INTRODUCTION AND EPIDEMIOLOGY
Traumatic dislocations of the knee are relatively uncommon, representing less than 0.2% of all orthopedic injuries. However, their true incidence is likely underestimated because many knee dislocations spontaneously reduce prior to medical evaluation. These are true orthopedic emergencies, carrying a high risk of limb-threatening vascular compromise and debilitating neurological deficits.
In an acutely dislocated knee, the diagnosis is usually obvious due to gross deformity, severe pain, and massive swelling. However, the diagnosis becomes significantly more difficult in obese patients, in those whose knees have spontaneously reduced, and in polytrauma patients where distracting injuries may mask the knee pathology. Failure to correctly diagnose a spontaneously reduced knee dislocation diminishes the likelihood of recognizing an associated injury to the popliteal artery, which can result in devastating complications, including ischemic contracture or above-knee amputation.
Velocity and Mechanism of Injury
Historically, knee dislocations were categorized primarily as high-velocity injuries (e.g., motor vehicle accidents, industrial trauma). However, modern literature recognizes distinct prognostic categories based on the energy of the trauma:
- High-Velocity Injuries: Typically result from high-energy trauma. These are associated with a higher incidence of open fractures, severe soft-tissue degloving, and concomitant systemic injuries.
- Low-Velocity Injuries: Often occur during athletic activities. Shelbourne et al. reported on low-velocity dislocations, noting that vascular injury occurred in only 4.8% of cases, meniscal damage in 20%, and osteochondral fractures in 5%. Patients sustaining low-velocity injuries generally have a superior prognosis following aggressive rehabilitation and ligamentous reconstruction.
- Ultralow-Velocity Injuries: A distinct subset identified in morbidly obese patients (Body Mass Index [BMI] > 30, often > 40). These occur during activities of daily living, such as stepping off a curb or a simple ground-level fall. The massive kinetic energy generated by the patient's body weight acting on a fixed tibia results in catastrophic multi-ligamentous failure.
Clinical Pearl: There is a direct correlation between BMI and the severity of neurovascular injury in ultralow-velocity dislocations. In one series, patients with nerve injuries had an average BMI of 48.3; those with vascular injuries averaged 56.3; and those with combined neurovascular injuries averaged 60.3.
CLASSIFICATION SYSTEMS
Classification of knee dislocations is essential for standardizing communication, guiding preoperative planning, and determining the timing of surgical intervention.
Directional Classification (Kennedy)
This historical classification is based on the position of the tibia relative to the femur at the time of injury:
1. Anterior (Most Common): Typically caused by hyperextension. High risk of intimal tear to the popliteal artery due to traction.
2. Posterior: Usually results from a direct blow to the proximal tibia with the knee flexed (e.g., dashboard injury). High risk of complete popliteal artery transection.
3. Medial / Lateral: Caused by severe varus or valgus forces.
4. Rotatory: Often irreducible due to soft-tissue interposition (e.g., posterolateral dislocation with the medial femoral condyle buttonholed through the medial capsule).
Anatomic/Structural Classification (Schenck)
Modern classification focuses on the specific ligamentous structures disrupted, which directly dictates the surgical reconstructive plan:
* KD-I: Single cruciate injury (ACL or PCL) with collateral ligament disruption.
* KD-II: Both ACL and PCL torn, collaterals intact.
* KD-III: Both ACL and PCL torn, plus one collateral ligament (KD-IIIM for medial, KD-IIIL for lateral).
* KD-IV: Pan-ligamentous injury (ACL, PCL, MCL, and LCL/PLC all torn).
* KD-V: Multi-ligamentous injury associated with a periarticular fracture.
CLINICAL AND RADIOGRAPHIC EVALUATION
The Neurovascular Examination
Completion and meticulous documentation of a thorough neurovascular examination are mandatory at the time of initial evaluation, immediately following any reduction maneuver, and serially thereafter.
The extremity must be examined for color, temperature, and capillary refill. Posterior tibial and dorsalis pedis pulses must be palpated and compared with the contralateral side.
Surgical Warning: The presence of palpable pulses does NOT rule out a devastating popliteal artery injury. An intimal tear may allow sufficient initial blood flow to maintain a pulse, only to thrombose hours later, leading to irreversible ischemia.
The Ankle-Brachial Index (ABI) is a critical screening tool. The ABI is calculated by dividing the systolic pressure in the injured ankle by the systolic pressure in the uninjured arm.
* ABI > 0.90: High negative predictive value (100% in some prospective studies). Warrants close serial observation.
* ABI < 0.90: Indicates abnormal flow and mandates immediate further vascular imaging (CT angiography or conventional arteriography).
Nerve damage occurs in approximately 20% of knee dislocations, most commonly affecting the common peroneal nerve. Nearly half of these injuries result in a permanent neurological deficit. The risk of peroneal nerve palsy approaches 45% in dislocations involving disruption of the posterolateral corner (PLC) and PCL.
Radiographic Evaluation
Initial radiographic evaluation focuses on determining the direction of the dislocation, confirming reduction, and identifying concomitant bony injuries (e.g., Segond fractures, fibular head avulsions, or tibial plateau fractures). Anteroposterior (AP), lateral, and oblique views are mandatory.

Fig. 43-147 A: Lateral radiograph demonstrating a gross traumatic knee dislocation with posterior displacement of the tibia.

Fig. 43-147 B: Anteroposterior (AP) radiograph of the same traumatic knee dislocation.
Advanced Imaging
Magnetic Resonance Imaging (MRI): MRI is the gold standard for evaluating soft-tissue injuries. It precisely identifies the location of cruciate tears (midsubstance vs. avulsion), collateral ligament disruptions, meniscal pathology, and the status of the popliteus tendon.
* ACL Tears: 45% midsubstance, 34% femoral avulsions, 21% tibial avulsions.
* PCL Tears: 76% femoral avulsions, 17% midsubstance, 7% tibial avulsions.
Arteriography: Femoral arteriography or CT Angiography is indicated for any patient with questionable circulation, an ABI < 0.90, or absent peripheral pulses before or after reduction.

Fig. 43-148: Femoral arteriogram in a patient with a knee dislocation, demonstrating abrupt occlusion of the popliteal artery requiring emergent vascular bypass.
INITIAL MANAGEMENT AND REDUCTION
The first priority is the vascular status of the extremity, not the ligaments. If peripheral circulation is deficient, the dislocation must be reduced immediately in the trauma bay.
Closed Reduction Technique
- Administer adequate procedural sedation and analgesia.
- Apply longitudinal traction to the tibia.
- Translate the tibia anteriorly or posteriorly depending on the direction of the dislocation. Avoid excessive hyperextension, which can further stretch the popliteal artery.
- Reassess neurovascular status immediately post-reduction.
- Immobilize the knee in a posterior plaster splint or hinged knee brace at 30 to 45 degrees of flexion. This position relaxes the posterior capsule, the popliteal vessels, and the posterolateral/posteromedial structures.
Pitfall: Avoid circumferential casting in the acute setting. Massive swelling is expected, and a circumferential cast obscures the ability to monitor for compartment syndrome and vascular compromise.
Indications for Emergent Surgical Intervention
While ligamentous reconstruction is typically delayed, certain conditions mandate immediate trip to the operating room:
* Vascular Injury: Requiring repair or bypass by a vascular surgeon. Prophylactic fasciotomies are routinely performed during revascularization.
* Irreducible Dislocation: Often due to soft tissue interposition. A classic sign is the "dimple sign" or puckering along the medial joint line, indicating the medial capsule and MCL are trapped within the joint during a posterolateral dislocation.
* Open Knee Dislocation: Requiring emergent irrigation and debridement.
* Compartment Syndrome: Requiring emergent four-compartment fasciotomy.
If splinting is inadequate to maintain a concentric reduction (highly unstable KD-IV injuries), a spanning external fixator should be applied. Transarticular pinning should be avoided due to the risk of articular cartilage damage and pin-tract infection communicating with the joint.
SURGICAL RECONSTRUCTION: PRINCIPLES AND TECHNIQUES
Historically, nonoperative treatment (cast immobilization) was favored due to the complexity of the injuries. However, modern meta-analyses conclusively demonstrate that early surgical repair or reconstruction of disrupted ligaments produces superior functional results, greater stability, and a significantly lower risk of arthrofibrosis compared to nonoperative management, especially in young, active patients.
Timing of Surgery
If the knee is concentrically reduced and vascularly intact, surgery is typically delayed for 2 to 3 weeks. This delay allows the capsular structures to heal (preventing fluid extravasation and compartment syndrome during arthroscopy) and allows the inflammatory phase to subside, reducing the risk of postoperative arthrofibrosis.
Patient Positioning and Setup
- The patient is placed supine on the operating table.
- A high-thigh tourniquet is applied but inflated only if necessary, to minimize ischemic time in a previously traumatized limb.
- A lateral post or leg holder is utilized to allow valgus stress, though care must be taken not to apply excessive stress to an already incompetent medial side.
- The contralateral leg is prepped and draped if autograft harvest (e.g., bone-patellar tendon-bone or hamstrings) is planned. Allograft tissue (Achilles, tibialis anterior, or hamstring) is frequently utilized in multi-ligament reconstructions to decrease donor-site morbidity and operative time.
Surgical Approaches and Incisions
Careful planning of incisions is critical to avoid skin necrosis, especially when multiple approaches are required.
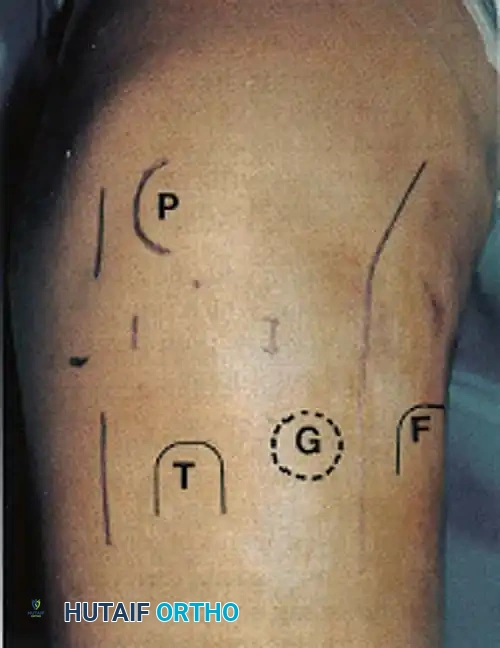
Fig. 4: Standard surgical landmarks and planned incisions for multi-ligament knee reconstruction. (P = Patella, T = Tibial tubercle, G = Gerdy's tubercle, F = Fibular head).
- Standard Arthroscopic Portals: Anterolateral and anteromedial portals for intra-articular work.
- Posteromedial Portal: Essential for PCL tibial footprint preparation and inlay techniques.
- Medial Approach: A longitudinal incision centered over the medial epicondyle extending distally to the pes anserinus for MCL and posteromedial corner (PMC) repair/reconstruction.
- Lateral Approach: A curvilinear incision based over the lateral epicondyle, extending distally between Gerdy's tubercle and the fibular head, utilized for LCL and posterolateral corner (PLC) reconstruction.
Step-by-Step Reconstruction Sequence
The general consensus for the sequence of multi-ligament reconstruction is to build from the center outward, establishing the central pivot before addressing the peripheral stabilizers.
1. Diagnostic Arthroscopy and Cruciate Preparation
- Perform a careful diagnostic arthroscopy. Use gravity flow or a low-pressure pump to avoid fluid extravasation into the calf compartments.
- Debride the torn stumps of the ACL and PCL.
- Address any repairable meniscal pathology. Meniscal preservation is paramount to protect the reconstructed ligaments from excessive stress.
2. Posterior Cruciate Ligament (PCL) Reconstruction
The PCL is the primary stabilizer of the knee and is typically reconstructed first.
* Tunnel Preparation: The femoral tunnel is drilled inside-out at the anatomic footprint of the anterolateral bundle (and posteromedial bundle if a double-bundle technique is used).
* Tibial Preparation: Depending on surgeon preference, a transtibial tunnel is drilled, or an open tibial inlay technique is performed via a posteromedial approach. The inlay technique avoids the "killer turn" of the transtibial route, potentially reducing graft abrasion.
* The PCL graft is passed but not yet tensioned or fixed distally.
3. Anterior Cruciate Ligament (ACL) Reconstruction
- Femoral and tibial tunnels are drilled anatomically.
- The ACL graft is passed into the joint.
- Fixation Sequence: The PCL is tensioned and fixed first, typically at 90 degrees of flexion with an anterior drawer force applied to restore the normal anatomic tibial step-off. Following PCL fixation, the ACL is tensioned and fixed in full extension or slight flexion (0-20 degrees).
4. Posterolateral Corner (PLC) Reconstruction
Failure to recognize and reconstruct the PLC is the leading cause of cruciate reconstruction failure.
* Through the lateral approach, identify and protect the common peroneal nerve.
* Anatomic reconstruction (e.g., LaPrade technique) involves reconstructing the LCL, popliteus tendon, and popliteofibular ligament using a split Achilles allograft or hamstring autografts.
* Fibular and tibial tunnels are drilled. The grafts are passed and fixed with the knee in 30 degrees of flexion and neutral rotation, applying a valgus and internal rotation force.
5. Medial Collateral Ligament (MCL) and Posteromedial Corner (PMC)
- Avulsions from the femur or tibia can sometimes be repaired acutely with suture anchors if tissue quality is robust.
- Midsubstance tears or chronic presentations require reconstruction using allograft or autograft, recreating the superficial MCL and the posterior oblique ligament (POL).
- Fixation is typically performed at 20 to 30 degrees of flexion with a varus force applied to eliminate medial gapping.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Aggressive, yet carefully phased rehabilitation is critical. The goal is to navigate the narrow therapeutic window between arthrofibrosis (stiffness) and graft stretching (recurrent instability).
- Phase I (Weeks 0-2): The knee is immobilized in a hinged brace locked in full extension. Weight-bearing is strictly non-weight-bearing (NWB) or toe-touch weight-bearing (TTWB). Focus is on edema control, quadriceps activation (straight leg raises), and patellar mobilization to prevent infrapatellar contracture syndrome.
- Phase II (Weeks 2-6): Passive range of motion (PROM) is initiated. If the PCL was reconstructed, flexion is typically limited to 90 degrees, and active hamstring contraction is strictly avoided to prevent posterior tibial translation.
- Phase III (Weeks 6-12): Progression to partial, then full weight-bearing. Active range of motion is advanced. Closed-chain kinetic exercises are initiated.
- Phase IV (Months 3-9): Focus on proprioception, progressive strengthening, and functional movement patterns. Return to sport or heavy labor is rarely permitted before 9 to 12 months, and only after objective functional testing demonstrates >85% limb symmetry index.
COMPLICATIONS
- Vascular Compromise: The most catastrophic complication. Delayed thrombosis of the popliteal artery can lead to compartment syndrome, ischemic contracture, or amputation.
- Arthrofibrosis: The most common complication following multi-ligament reconstruction. Requires aggressive physical therapy, and potentially manipulation under anesthesia (MUA) or arthroscopic lysis of adhesions if ROM plateaus after 3-4 months.
- Neurological Deficit: Peroneal nerve palsy may be transient (neurapraxia) or permanent. If no recovery is noted clinically or on EMG by 3 to 6 months, tendon transfers (e.g., posterior tibial tendon to the dorsum of the foot) or an ankle-foot orthosis (AFO) may be required to manage foot drop.
-
Recurrent Instability: Often due to unrecognized peripheral corner injuries (PLC or PMC), premature return to activity, or biologic failure of the grafts. Preexisting mechanical alignment must be considered; a patient with severe varus alignment and a reconstructed LCL/PLC is at high risk for graft stretching unless a concurrent high tibial osteotomy (HTO) is performed.
