DEFINITION
Injuries caused by high-pressure injection equipment, which can generate pressures of 2000 to 12,000 pound per square inch (psi),9 are more than sufficient force to break the skin.15 Substances typically injected include grease, paint, paint thinners, diesel fuel, oil, water, and cement. Cases involving molten metal,3 dry cleaning solvents,11 and veterinary vaccines5 have also been documented.Hallmark of injury is an innocuous-appearing superficial wound that can greatly underestimate the true extent of injury (FIG 1).The three most important determinants of morbidity are the (1) type of substance injected, (2) anatomic location of injury, and (3) delay in treatment.Treatment of injection injuries is urgent and thorough surgical débridement.High-pressure injection injuries occur most frequently in young men, particularly among those who are manual laborers.Previously, it was thought that most of these injuries occurred to people who had been on the job for less than 6 months, but more recent studies show that the mean time on the job was 11 years.12,32Typical scenarios include grasping pressurized tubing in which there is a break in the seal or attempting to unclog the nozzle of a high-pressure injector with the guard removed (FIG 2).With the increasing use of power contrast injection in computed tomography (CT), contrast extravasation injuries may be classified under injection injuries of the upper extremity. However, the pressures involved are generally much lower (100 psi),33 the associated injuries are more proximal, and the natural history isgenerally benign, with surgery rarely being required. FIG 1 • An innocuous-appearing puncture of the volar radial surface of the right small finger. This may be the only visible point of injury in a high-pressure injection injury.


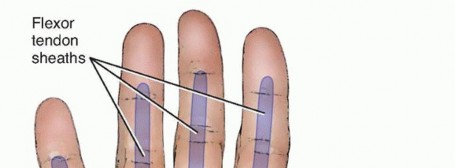
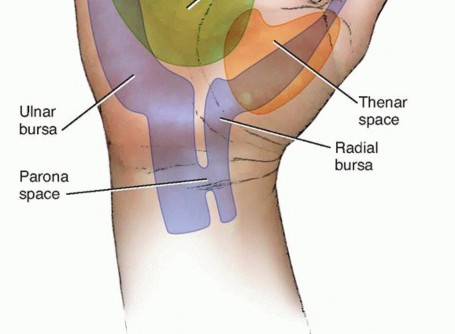
ANATOMY

FIG 2 • Injury commonly occurs to the nondominant hand while attempting to clean the nozzle of a high-pressure injector. Note that the nozzle guard has been removed.

PATHOGENESIS
Two key pathogenic mechanisms are responsible for the morbidity of high-pressure injuries: (1) mechanical injury directly resulting from the injected material, which is a function of viscosity, velocity, and volume, and (2) the inflammatory host response, which is a function of the irritant/chemical properties of the injected material.The degree of mechanical injury has been shown to be inversely proportional to the viscosity of the material and proportional to the volume of material delivered and the pressure at which it was delivered.9,13,27 For example,injected material with relatively low viscosity, such as paint thinner,10 has been shown to result in wider zones of injury and greater morbidity.The type of inflammatory response incited by the injected material also has an important effect on degree of injury. Only rare cases of water or air injection have been found to result in amputation. In contrast, organic solvents such as oil paint have been found to have a 10-fold increased incidence of amputation compared to other materials such as hydraulic fluid or grease (58% vs. 6%). The inflammatory response to various materialsis clearly different.14Controversy continues as to which aspect dominates in these injuries; however, they are more likely synergistic, with the inflammatory response compounding the mechanical injury.Time elapsed before intervention has a major influence on prognosis (see Natural History, next section). Most agree that surgery should be done within 6 hours after injury to decrease morbidity.29
NATURAL HISTORY
The natural history of high-pressure injuries can be divided into three stages.Acute stageTheacute stageoccurs immediately.The injection causes external compression and spasm of the vessels, leading to compromised blood flow that is manifested by white, mottled tissue; numbness; severe pain; or a combination of these findings.Any initial paresthesias that occur are due to local compression or chemical irritation of the involved nerves.During this stage, the site of injection is key in determining where the material has spread.The volume of material injected also determines the degree of tissue distention and impairment of blood flow.In several studies by Gelberman et al,9 Schoo et al,27 and Hayes and Pan,13 patients with hands that had higher volume injections and longer time to decompression had higher morbidity rates.Intermediate stageDuring theintermediate stage, a foreign body reaction induces granuloma formation and fibrosis. Severity of inflammation that occurs is determined by the volume and type of substance.Injection of paint solvent has a significantly higher morbidity due to its low viscosity, allowing diffusionthrough the soft tissues. Its corrosive effects cause severe tissue necrosis.9P.1131Grease injections have more chronic inflammatory reactions, leading to prolonged sequelae (foreign bodygranulomas).13,28Schoo et al27 reported that amputation rates associated with various injection injuries were as follows: paint thinner, 80%; paint (soya alkyl base), 58%; automotive grease, 23%; and hydraulic fluid, 14%.Late stageLate stage of injury occurs when the granulomas break open, resulting in draining sinuses and cutaneouslesions.8,27Chronic sinuses may degenerate into malignancies (squamous epithelioma).8Secondary infections may occur in this stage; these may be due toStaphylococcus aureus,Streptococcus epidermidis,Pseudomonasspp., or a variety of polymicrobial flora.24,26
PATIENT HISTORY AND PHYSICAL FINDINGS
Important information includes hand dominance and occupation, sequence of events postinjury, and type of injector and pressure as well as substance injected.Comorbidities, including vascular disease, diabetes, and smoking history, are relevant risk factors that influence healing and posttreatment function.19If possible, a Material Safety Data Sheet (MSDS) for the substance injected should be obtained from the company or online athttp://www.msdsonline.com.Physical examination should include the following:Determining location of puncture site to determine spread of injected material. It is not uncommon for the site of injury to be small and difficult to find.Observing range of motion when the patient attempts to form a fistPalpation of the digit, hand, and arm to help determine the extent of required débridement
IMAGING AND OTHER DIAGNOSTIC STUDIES
Radiographs of the hand and forearm are helpful in evaluating the extent of injury.Although not all injected substances are radiopaque, air may be present in the compartments of the hand and forearm, which may help in determining how far the substance has traveled.23,24,31It may be necessary to obtain radiographs of the arm and chest. Extension into the arm, chest wall, and mediastinum from injuries to the hand has been reported.30Imaging studies also document preexisting pathology.
DIFFERENTIAL DIAGNOSIS
Snake bite Spider bite Crush injurySuppurative tenosynovitis Black thorn tenosynovitisMycobacterium marina infection (chronic)
NONOPERATIVE MANAGEMENT
Most injuries require surgical débridement, and there are only few case reports of nonoperative management for such injuries.Cases managed without surgery include air injection into the hand, which leads to subcutaneous emphysema that resolves within hours to days18 or, occasionally, water injection in an otherwise clean environment may be managed conservatively in some cases.17
SURGICAL MANAGEMENT
Early and aggressive decompression and débridement of all tissues is the cornerstone of treatment. Some authors also include amputation as a major treatment modality.The time from injury to surgery is the major determinant of morbidity and prognosis in high-pressure injection injuries.29
PREOPERATIVE PLANNING
Radiographic studies should be reviewed.Attention should be paid to radiopaque areas of the hand and forearm.Air in the soft tissue should be evaluated.Bones should be evaluated for any possible fractures or preexisting lesions.Intravenous (IV) lines should be placed in the patient's noninjured extremity, and manipulation of the injured extremity should be limited.
POSITIONING
Patient should be placed supine with the arm abducted.Arm should not be exsanguinated with an Esmarch bandage to avoid proximal spread of injected material and further trauma to the tissues.Regional nerve block can be used, if necessary.If an IV regional (Bier) block is selected, gravity exsanguination is performed without a compression wrap but with 4 minutes of elevation.
APPROACH
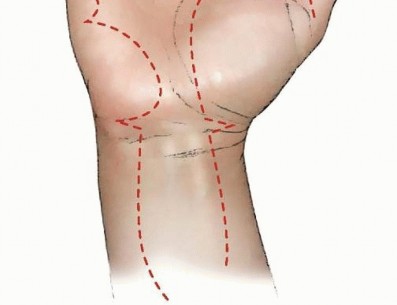
High-pressure injection injuries must be approached with a view to expose and débride all particulate matter. Incisions must follow the general principle of avoiding longitudinal incisions across flexion creases.Débridement of the neurovascular bundle, if affected, must be done with extreme caution. Some particulate matter may be left behind in order to preserve vital structures.All suspected compartments should be opened and explored.P.1132
TECHNIQUES
BRUNER INCISION
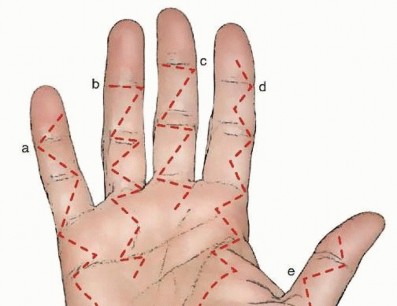
TECH FIG 1 • Various incisions for débridement. All are based on the principle of avoiding longitudinal
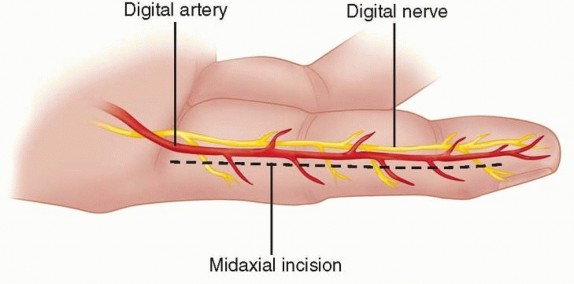
TECH FIG 2 • Midaxial incision of the finger. This sacrifices the dorsal branches of the neurovascular bundle, but the digital nerve and artery are protected.
Other Incisions
Other diagonal incisions may be used. These are similar to Bruner incision in that they adhere to the principle of avoiding crossing a flexion crease longitudinally. Littler incision (see FIG 1D) does not provide as wide as an exposure of the finger but minimizes exposure of the tendon sheath.
A mixed diagonal-transverse-type incision may also be used in these cases. A transverse incision is made parallel to the flexion crease and the next interphalangeal incision is another oblique Bruner incision (see TECH FIG 1c).
This is continued along the length of the digit onto the palm.
The authors use a mixed diagonal-transverse incision that is similar to the one described in TECH FIG 1b. This technique allows for loose closure of the incision along the creases while allowing drainage along the oblique incisions.
P.1133
OTHER INCISIONS
PEARLS AND PITFALLS
Understand that the underlying pathology will usually be worse than the external wound. Managing comorbidities are important in the care of patients with injection injuries.Obtain the MSDS to understand the toxic effects of the injected material. This can be obtained from the manufacturer or online athttp://www.msdsonline.com.Exploration should extend to clearly healthy tissue. Avoid “minimally invasive” treatment. Leave the wound open or very loosely closed.
POSTOPERATIVE CARE
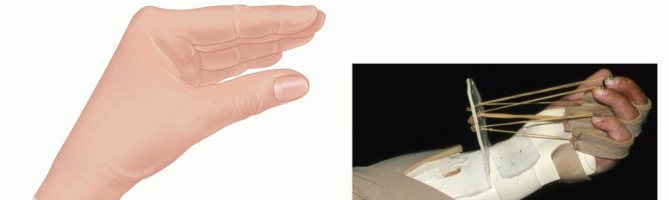
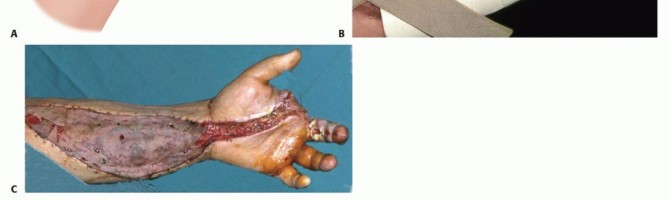
FIG 4 • A. The safe position for postoperative splinting. The wrist is slightly extended, the metacarpophalangeal joints are fully flexed, and the interphalangeal joints are fully extended. B. Dynamic splinting of the hand in flexion to allow for early mobilization. C. Primary and split-thickness skin graft closure of a wound after final débridement. No convincing human studies have been published that show that corticosteroids are effective in limitingtissue loss, and they should be used cautiously.14Early range-of-motion exercises are important to reduce the risk of stiffness and should be done prior to woundhealing.
OUTCOMES
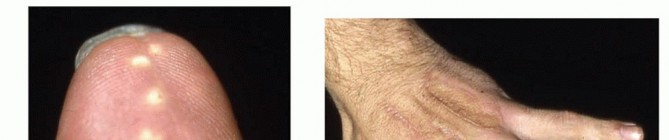
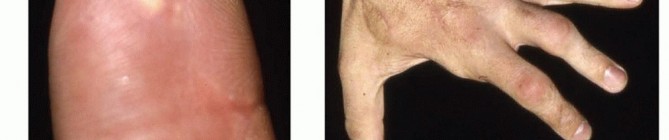
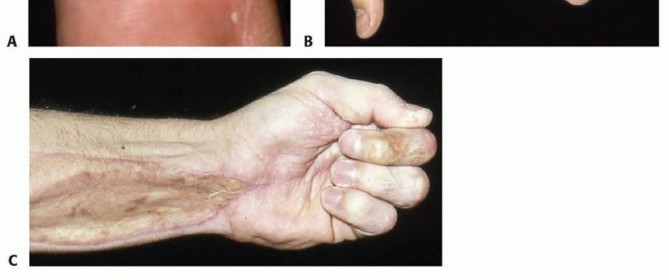
FIG 5 • A. Oleoma formation after débridement and closure of a digital high-pressure injection. The well-healed longitudinal incision on the volar surface of the digit is surrounded by yellow lesions, consistent with oleomas. B,C. Well-healed primary closures and split-thickness skin grafts of the volar and dorsal hand and forearm. There is full range of motion of the remaining digits after amputation of the index finger. In this subset of patients, time to débridement has a significant impact on amputation rate.Even if surgery occurs within 6 hours of injury, the amputation rate is 40%.If the surgery is delayed for more than 6 hours, the amputation rate increases to 57%.If débridement is delayed to more than 1 week after injury, the amputation rate is 88%.14Metacarpophalangeal range of motion decreases an average of 8.1%, proximal interphalangeal range of motion decreases 23.9%, and distal interphalangeal range of motion decreases by 29.7%.Maximum grip strength diminishes by 12% and pinch strength decreases by 35%. Two-point discrimination increases by 49%32 (FIG 5B,C).The average impairment for injuries caused by spray guns is 15%, by pneumatic hoses is less than 2%,and by hydraulic fluid is 6%.31If treatment is delayed more than 6 hours after injury, then permanent impairment rate is approximately 17%; however, if treatment is obtained in under 6 hours, that rate is only 4%.31Loss of work related to these injuries also varies, from 6 to 26 weeks, with about 92% of patients returning to their previous jobs.13
COMPLICATIONS
InfectionCold intolerance Hypersensitivity Oleoma formation Malignant degenerationDecreased range of motion and function ParesthesiasDiminished two-point discrimination Amputation
CONTRAST EXTRAVASATION INJURIES
Modern CT studies tend to use higher contrast injection rates.20Depending on the study, automated power injectors can deliver contrast at 4 to 5 mL per second, two to three times higher than for a routine survey CT. Pressures generated by an automated power injector can reach 100 psi. Typical volume of contrast administered varies greatly depending on the study and image acquisitioncapabilities of the scanner but varies from 30 to 50 mL.33Increasing use of automated power injectors has led to an increased incidence and severity of extravasation injuries. Prior to mechanical injectors, rate of extravasation ranged from 0.03% to 0.17%. More recently, the incidence has increased to 0.25% to 0.9%.33 Furthermore, contrast extravasations from automated pressureinjectors tend to be higher volume. Accordingly, approximately 60% of contrast extravasations involve volumesgreater than 50 mL.25Pathogenesis of extravasation injuries involve multiple factors, such as (1) volume of contrast extravasation, (2) increased osmolality associated with contrast, and (3) cytotoxic effect of contrast media. The literature shows ageneral trend toward more severe extravasation injuries with larger volumes of contrast material. The threshold for significant tissue injury from increased osmolality is estimated in the literature to be between 1.025 and 1.420mOsm/kg water.1 The higher the osmolality of the contrast, the more fluid isP.1135drawn into the injured tissue, resulting in greater subcutaneous edema. Thirdly, although use of low osmolalitynonionic contrast such as iopamidol 300 has decreased the morbidity associated with contrast extravasation,25 iodinated contrast media is still listed as a vesicant and can cause significant soft tissue injury that manifests as blistering, ulceration, and necrosis.The anatomy of the hand and forearm as it relates to the complications of contrast extravasation have not been definitively studied. Similarly, the pathophysiology of compartment syndrome in contrast extravasation has not been clearly established, presumably from the infrequency of this complication. Because the veins used in the extremity for IV access are superficial and proximal, direct infiltration of the muscle compartments or hand involvement is uncommon. It has been the authors' experience that most contrast extravasation injuries involve the subcutaneous tissue and not the muscular compartments. Some authors have suggested that the mechanism of compartment syndrome in contrast extravasation is subcutaneous edema that results in extrinsiccompression of the hand or forearm compartments.7 Usually, patient comorbidities such as collagen vascular disease and peripheral vascular disease are potentiating factors.In the workup of the patient with contrast extravasation, it is important to note the type of contrast given, the estimated volume extravasated, and the IV access site. The presence of collagen vascular disease, peripheral vascular disease, diabetes, and other comorbidities must be determined and documented. The presence of swelling of the forearm and hand, blistering, and erythema must be noted on examination. If compartment syndrome is a concern, the importance of a neurovascular examination and compartment pressure measurements cannot be overemphasized.The overwhelming majority of cases reported in the literature resolve without surgical intervention; conservative treatment, in the form of elevation, cold compresses, and interval neurovascular examinations during a period of observation for 24 hours is generally all that is required. However, early signs of compartment syndrome should be vigilantly assessed and the appropriate surgical compartment release performed.
REFERENCES
- Bellin MF, Jakobsen JA, Tomassin I, et al. Contrast medium extravasation injury: guidelines for prevention and management. Eur Radiol 2002;12(11):2807-2812.
- Bruner JM. The zig-zag volar-digital incision for flexor-tendon surgery. Plast Reconstr Surg 1967;40(6):571-574.
- Caddick JF, Rickard RF. A molten metal, high-pressure injection injury of the hand. J Hand Surg Br 2004;29(1):87-89.
- Chan BK, Tham SK, Leung M. Free toe pulp transfer for digital reconstruction after high-pressure injection injury. J Hand Surg Br 1999;24(5):534-538.
- Couzens G, Burke FD. Veterinary high pressure injection injuries with inoculations for larger animals. J Hand Surg Br 1995;20(4):497-499.
- del Pinal F, Herrero F, Jado E, et al. Acute thumb ischemia secondary to high-pressure injection injury: salvage by emergency decompression, radical debridement, and free hallux hemipulp transfer. J Trauma 2001;50(3):571-574.
- Fallscheer P, Kammer E, Roeren T, et al. Injury to the upper extremity caused by extravasation of contrast medium: a true emergency. Scand J Plast Reconstr Surg Hand Surg 2007;41(1):26-32.
- Fialkov JA, Freiberg A. High pressure injection injuries: an overview. J Emerg Med 1991;9(5):367-371.
- Gelberman RH, Posch JL, Jurist JM. High-pressure injection injuries of the hand. J Bone Joint Surg Am 1975;57(7):935-937.
- Gonzalez R, Kasdan ML. High pressure injection injuries of the hand. Clin Occup Environ Med 2006;5(2):407-411, ix.
- Gutowski KA, Chu J, Choi M, et al. High-pressure hand injection injuries caused by dry cleaning solvents: case reports, review of the literature, and treatment guidelines. Plast Reconstr Surg 2003;111(1):174-177.
- Hart RG, Smith GD, Haq A. Prevention of high-pressure injection injuries to the hand. Am J Emerg Med 2006;24(1):73-76.
- Hayes CW, Pan HC. High-pressure injection injuries to the hand. South Med J 1982;75(12):1491-1498, 1516.
- Hogan CJ, Ruland RT. High-pressure injection injuries to the upper extremity: a review of the literature. J Orthop Trauma 2006;20(7): 503-511.
- Kaufman HD. The anatomy of experimentally produced high-pressure injection injuries of the hand. Br J Surg 1968;55(5):340-344.
- Kaufman HD. The clinicopathological correlation of high-pressure injection injuries. Br J Surg 1968;55(3):214-218.
- Kon M, Sagi A. High-pressure water jet injury of the hand. J Hand Surg Am 1985;10(3):412-414.
- Lo SJ, Hughes J, Armstrong A. Non-infective subcutaneous emphysema of the hand secondary to a minor webspace injury. J Hand Surg Br 2005;30(5):482-483.
- Luber KT, Rehm JP, Freeland AE. High-pressure injection injuries of the hand. Orthopedics 2005;28(2):129-132.
- Macha DB, Nelson RC, Howle LE, et al. Central venous catheter integrity during mechanical power injection of iodinated contrast medium. Radiology 2009;253(3):870-878.
- Malenfant J, Walters A, Kralovic S, et al. Francesco Parona (1842-1908) and his contributions to ourunderstanding of surgery through anatomy. Clin Anat 2013;26(5):547-550.
- Neal NC, Burke FD. High-pressure injection injuries. Injury 1991;22(6):467-470.
- O'Reilly RJ, Blatt G. Accidental high-pressure injection-gun injuries of the hand; the role of the emergency radiologic examination. J Trauma 1975;15(1):24-31.
- Pinto MR, Turkula-Pinto LD, Cooney WP, et al. High-pressure injection injuries of the hand: review of 25 patients managed by open wound technique. J Hand Surg Am 1993;18(1):125-130.
- Sbitany H, Koltz PF, Mays C, et al. CT contrast extravasation in the upper extremity: strategies for management. Int J Surg 2010;8(5): 384-386.
- Schnall SB, Mirzayan R. High-pressure injection injuries to the hand. Hand Clin 1999;15(2):245-248, viii.
- Schoo MJ, Scott FA, Boswick JA Jr. High-pressure injection injuries of the hand. J Trauma 1980;20(3):229-238.
- Sirio CA, Smith JS Jr, Graham WP III. High-pressure injection injuries of the hand. A review. Am Surg 1989;55(12):714-718.
- Stark HH, Ashworth CR, Boyes JH. Paint-gun injuries of the hand. J Bone Joint Surg Am 1967;49(4):637-647.
- Temple CL, Richards RS, Dawson WB. Pneumomediastinum after injection injury to the hand. Ann Plast Surg 2000;45(1):64-66.
- Vasilevski D, Noorbergen M, Depierreux M, et al. High-pressure injection injuries to the hand. Am J Emerg Med 2000;18(7):820-824.
- Wieder A, Lapid O, Plakht Y, et al. Long-term follow-up of high-pressure injection injuries to the hand. Plast Reconstr Surg 2006;117(1):186-189.
- Wilson BG. Contrast media-induced compartment syndrome. Radiol Technol 2011;83(1):63-77.
