PRINCIPLES OF ORTHOPAEDIC INFECTION MANAGEMENT
The treatment of orthopaedic infections represents one of the most challenging paradigms in musculoskeletal medicine. Successful eradication requires a dual-pronged approach: targeted antimicrobial therapy and aggressive surgical intervention. While antibiotic therapy alone may occasionally suffice in early, uncomplicated cases, the presence of avascular bone, necrotic tissue, and bacterial biofilm typically mandates surgical debridement.
Antimicrobial Therapy Fundamentals
The foundation of medical management relies on the accurate identification of the offending organism and the determination of its antimicrobial susceptibility.
- Bactericidal vs. Bacteriostatic: Bactericidal agents are strongly preferred over bacteriostatic agents, particularly in the presence of retained hardware or compromised host immunity.
- MIC and SBC: The chosen antibiotic must be dosed to achieve local tissue concentrations that exceed the Minimum Inhibitory Concentration (MIC) and ideally the Serum Bactericidal Concentration (SBC) for the specific pathogen.
- Empiric vs. Directed Therapy: If the patient is hemodynamically stable, antibiotics should be withheld until deep intraoperative cultures are obtained. If empiric therapy is initiated, it must be tailored once sensitivities are reported (typically within 48 to 72 hours). Failure to respond to appropriate antibiotic therapy within 36 to 48 hours strongly suggests either an incorrect antibiotic spectrum, the development of a localized abscess, or the presence of a mature biofilm requiring surgical excision.
Clinical Pearl: Surgery can accomplish in one hour what the host immune system and intravenous antibiotics may require weeks to achieve. The primary purpose of surgical intervention is the mechanical augmentation of the host response by reducing the bacterial inoculum and excising the avascular substrate upon which biofilm propagates.
SURGICAL MANAGEMENT OF OSTEOMYELITIS
Surgery is not universally required for all infections, but it becomes absolute in the presence of purulence on aspiration, radiographic evidence of chronic osteomyelitis (e.g., sequestrum, involucrum), or failure of medical management.
Preoperative Planning and Positioning
- Imaging: Advanced imaging (MRI with contrast or CT) is essential to delineate the extent of osseous necrosis, soft tissue abscesses, and sinus tracts.
- Positioning: The patient must be positioned to allow for an extensile approach. A tourniquet may be applied to minimize blood loss but should be deflated prior to final debridement to accurately assess bone viability (the "paprika sign").
Step-by-Step Surgical Debridement
- Incision and Approach: Utilize an extensile exposure. Excise all previous sinus tracts elliptically, as these are lined with infected, necrotic tissue.
- Soft Tissue Debridement: Radically excise all necrotic, fibrotic, and poorly perfused soft tissue. Healthy muscle should bleed and contract when stimulated.
- Osseous Debridement: Use a high-speed burr or osteotomes to unroof the medullary canal. Remove all sequestra (dead bone). Continue debridement until punctate cortical bleeding is observed (the paprika sign), indicating viable, vascularized bone.
- Irrigation: Perform copious irrigation using low-pressure pulsatile lavage or gravity flow with normal saline to mechanically wash away planktonic bacteria and residual debris.
LOCAL ANTIBIOTIC DELIVERY SYSTEMS
Systemic intravenous (IV) antibiotics are standard for serious infections, but achieving therapeutic concentrations in ischemic, infected bone is notoriously difficult. Local antibiotic delivery systems bridge this gap, providing supratherapeutic local concentrations while minimizing systemic toxicity.
Polymethyl Methacrylate (PMMA) Beads
Since the 1970s, PMMA cement impregnated with heat-stable antibiotics has been the gold standard for dead space management and local drug delivery.
* Antibiotic Selection: Only heat-stable antibiotics in powder form can be used, as the exothermic reaction of curing PMMA destroys heat-labile drugs. Tobramycin, vancomycin, and gentamicin are the most commonly utilized agents.
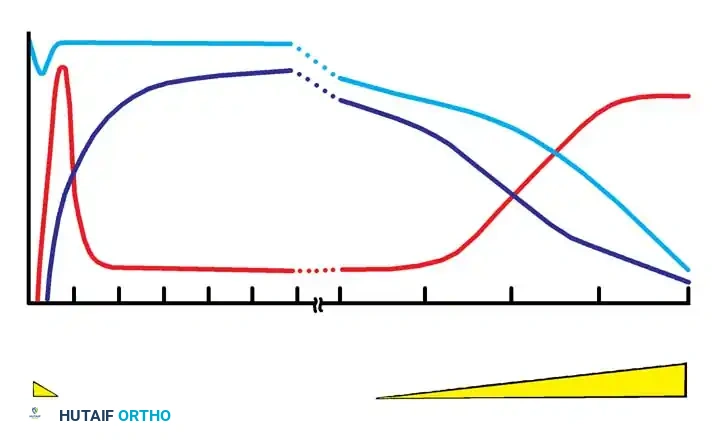
* Elution Kinetics: PMMA beads create a 2- to 3-cm zone of high antibiotic concentration. Peak elution occurs within the first 24 to 48 hours and rapidly declines, maintaining therapeutic local levels for approximately one to two weeks.
* Drawbacks: PMMA is non-biodegradable and acts as a foreign body once the antibiotic has eluted. It requires a secondary surgical procedure for removal, typically within 2 to 4 weeks, before it becomes encapsulated by a fibrous membrane or colonized by secondary pathogens.
Biodegradable Delivery Systems
To circumvent the need for secondary removal surgeries, biodegradable systems have been developed:
* Collagen-Gentamicin Sponges: These sponges deliver higher peak concentrations of antibiotics than PMMA beads and do not require surgical removal. However, their elution profile is extremely rapid, with complete antibiotic release often occurring within 4 days.
* Lactic Acid Polymerase: An emerging technology that delivers high concentrations of quinolones (highly effective against chronic osteomyelitis pathogens). This system provides a sustained release for up to 60 days, with a peak release at day 15.
* Antibiotic-Impregnated Bone Graft: Mixing autogenous iliac crest bone graft with piperacillin or vancomycin provides both local antimicrobial therapy and osteoconductive/osteoinductive properties for bone defect reconstruction. Complications are rare, with localized rash being the most frequently reported adverse event.
Surgical Warning: When mixing antibiotics with bone graft, ensure the chosen antibiotic does not exhibit severe local cytotoxicity that could impair osteoblast function and subsequent graft incorporation.
HUMAN IMMUNODEFICIENCY VIRUS (HIV) IN ORTHOPAEDICS
The global pandemic of HIV and Acquired Immunodeficiency Syndrome (AIDS) profoundly impacts orthopaedic surgery. Orthopaedic surgeons frequently encounter HIV-positive patients in trauma bays, clinics, and operating theaters. A comprehensive understanding of the virus's pathophysiology, musculoskeletal manifestations, and occupational risks is mandatory.
Pathophysiology and Clinical Stages
HIV is a human RNA retrovirus. It utilizes the enzyme reverse transcriptase to convert its viral RNA into DNA, which is then integrated into the host's genome. The virus is highly trophic for the CD4 surface receptors of T-lymphocytes.
The infection triggers a progressive deregulation and destruction of CD4 T-lymphocytes, leading to a profound immunodeficient state. When the absolute CD4 cell count falls below 200/mm³, the patient is highly susceptible to opportunistic infections (e.g., Pneumocystis carinii pneumonia, Kaposi sarcoma), marking the clinical onset of AIDS.
The clinical progression of HIV is categorized into four distinct stages:
1. Acute Primary HIV Infection: Occurs 2 to 6 weeks post-transmission. Clinically mimics infectious mononucleosis (fever, lymphadenopathy, pharyngitis, rash, leukopenia). It is self-limiting.
2. Chronic Asymptomatic Infection: A prolonged latent period lasting 5 to 15+ years. Viral replication continues, and CD4 counts slowly decline.
3. Symptomatic HIV Infection (AIDS-Related Complex): Patients develop constitutional symptoms but have not yet met the CDC criteria for AIDS (CD4 remains > 200/mm³).
4. Advanced HIV-Associated Disease (AIDS): Severe cell-mediated immunodeficiency characterized by life-threatening opportunistic infections and malignancies.
Diagnostic Modalities and the "Window Period"
Serological testing relies on the detection of host antibodies against the virus.
* The Window Period: There is a critical period immediately following infection during which the patient is highly infectious but has not yet produced detectable antibodies. Relying on a single test during this phase can yield a false-negative result.
* ELISA (Enzyme-Linked Immunosorbent Assay): The standard screening test. It is highly sensitive (>99% after 3 months of infection) but prone to false positives.
* Western Blot: The confirmatory test used if the ELISA is reactive. It is highly specific. The probability of a false-positive result with a combined ELISA and Western blot sequence is approximately 1 in 350,000.
* CD4 Count: Not a diagnostic test for the presence of the virus, but a critical biomarker for quantifying the degree of immunosuppression and guiding surgical risk stratification.
MUSCULOSKELETAL SYNDROMES IN HIV-INFECTED PATIENTS
HIV infection can alter the clinical presentation, severity, and natural history of standard musculoskeletal pathologies. Early diagnosis is paramount to prevent rapid dissemination in the immunocompromised host.
Reactive and Septic Arthritis
- Reactive Arthritis: Frequently presents in the lower extremities, particularly the foot and ankle. It is often accompanied by severe tendinitis of the Achilles, anterior tibial, or posterior tibial tendons.
- Septic Arthritis: More prevalent in HIV patients with concurrent risk factors, such as intravenous drug use or hemophilia. Despite the immunocompromised state, the most common causative organisms remain typical Gram-positive bacteria (Staphylococcus aureus and Streptococcus pneumoniae).
Osteomyelitis and Prosthetic Joint Infection
Primary hematogenous osteomyelitis is relatively rare in HIV patients; osseous infection usually results from direct extension from an adjacent septic joint or soft tissue ulceration. However, as immunosuppression progresses (CD4 < 200/mm³), patients with total joint arthroplasties are at a significantly elevated risk for late hematogenous periprosthetic joint infections (PJI).
Myopathies and Muscle Pain
Muscle pain is a ubiquitous complaint in the HIV-positive population and requires careful differentiation:
1. Idiopathic Polymyositis: An autoimmune-like inflammatory myopathy presenting with proximal muscle weakness, elevated creatine phosphokinase (CPK), and myofibril necrosis on biopsy.
2. Zidovudine (AZT) Toxicity: Clinically and histologically indistinguishable from idiopathic polymyositis. Diagnosis relies on a trial of medication cessation, which typically resolves the myopathy.
3. Pyomyositis: A deep bacterial infection of the skeletal muscle, almost exclusively caused by S. aureus. It presents as localized muscle pain, swelling, erythema, and fever. It may manifest as a solitary abscess or multiple intramuscular abscesses.
* Treatment: Broad-spectrum IV antibiotics and ultrasound- or CT-guided aspiration are first-line therapies. Formal surgical incision and drainage are indicated for large, loculated abscesses or failure of percutaneous management.
OCCUPATIONAL RISKS AND PREVENTION IN ORTHOPAEDIC SURGERY
The transmission of HIV occurs via sexual, parenteral, and maternal-infant routes. The virus has been isolated from blood, semen, vaginal secretions, breast milk, and bone.
Transmission via Allograft and Transfusion
Historically, the transmission of HIV through musculoskeletal allografts was a significant concern, with documented cases in 1984 and 1985. However, with the advent of rigorous donor screening and advanced nucleic acid testing (NAT), no further transmissions via orthopaedic allografts have been reported since 1985. The risk of HIV transmission per unit of transfused allogenic blood is currently estimated at 1 in 153,000, prompting a paradigm shift toward blood conservation strategies and autologous transfusions in elective orthopaedic surgery.
Occupational Risk to the Surgeon
Orthopaedic surgery, particularly trauma surgery, involves frequent exposure to blood, bone spicules, and sharp instruments, placing the surgeon at theoretical risk for occupational transmission.
* Prevalence: While the general U.S. population prevalence of HIV is approximately 0.5%, the prevalence in urban Level I trauma centers can approach 10%. Alarmingly, up to 30% of HIV-infected patients are unrecognized at the time of acute surgical treatment.
* Needlestick Risk: The risk of seroconversion following a percutaneous exposure (needlestick) to HIV-infected blood is approximately 0.3%.
* Prevention Strategies: Universal precautions are mandatory. Orthopaedic surgeons must employ double-gloving (which significantly reduces the viral inoculum in the event of a puncture), utilize blunt-tipped needles for fascial and muscle closure, wear impervious surgical gowns, and use protective eyewear or surgical helmets to prevent conjunctival splashing.
Surgical Pearl: The calculation of occupational risk depends on three variables: the frequency of percutaneous injuries, the prevalence of HIV in the specific patient population, and the transmission rate per exposure. Meticulous surgical technique, passing sharps in a neutral zone, and strict adherence to universal precautions remain the most effective methods for protecting the surgical team.
