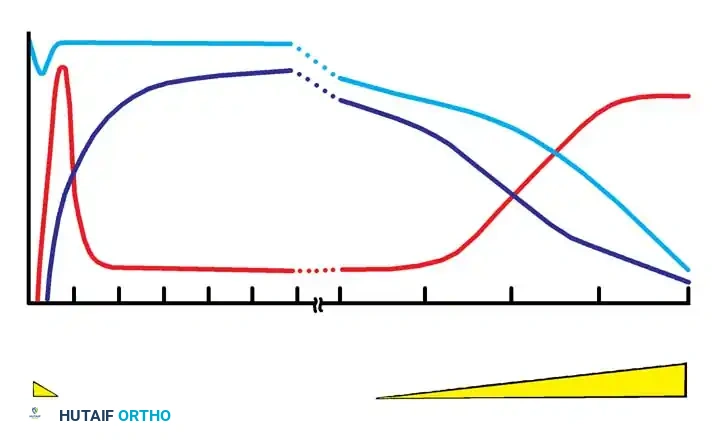
Following radical debridement, the surgeon is faced with the management of the resulting dead space. Systemic intravenous antibiotics exhibit notoriously poor penetration into the ischemic, fibrotic environment of an orthopaedic infection bed. Therefore, local antibiotic delivery systems are deployed to bridge this gap, providing supratherapeutic local tissue concentrations while minimizing systemic toxicity. Polymethyl methacrylate (PMMA) cement, impregnated with heat-stable antibiotics (typically tobramycin, vancomycin, or gentamicin), is the historical gold standard. The PMMA is molded into chains of beads on a non-absorbable suture or fashioned into structural spacer blocks. These systems create a 2- to 3-cm zone of high antimicrobial concentration, with peak elution occurring within the first 48 hours. Alternatively, biodegradable systems such as collagen-gentamicin sponges or calcium sulfate pellets can be utilized. These eliminate the need for a secondary surgical procedure to remove the PMMA, though their elution profiles are significantly more rapid.
The final stage of the surgical technique involves osseous stabilization and soft tissue coverage. Radical debridement often compromises the structural integrity of the bone, necessitating stabilization to prevent pathological fracture and facilitate soft tissue healing. In the presence of active infection, internal fixation (plates and intramedullary nails) is generally avoided due to the risk of biofilm colonization on the new implants. Instead, multiplanar external fixation (e.g., Ilizarov or Taylor Spatial Frames) is heavily favored, as it provides rigid stabilization while keeping the hardware distant from the infected zone. If a massive segmental bone defect is created, the surgeon may employ the induced membrane technique (Masquelet technique), placing a PMMA cement spacer in the defect to induce a vascularized pseudomembrane, followed 6 to 8 weeks later by spacer removal and massive autologous cancellous bone grafting. Immediate, durable soft tissue coverage, often requiring rotational or free vascularized muscle flaps performed in conjunction with plastic surgery, is mandatory to seal the debrided bed and provide a robust blood supply for eradication.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and targeted antimicrobial therapy, the treatment of orthopaedic infections is fraught with high complication rates and frequent recurrences. The most devastating complication is the persistence or recurrence of the infection, driven by residual microscopic biofilm or inadequate excision of necrotic bone. In the surgical management of chronic osteomyelitis, recurrence rates can range from 10% to 30%, depending on the host's physiological status (Cierny-Mader classification) and the virulence of the pathogen. Periprosthetic joint infections treated with two-stage revision arthroplasty carry a failure rate of approximately 10% to 15%, often necessitating a third or fourth stage, or ultimately leading to resection arthroplasty (Girdlestone procedure) or arthrodesis.
Systemic complications arising from the prolonged medical management of these infections are equally severe. The administration of high-dose, prolonged intravenous antibiotics—particularly aminoglycosides and glycopeptides—carries a significant risk of systemic toxicity. Acute kidney injury (nephrotoxicity) and irreversible hearing loss or vestibular dysfunction (ototoxicity) are well-documented risks, necessitating rigorous therapeutic drug monitoring and trough level assessments. Furthermore, the local elution of massive doses of antibiotics from PMMA spacers or calcium sulfate beads can occasionally lead to systemic absorption sufficient to cause acute renal failure, particularly in patients with pre-existing renal impairment or those concurrently receiving nephrotoxic HAART regimens.
In the HIV-positive surgical patient, complications are amplified by the underlying immunodeficiency and the pharmacological side effects of antiretroviral therapy. Delayed wound healing, wound dehiscence, and secondary opportunistic superinfections are significantly more common in patients with CD4 counts below 200 cells/mm³. Furthermore, orthopaedic surgeons must be vigilant in differentiating postoperative complications from HIV-specific musculoskeletal syndromes. For instance, a patient presenting with profound proximal muscle weakness and elevated creatine phosphokinase (CPK) postoperatively may be experiencing idiopathic polymyositis or Zidovudine (AZT) toxicity, both of which are clinically and histologically indistinguishable but require vastly different management (immunosuppression vs. cessation of the offending retroviral agent).
When repeated surgical debridements and targeted antimicrobial therapies fail, the surgeon must pivot to salvage management strategies to preserve the patient's life and overall function. Chronic suppressive antibiotic therapy—the indefinite administration of oral antibiotics—may be employed in patients who are medically unfit for further surgery or who refuse amputation, provided the pathogen is highly susceptible to an oral agent and the patient can tolerate the long-term side effects. However, when the infection threatens life via recurrent sepsis, or when the limb becomes a painful, non-functional burden due to massive bone loss and soft tissue destruction, amputation becomes the definitive salvage procedure. The level of amputation must be carefully planned to ensure excision of all infected tissue while maximizing the potential for prosthetic rehabilitation.
| Complication Category | Specific Complication | Estimated Incidence | Salvage / Management Strategy |
|---|---|---|---|
| Infectious | Recurrent Osteomyelitis / Biofilm Persistence | 10% - 30% | Repeat radical debridement, transition to biodegradable local delivery, consider amputation if soft tissue envelope is exhausted. |
| Systemic Medical | Aminoglycoside/Vancomycin Nephrotoxicity | 5% - 15% | Immediate cessation of offending agent, aggressive IV hydration, transition to alternative antibiotic class (e.g., Linezolid, Daptomycin). |
| Biomechanical | Pathological Fracture through Debridement Site | 2% - 8% | Application of multiplanar external fixation, initiation of bone transport (Ilizarov) or Masquelet technique for segmental defects. |
| HIV-Specific | HAART-Induced Myopathy (AZT Toxicity) | Variable | Differentiate from pyomyositis via MRI/biopsy. Trial cessation of AZT; symptoms typically resolve rapidly upon withdrawal. |
Phased Post-Operative Rehabilitation Protocols
The post-operative rehabilitation following the surgical management of orthopaedic infections is a protracted, highly phased process that requires continuous coordination between the orthopaedic surgeon, infectious disease team, and physical therapists. Phase I (Acute Post-Operative Phase, Weeks 0-2) is heavily focused on wound healing, dead space management, and the initiation of targeted systemic antimicrobial therapy. Following radical debridement, the surgical incisions are often under significant tension or may be left open for delayed primary closure. Negative Pressure Wound Therapy (NPWT) is frequently employed to manage exudate, promote angiogenesis, and reduce the physical dimensions of the soft tissue defect. During this phase, the patient remains non-weight-bearing on the affected extremity. Deep tissue cultures obtained intraoperatively dictate the transition from empiric to directed intravenous antibiotics, with dosing meticulously calibrated to exceed the Minimum Inhibitory Concentration (MIC) for the specific pathogen.
Phase II (Subacute Healing Phase, Weeks 2-6) marks the critical period of soft tissue consolidation and the peak elution phase of local antibiotic delivery systems. If non-biodegradable PMMA beads were utilized for dead space management, a secondary surgical procedure is typically scheduled within 2 to 4 weeks for their removal, prior to their encapsulation by a dense fibrous membrane or colonization by secondary, resistant pathogens. Following bead removal, the dead space may be grafted with autologous cancellous bone (often harvested from the iliac crest and mixed with antibiotic powder) to promote osteoconduction and structural stability. Physical therapy in this phase focuses on maintaining adjacent joint range of motion and preventing contractures, particularly if external fixation devices are in place. Weight-bearing status remains highly restricted, dependent on the structural integrity of the remaining cortical bone and the type of stabilization employed.
Phase III (Reconstruction and Strengthening, Weeks 6-12) involves the transition from intravenous to oral antimicrobial therapy, provided the patient demonstrates a robust clinical response, normalizing inflammatory markers (ESR and CRP), and the identified pathogen is susceptible to a highly bioavailable oral agent (e.g., fluoroquinolones, rifampin combinations). Radiographic surveillance is critical during this phase to assess for the incorporation of bone grafts, the progression of bone transport in Ilizarov reconstructions, or the integration of revision arthroplasty components. Weight-bearing is progressively advanced based on radiographic evidence of osseous union and structural stability. In patients undergoing the Masquelet technique, this phase corresponds with the maturation of the induced pseudomembrane and the subsequent massive bone grafting procedure.
Long-term surveillance (Months 3 to Years) is the final, indefinite phase of rehabilitation. Orthopaedic infections are notorious for their latency; bacteria can remain dormant within osteoblastic lacunae or sequestered micro-abscesses for decades before reactivating. Patients are monitored with serial clinical examinations and inflammatory markers at regular intervals. For the HIV-positive patient, this long-term phase requires rigorous medical adherence to HAART. The orthopaedic surgeon must work closely with the patient's primary infectious disease physician to ensure that CD4 counts remain elevated (>200 cells/mm³) and viral loads remain suppressed. Fluctuations in immune status significantly increase the risk of late hematogenous seeding of previously treated surgical sites or retained orthopaedic implants, demanding lifelong vigilance and rapid intervention at the first sign of recurrent localized pain or systemic inflammation.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management of orthopaedic infections is built upon a foundation of landmark literature and rigorously developed clinical guidelines. The Cierny-Mader classification system, introduced in the 1980s, remains the definitive framework for categorizing osteomyelitis and guiding surgical strategy. Unlike traditional classifications based solely on etiology or chronicity, the Cierny-Mader system uniquely incorporates the anatomic extent of the infection (Medullary, Superficial, Localized, or Diffuse) and, critically, the physiological status of the host (A-host: healthy; B-host: compromised locally or systemically; C-host: treatment worse than the disease). This classification underscores the modern principle that radical surgical debridement is mandatory for localized and diffuse anatomic types, but may be contraindicated in the C-host, where suppressive therapy is favored.
In the realm of Periprosthetic Joint Infection (PJI), the diagnostic criteria established by the Musculoskeletal Infection Society (MSIS) and subsequently refined by the International Consensus Meeting (ICM) on PJI represent the gold standard for clinical diagnosis. These guidelines synthesized decades of literature to create a definitive algorithm, moving away from subjective clinical gestalt to objective, measurable parameters. The criteria define absolute indicators of infection (e.g., two positive periprosthetic cultures with phenotypically identical organisms, or a sinus tract communicating with the joint) and minor criteria (elevated synovial fluid WBC count, elevated synovial polymorphonuclear percentage, elevated serum CRP/ESR, and positive histological analysis of periprosthetic tissue). The integration of novel biomarkers, such as synovial alpha-defensin, into these guidelines has further revolutionized the accuracy of preoperative PJI diagnosis.
The literature surrounding local antibiotic delivery systems has evolved significantly since the pioneering work of Klemm and Ostermann, who first popularized the use of gentamicin-impregnated PMMA beads. Modern literature has heavily investigated the pharmacokinetics of biodegradable carriers. Studies have demonstrated that calcium sulfate and collagen-based sponges can deliver peak local antibiotic concentrations that are orders of magnitude higher than systemic administration, effectively eradicating biofilm-embedded organisms without the need for a secondary removal surgery. However, clinical guidelines emphasize the "Surgical Warning" associated with these systems: surgeons must be acutely aware of the local cytotoxicity of massive antibiotic doses, which can impair osteoblast function, inhibit
