Mastering Trapeziometacarpal Arthrodesis and Rheumatoid Wrist Synovectomy
Key Takeaway
Trapeziometacarpal arthrodesis is a highly effective surgical intervention for advanced carpometacarpal joint arthritis, providing durable pain relief and stability. This procedure involves meticulous cup-and-cone joint preparation, precise positioning in 45 degrees of palmar abduction, and rigid internal fixation using a plate or Kirschner wires. Concurrently, addressing rheumatoid wrist synovitis through dorsal or volar synovectomy is critical to preventing progressive carpal destabilization and debilitating extensor or flexor tendon ruptures.
TRAPEZIOMETACARPAL ARTHRODESIS
Trapeziometacarpal (TMC) arthrodesis is a powerful, durable surgical intervention for advanced osteoarthritis or post-traumatic arthritis of the thumb carpometacarpal (CMC) joint. While suspensionplasty and interposition arthroplasty remain popular for older, lower-demand patients, TMC arthrodesis is the gold standard for young, high-demand patients, heavy manual laborers, and individuals requiring absolute pinch strength and thumb stability. By fusing the joint, the procedure eliminates pain while preserving the length of the thumb ray, thereby optimizing the biomechanics of the intrinsic and extrinsic thumb musculature.
Indications and Contraindications
Indications:
* Isolated, symptomatic Eaton-Littler Stage II or III osteoarthritis of the TMC joint.
* Post-traumatic arthritis following Bennett or Rolando fractures.
* High-demand patients (e.g., manual laborers, mechanics, young active individuals) who require maximum grip and key pinch strength.
* Failed prior ligament reconstruction or instability procedures.
Contraindications:
* Eaton-Littler Stage IV disease (involving the scaphotrapeziotrapezoid [STT] joint). Fusing the TMC joint in the presence of STT arthritis will rapidly accelerate STT degeneration due to increased compensatory motion.
* Severe thumb metacarpophalangeal (MCP) joint hyperextension instability (unless addressed concurrently).
* Elderly, low-demand patients who prioritize mobility over absolute strength.
Biomechanics and Optimal Joint Positioning
The success of a TMC arthrodesis hinges entirely on achieving the correct three-dimensional spatial orientation of the thumb. Improper positioning leads to severe functional deficits, such as the inability to place the hand flat on a surface or the inability to perform a functional pinch.
Surgical Pearl: The "Fist and Flat" Rule
The ideal position for TMC arthrodesis is approximately 40 to 45 degrees of palmar abduction, 30 degrees of radial abduction, and 15 degrees of pronation. Clinically, this means the thumb pulp should comfortably oppose the index and middle fingers, and when the hand is held in a tight fist, the thumb should overlie the dorsum of the middle phalanx of the index finger. Furthermore, the patient must be able to lay their palm completely flat on a table.
Surgical Technique: Step-by-Step
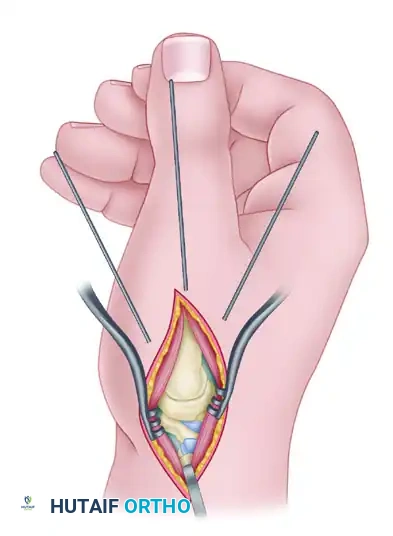
1. Incision and Exposure
The procedure is performed under regional anesthesia (supraclavicular or axillary block) with a proximal arm tourniquet.
A dorsal-radial or Wagner incision is utilized, centered over the TMC joint. The incision extends from the proximal third of the first metacarpal to just proximal to the radiocarpal joint.
Meticulous blunt dissection is required in the subcutaneous tissues to identify and protect the terminal branches of the superficial radial nerve (SRN) and the lateral antebrachial cutaneous nerve. The first dorsal compartment is identified, and the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) tendons are mobilized and retracted. The radial artery, which crosses the operative field proximally in the anatomic snuffbox, must be carefully protected.
The joint capsule is incised longitudinally, and subperiosteal flaps are elevated to expose the base of the first metacarpal and the distal articular surface of the trapezium.
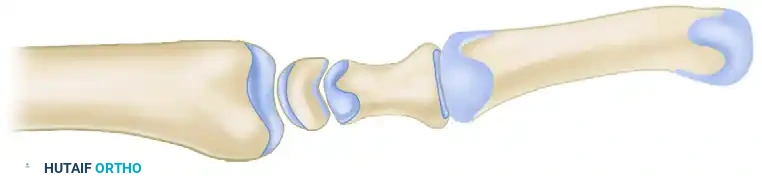
2. Joint Preparation: The Cup-and-Cone Technique
Achieving a high union rate requires maximizing the cancellous bone contact area. The "cup-and-cone" technique is highly recommended as it provides intrinsic stability and allows for fine-tuning of the thumb position before definitive fixation.
- Metacarpal Preparation (The Cone): Use a rongeur and an air-driven burr to remove the remaining articular cartilage and dense subchondral bone from the base of the first metacarpal. Shape the base into a convex, cone-shaped surface of healthy, bleeding cancellous bone.
- Trapezial Preparation (The Cup): Use a high-speed burr, curet, and small osteotomes to shape the distal articular surface of the trapezium into a concave cup configuration. The radius of curvature must match the metacarpal cone perfectly.
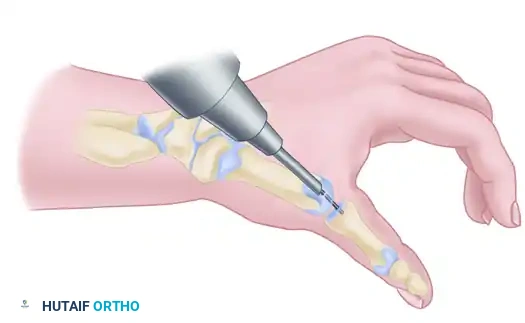
Appose the prepared bone surfaces and assess the fit. The cup-and-cone geometry allows the surgeon to rotate and angulate the metacarpal into the perfect functional position without losing bony contact.

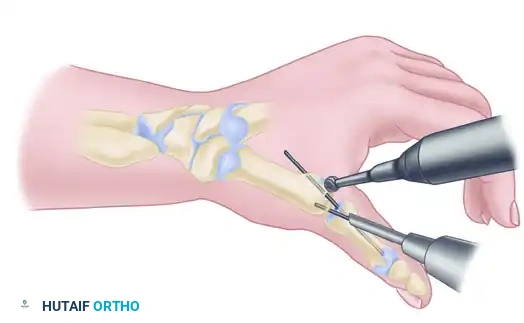
3. Provisional Fixation and Bone Grafting
Place the thumb in the optimal position (45 degrees palmar abduction, slight pronation). Temporarily stabilize the joint by driving a 1.6-mm Kirschner wire (K-wire) antegrade from the dorsal metacarpal shaft into the trapezium.
Confirm bony apposition, alignment, and hardware placement with multi-planar fluoroscopy.

Surgical Warning: Assessing Bone Stock
Once satisfactory joint positioning is confirmed, critically evaluate the quality of the bony apposition. Sclerotic bone or areas of suboptimal contact will lead to non-union. If defects are present, supplemental cancellous bone graft is mandatory.
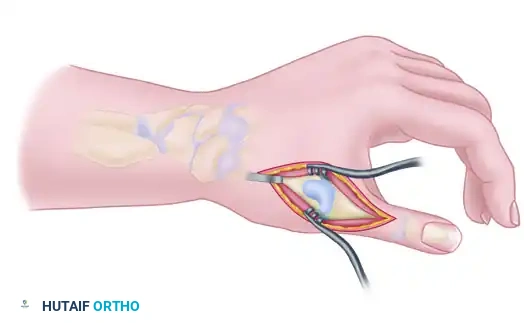
Bone Graft Harvest:
If grafting is required, extend the incision proximally over the distal radius. Protect the sensory nerves and release the first dorsal compartment. Make a 5 × 5-mm cortical window in the radial metaphysis (Lister's tubercle area) to harvest rich cancellous bone graft. Pack this graft tightly into any fusion defects at the TMC joint to ensure a continuous trabecular bridge.
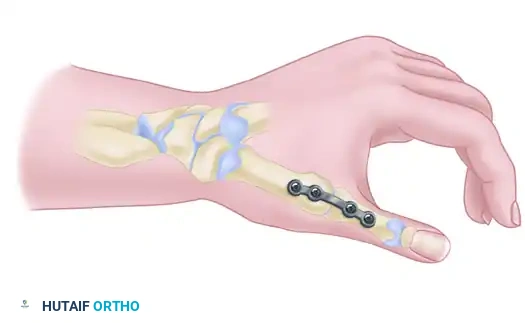
4. Definitive Fixation
Rigid internal fixation is paramount. The surgeon may choose between plate-and-screw fixation or multiple K-wires, depending on bone quality and surgeon preference.
Option A: Plate Fixation (Preferred for Rigid Stability)
With the provisional K-wire in place, contour a 2.4-mm T-plate or a 2.0-mm/2.4-mm minicondylar blade plate (e.g., Synthes USA, Paoli, PA) to the dorsal-radial aspect of the joint. Insert the screws, ensuring at least two (preferably three) screws achieve bicortical purchase in both the metacarpal and the trapezium.
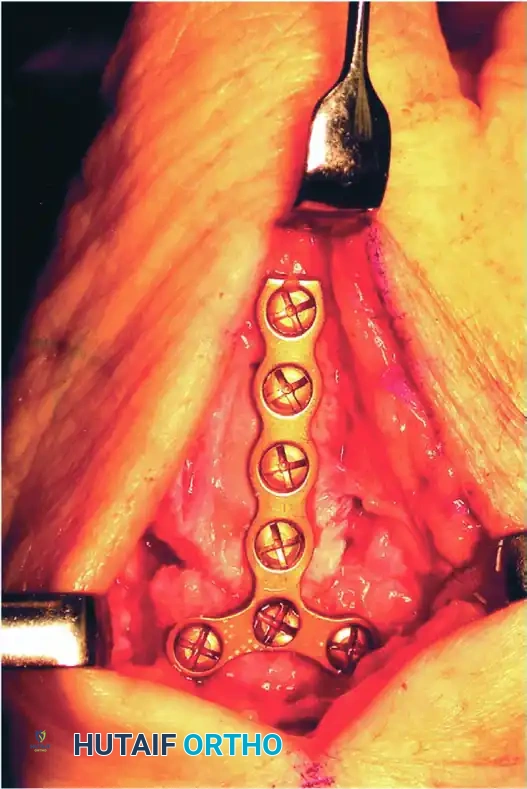
Take extreme care to use image intensification in multiple planes. It is critical to ensure that the screws or blades do not penetrate the adjacent STT joint or the CMC joint of the index finger.

Option B: Kirschner Wire Fixation
If K-wire fixation is chosen (often preferred in cases of small trapezial bone stock where a plate might cause comminution), drive three 1.1-mm or 1.6-mm wires retrograde from the metacarpal into the trapezium.
The first pin follows the planned longitudinal axis of the bone fusion. The other two pins should diverge 10 to 20 degrees from this central axis to provide rotational stability.
Take care to avoid pin penetration into the scaphotrapeziotrapezoid (STT) joint. Leave the pins protruding slightly outside the skin, capped, for later removal in the clinic.
Postoperative Protocol
- Close the capsule and skin in a routine, layered fashion.
- Apply a bulky, sterile dressing and a rigid short-arm thumb spica cast in the operating room. The interphalangeal (IP) joint of the thumb is left free to allow early active motion and prevent tendon adhesions.
- Weeks 0-6: Absolute immobilization in the cast.
- Week 6: Remove the cast (and K-wires if utilized). Obtain radiographs to assess trabecular bridging. Transition to a custom thermoplastic thumb spica splint.
- Weeks 6-12: Initiate progressive range of motion for the wrist and thumb IP joint. Begin gentle strengthening at 8 weeks if radiographic union is progressing.
- Months 3-4: Return to heavy manual labor or unrestricted activities once solid radiographic and clinical union is achieved.
RHEUMATOID DEFORMITIES OF THE WRIST
Rheumatoid arthritis (RA) is a systemic autoimmune disease characterized by chronic, hypertrophic synovitis. The wrist is the "keystone" of hand function, and rheumatoid involvement here is nearly universal. The proliferating synovium (pannus) releases proteolytic enzymes that destroy articular cartilage, attenuate critical stabilizing ligaments, and directly invade tendons, leading to profound deformity and functional collapse.
Pathophysiology of Carpal Collapse
The natural history of rheumatoid wrist disease follows a predictable pattern of destabilization:
1. Ulnar Styloid Erosion: Radiographs may reveal a small pit at the base of the ulnar styloid as the first radiographic evidence of the disease, caused by prestyloid recess synovitis.
2. Ligamentous Attenuation: The radiocarpal and midcarpal ligaments stretch under the pressure of the hypertrophic synovium.
3. Carpal Shift: The carpus translates ulnarly and subluxates volarly down the slope of the distal radius.
4. Metacarpal Compensation: As the carpus shifts ulnarly, the metacarpals undergo radial angulation to maintain the mechanical axis, which subsequently drives the classic ulnar deviation of the fingers at the MCP joints.
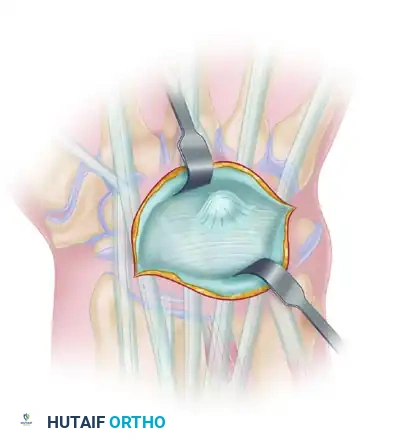
SYNOVITIS OF THE WRIST: DORSAL COMPARTMENT
Painful dorsal wrist swelling is frequently the presenting symptom in rheumatoid arthritis. This tenosynovial swelling may initially mimic or contribute to de Quervain disease, trigger finger, or carpal tunnel syndrome, masking the underlying systemic etiology.
The synovitis can spread rapidly, causing massive swelling in the shape of an hourglass—the middle being constricted by the unyielding dorsal carpal ligament (extensor retinaculum).
Extensor Tendon Rupture (Vaughan-Jackson Syndrome)
If left untreated, the hypertrophic synovium directly invades the extensor tendons. Furthermore, the destruction of the distal radioulnar joint (DRUJ) leads to dorsal subluxation of the distal ulna (Caput Ulnae Syndrome). The subluxated, eroded ulnar head acts as a saw blade against the extensor tendons.
Tendons, especially those of the three ulnar finger extensors (EDM, EDC to the small and ring fingers), may rupture sequentially from ulnar to radial. This is a catastrophic event; function can never be restored completely to its pre-morbid state.
Indications for Dorsal Synovectomy
If the synovitis is only moderate, and if changes in the bones are absent but pain is significant, a dorsal synovectomy of the wrist is of lasting benefit.
Clinical Pitfall: The 6-Week Rule
Persistent swelling at the dorsum of the wrist that continues for 6 weeks or longer despite adequate medical treatment (DMARDs, biologics) is an absolute indication for a surgical dorsal synovectomy. This must be considered a prophylactic measure to avoid irreversible extensor tendon rupture.
Surgical Management of Dorsal Synovitis
- Exposure: A longitudinal dorsal incision is made. The extensor retinaculum is divided, often stepping the cut to allow for later reconstruction or relocation of the retinaculum deep to the extensor tendons to shield them from the carpus.
- Synovectomy: Meticulous excision of all hypertrophic synovium from the extensor tendon sheaths and the radiocarpal/midcarpal joints.
- Tendon Reconstruction: Any tendons ruptured at the wrist level must be repaired or reconstructed at the time of synovectomy. Options include:
- Distal side-to-side suture of the ruptured tendon to an adjacent intact tendon (e.g., ruptured EDC of the ring finger sutured to the intact EDC of the middle finger).
- Free tendon grafts (e.g., palmaris longus).
- Tendon transfers (e.g., Extensor Indicis Proprius [EIP] transferred to the Extensor Pollicis Longus [EPL] to restore thumb extension).
- DRUJ Management: If caput ulnae is present, a Darrach procedure (distal ulnar resection) or a Sauvé-Kapandji procedure (DRUJ arthrodesis with proximal ulnar pseudoarthrosis) is performed concurrently to remove the bony impingement.
SYNOVITIS OF THE WRIST: VOLAR COMPARTMENT
Hypertrophy of the volar wrist synovium, even though undetectable clinically due to the thick palmar fascia and transverse carpal ligament, can cause severe median nerve compression and symptoms of carpal tunnel syndrome. Synovitis is considered one of the most frequent causes of secondary carpal tunnel syndrome in the RA population.
Indications for Volar Tenosynovectomy
Compression of the median nerve in rheumatoid arthritis should be relieved surgically if conservative treatment with splinting and corticosteroid injections has been unsuccessful. If hypertrophy of the tenosynovium on the volar aspect of the wrist is obvious clinically, with or without symptoms of median nerve compression, a palmar (flexor) tenosynovectomy is highly useful in relieving pain and preventing flexor tendon rupture.
Flexor Tendon Rupture and the Mannerfelt Lesion
The level of the deep transverse carpal ligament is a frequent site of rupture for flexor tendons. However, a more insidious mechanism occurs at the floor of the carpal tunnel.
Erosion of the distal end of the radius or the carpal scaphoid into the floor of the carpal tunnel creates sharp bony spicules. These osteophytes can cause fraying and eventual attritional rupture of several profundus tendons. This specific pathology—attritional rupture of the flexor pollicis longus (FPL) or the index flexor digitorum profundus (FDP) over a scaphoid osteophyte—is known as a Mannerfelt lesion.
Surgical Management of Volar Synovitis
- Exposure: An extended carpal tunnel incision is utilized, crossing the wrist crease obliquely to avoid contracture.
- Decompression: The transverse carpal ligament is completely released to decompress the median nerve.
- Tenosynovectomy: A meticulous, tendon-by-tendon synovectomy is performed. The surgeon must inspect the floor of the carpal tunnel (the volar radiocarpal ligaments).
- Bony Debridement: Any protruding osteophytes from the radius or scaphoid must be aggressively rongeured flat, and the defect covered with a local capsular flap to prevent recurrent tendon abrasion.
- Tendon Repair: Wrist-level flexor tendon ruptures are best repaired by side-to-side suture to adjoining intact tendons or by segmental grafts. However, in the case of an FPL rupture in a rheumatoid patient, an arthrodesis of the thumb interphalangeal (IP) joint is often a more reliable and preferred procedure than complex tendon grafting, providing a stable, pain-free post for pinch.
Conclusion
The surgical management of the rheumatoid wrist requires a comprehensive understanding of the disease's progressive nature. Whether performing a prophylactic synovectomy to save tendons or executing a complex trapeziometacarpal arthrodesis to restore pinch stability, the orthopedic surgeon must balance meticulous soft-tissue handling with rigid biomechanical principles to optimize patient outcomes.
📚 Medical References
- Trapeziometacarpal arthrodesis: a functional evaluation, J Hand Surg 17A:604, 1992.
- Barron OA, Eaton RG: Save the trapezium: double interposition arthroplasty for the treatment of stage IV disease of the basal joint, J Hand Surg 23A:196, 1998.
- Bezwada HP, Sauer ST, Hankins ST, et al: Long-term results of trapeziometacarpal silicone arthroplasty, J Hand Surg 27A:409, 2002.
- Budoff JE, Gordon L: Long-term results of tendon shortening trapeziometacarpal arthroplasty, Clin Orthop Relat Res 405:199, 2002.
- Burton RI, Pelligrini VD Jr: Surgical management of basal joint arthritis of the thumb: II. Ligament reconstruction with tendon interposition arthroplasty, J Hand Surg 11A:324, 1986.
- Caputo RJ, Bennett JB: Power staple fi xation in trapeziometacarpal arthrodesis, J Hand Surg 18A:926, 1993.
- Carroll RE: Arthrodesis of the carpometacarpal joint of the thumb: a review of patients with a long postoperative period, Clin Orthop Relat Res 220:106, 1987.
- Creighton JJ, Steichen JB, Strickland JW: Long-term evaluation of silastic trapezial arthroplasty in patients with osteoarthritis, J Hand Surg 16A:510, 1991.
- Dell PC, Muniz RB: Interposition arthroplasty of the trapeziometacarpal joint for osteoarthritis, Clin Orthop Relat Res 220:27, 1987.
- De Smet L, Stoen W, Spaepen D, et al: Total joint arthroplasty for osteoarthritis of the thumb basal joint, Acta Orthop Belg 70:19, 2004.
- Doyle JR: Sliding bone graft technique for arthrodesis of the trapeziometacarpal joint of the thumb, J Hand Surg 16A:363, 1991.
- Eaton RG: Replacement of the trapezium, J Bone Joint Surg 61A:76, 1979.
- Eaton RG, Glickel S, Littler J: Tendon interposition arthroplasty for degenerative arthritis of the trapeziometacarpal joint of the thumb, J Hand Surg 10A:645, 1985.
- Eaton RG, Littler JW: Ligament reconstruction for the painful thumb carpometacarpal joint, J Bone Joint Surg 55A:1665, 1973.
- Freedman DA, Eaton RG, Glickel SZ: Long-term results of volar ligament reconstruction for symptomatic basal joint laxity, J Hand Surg 25A:297, 2000.
- Gervis W: A review of excision of the trapezium for osteoarthritis of the trapeziometacarpal joint after twenty-fi ve years, J Bone Joint Surg 55B:56, 1973.
- Glickel SZ, Kornstein AN, Eaton RG: Long-term follow-up of trapeziometacarpal arthroplasty with coexisting scaphotrapezial disease, J Hand Surg 17A:612, 1992.
- Goldner JL, Clippinger FW: Excision of the greater multangular bone as an adjunct to mobilization of the thumb, J Bone Joint Surg 41A:609, 1959.
- Hay EL, Bomberg BC, Burke C, et al: Long-term results of silicone trapezial implant arthroplasty, J Arthroplasty 3:215, 1988.
- Herndon JH: Trapeziometacarpal arthroplasty: a clinical review, Clin Orthop Relat Res 220:99, 1987.
- Irwin AS, Maffulli N, Chesney RB: Scaphotrapezoid arthritis: a cause of residual pain after arthroplasty of the trapeziometacarpal joint, J Hand Surg 20B:346, 1995.
- Jennings CD, Livingstone DP: Convex condylar arthroplasty of the basal joint of the thumb: failure under load, J Hand Surg 15A:573, 1990.
- Jones NF, Maser BM: Treatment of arthritis of the trapeziometacarpal joint with trapeziectomy and hematoma arthroplasty, Hand Clin 17:237, 2001.
- Kleinman WB, Eckenrode JF: Tendon suspension sling arthroplasty for thumb trapeziometacarpal arthritis, J Hand Surg 16A:983, 1991.
- Kuhns CA, Emerson ET, Meals RA: Hematoma and distraction arthroplasty for thumb basal joint osteoarthritis: a prospective, single-surgeon study including outcomes measures, J Hand Surg 28A:381, 2003.
- Lane LB, Eaton RG: Ligament reconstruction for the painful “prearthritic” thumb carpometacarpal joint, Clin Orthop Relat Res 220:52, 1987.
- Le Viet D, Kerboull L, Lantieri LA, et al: Stabilized resection arthroplasty by an anterior approach in trapeziometacarpal arthritis: results and surgical technique, J Hand Surg 21A:194, 1996.
- Lins RE, Gelberman RH, McKeown L, et al: Basal joint arthritis: trapeziectomy with ligament reconstruction and tendon interposition arthroplasty, J Hand Surg 21A:202, 1996.
- Livesey JP, Norris SH, Page RE: First carpometacarpal joint arthritis: a comparison of two arthroplasty techniques, J Hand Surg 21B:182, 1996.
- Lucht U, Vang PS, Munck J: Soft tissue interposition arthroplasty for osteoarthritis of the CMC joint of the thumb, Acta Orthop Scand 51:767, 1980.
- MacDermid JC, Roth JH, Rampersaud R, et al: Trapezial arthroplasty with silicone rubber implantation for advanced osteoarthritis of the trapeziometacarpal joint of the thumb, Can J Surg 46:103, 2003.
- Melone CP Jr, Beavers B, Isani A: The basal joint pain syndrome, Clin Orthop Relat Res 220:58, 1987.
- Menon J: Partial trapeziectomy and interpositional arthroplasty for trapeziometacarpal osteoarthritis of the thumb, J Hand Surg 20B:700, 1995.
- Menon J: Arthroscopic management of trapeziometacarpal joint arthritis of the thumb, Arthroscopy 12:581, 1996.
- Menon J, Schoene HR, Hohl JC: Trapeziometacarpal arthritis: results of tendon interpositional arthroplasty, J Hand Surg 6:442, 1981.
- Millender LH, Nalebuff EA, Amadio P, et al: Interpositional arthroplasty for rheumatoid carpometacarpal joint disease, J Hand Surg 3A:533, 1978.
- Muermans S, Coenen L: Interpositional arthroplasty with GoreTex, Marlex or tendon for osteoarthritis of the trapeziometacarpal joint: a retrospective comparative study, J Hand Surg 23B:64, 1998.
- Mureau MAM, Rademaker RPC, Verhaar JAN, et al: Tendon interposition arthroplasty versus arthrodesis for the treatment of trapeziometacarpal arthritis: a retrospective comparative followup study, J Hand Surg 26A:869, 2001.
- Nusem I, Goodwin DR: Excision of the trapezium and interposition arthroplasty with Gelfoam for the treatment of trapeziometacarpal osteoarthritis, J Hand Surg 23B:242, 2003.
- O’Leary ST, Grobbelaar AO, Goldsmith N, et al: Silicone arthroplasty for trapeziometacarpal arthritis, J Hand Surg 27B:457, 2002.
- Peimer CA: Long-term complications of trapeziometacarpal silicone arthroplasty, Clin Orthop Relat Res 220:86, 1987.
- Pérez-Úbeda MJ, García-López A, Martinez FM, et al: Results of the cemented SR trapeziometacarpal prosthesis in the treatment of thumb carpometacarpal osteoarthritis, J Hand Surg 28A:917, 2003.
- Phaltankar PM, Magnussen PA: Hemiarthroplasty for trapeziometacarpal arthritis—a useful alternative? J Hand Surg 23B:80, 2003.
- Pomerance JF: Painful basal joint arthritis of the thumb: II. Treatment, Am J Orthop 24:466, 1995.
- Robinson D, Halperin N: Abductor pollicis longus arthroplasty of the trapeziometacarpal joint: surgical technique and results, J Hand Surg 16A:504, 1991.
- Ruffi n RA, Rayan GM: Treatment of trapeziometacarpal arthritis with Silastic and metallic implant arthroplasty, Hand Clin 17:245, 2001.
- Stark HH, Moore JF, Ashworth CR, et al: Fusion of the fi rst metacarpotrapezial joint for degenerative arthritis, J Bone Joint Surg 59A:22, 1977.
- Swanson AB: Disabling arthritis at the base of the thumb: treatment by resection of the trapezium and fl exible (silicone) implant arthroplasty, J Bone Joint Surg 54A:456, 1972.
- Swanson AB: Disabilities of the thumb joints and their surgical treatment, including fl exible implant arthroplasty, Instr Course Lect 22:88, 1973.
- Swanson AB, deGroot-Swanson G: Reconstruction of the thumb basal joints: development and current status of implant techniques, Clin Orthop Relat Res 220:68, 1987.
- Swanson AB, deGroot-Swanson G, Watermeier JJ: Trapezium implant arthroplasty: long-term evaluation of 150 cases, J Hand Surg 6A:125, 1981.
- Tägil M, Kopylov P: Swanson verus APL arthroplasty in the treatment of osteoarthritis of the trapeziometacarpal joint: a prospective and randomized study in 26 patients, J Hand Surg 27B:452, 2002.
- Tomaino MM, Vogt M, Weiser R: Scaphotrapezoid arthritis: prevalence in thumbs undergoing trapezium excision arthroplasty and effi cacy of proximal trapezoid excision, J Hand Surg 24A:1220, 1999.
- Trumble TE, Rafi jah G, Gilbert M, et al: Thumb trapeziometacarpal joint arthritis: partial trapeziectomy with ligament reconstruction and interposition costochondral allograft, J Hand Surg 25A:61, 2000.
- Varitimidis SE, Fox RJ, King JA, et al: Trapeziometacarpal arthroplasty using the entire fl exor carpi radialis tendon, Clin Orthop Relat Res 370:164, 2000.
- Distal Radioulnar Joint Bain GI, Pugh DMW, MacDermic JC, et al: Matched
You Might Also Like