Masterclass: Corrective Surgery for Pediatric Cavus Foot Deformity

Key Takeaway
This masterclass guides fellows through the comprehensive surgical treatment of pediatric cavus foot deformity. We'll meticulously cover preoperative planning, patient positioning, detailed surgical anatomy, and real-time, step-by-step intraoperative execution of various corrective procedures including plantar fascia release, osteotomies, and tendon transfers. Emphasis is placed on neurovascular protection, instrument precision, and managing potential pitfalls to achieve a plantigrade, mobile, and balanced foot. Postoperative rehabilitation and complication management are also thoroughly discussed.
The surgical correction of a significant pediatric cavus foot deformity represents one of the most challenging, yet profoundly rewarding, endeavors in orthopedic surgery. This pathology demands far more than technical proficiency in osteotomies and tendon transfers; it requires an exhaustive understanding of complex foot biomechanics, the underlying neuromuscular pathology, and the meticulous restoration of dynamic function. The ultimate objective is invariant: to achieve a mobile, plantigrade, and well-balanced foot that can withstand the repetitive stresses of ambulation without progressive deterioration or ulceration.
The pathophysiologic cascade of the cavovarus deformity necessitates a systematic, stepwise surgical algorithm. In the pediatric population, the stakes are particularly high, as the developing skeleton is highly responsive to abnormal mechanical forces. Failure to address the primary deforming vectors will inevitably lead to structural adaptations, rendering a flexible deformity rigid and necessitating joint-sacrificing salvage procedures later in life. This masterclass chapter delineates the definitive approach to evaluating and surgically managing the pediatric cavus foot.
Comprehensive Introduction and Patho-Epidemiology
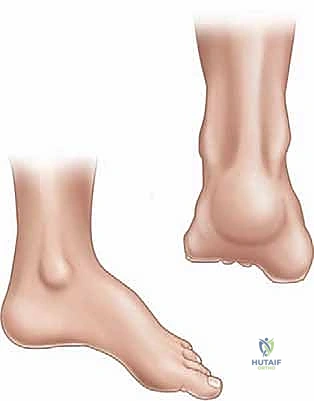
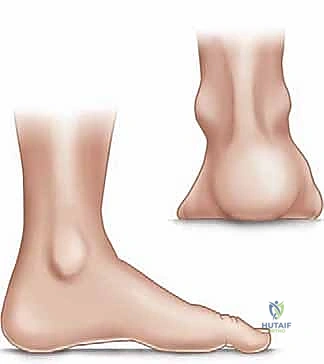
A cavus foot deformity in children is clinically characterized by an abnormally high medial longitudinal arch that persists rigidly even under full weight-bearing conditions. This architectural distortion is rarely an isolated structural anomaly; rather, it is predominantly the terminal manifestation of a profound neuromuscular imbalance. This imbalance invariably leads to a constellation of secondary deformities, including forefoot pronation, hindfoot varus, and complex clawing of the digits.

While the underlying etiology can occasionally be idiopathic, the overwhelming majority of bilateral cavovarus feet in the pediatric population are driven by an identifiable neurological disorder. Hereditary Sensory Motor Neuropathies (HSMN), particularly Charcot-Marie-Tooth (CMT) disease, account for the most significant percentage of these presentations. In CMT, the pathogenesis is characterized by a highly specific, length-dependent peripheral neuropathy. We observe early, progressive atrophy of the intrinsic muscles of the foot—often remarkably sparing the abductor hallucis—alongside selective involvement of the extrinsic musculature.
The hallmark of the CMT cavus foot is the dominance of the peroneus longus over an increasingly paretic tibialis anterior. Advanced magnetic resonance imaging and dynamic electromyographic studies have unequivocally demonstrated this specific vector mismatch. Similarly, the posterior tibialis retains its strength and overpowers the weakening peroneus brevis, driving the hindfoot into rigid varus. Understanding this specific pattern of muscle preservation and denervation is the absolute foundation upon which all reconstructive surgical planning must be based.
Beyond HSMN, the differential diagnosis for a pediatric cavus foot includes spinal dysraphism, tethered cord syndrome, diastematomyelia, poliomyelitis, Friedreich’s ataxia, and cerebral palsy. The natural history of the deformity is inextricably linked to its etiology. In progressive conditions like CMT, the foot transitions predictably from a flexible, dynamically driven posture to a rigid, structurally fixed deformity as adaptive shortening of the soft tissues and secondary osseous remodeling occur. Early surgical intervention, strategically timed before the onset of rigid bony adaptation, is therefore paramount to preserving joint mobility and preventing the need for future triple arthrodesis.
Detailed Surgical Anatomy and Biomechanics
Before initiating any surgical incision, a profound, three-dimensional understanding of foot anatomy and biomechanics is mandatory. The architecture of the foot must be viewed not as a static structure, but as a dynamic, load-bearing lever arm. Surgical intervention is essentially an exercise in biomechanical re-engineering.
The Plantar Fascia and Arch Mechanics
The plantar fascia is an extensive, remarkably dense aponeurotic structure originating from the medial process of the calcaneal tuberosity. As it courses distally, it fans out into five distinct slips that insert into the plantar plates and transverse metatarsal ligaments at the metatarsal heads. Its primary biomechanical role is to stabilize the longitudinal arch of the foot and to provide a critical protective shield for the underlying neurovascular structures of the plantar vault.
During the normal gait cycle, the plantar fascia acts as a dynamic tension band. At heel strike, the foot must act as a mobile adaptor; forefoot supination and heel inversion occur as the quadriceps eccentrically absorb impact energy. Mid-stance involves the unlocking of the transverse tarsal joints (talonavicular and calcaneocuboid), allowing hindfoot pronation and internal tibial rotation to accommodate uneven terrain.
At terminal stance and toe-off, the plantar fascia engages in the critical "windlass effect," originally described by Hicks. As the metatarsophalangeal (MTP) joints passively dorsiflex over the fixed forefoot, the plantar fascia is pulled distally and tightens around the metatarsal heads. This action draws the calcaneus toward the metatarsal heads, elevating the medial longitudinal arch, inverting the hindfoot, and locking the midtarsal joints. This effectively transforms the foot from a flexible shock absorber into a rigid lever arm essential for forward propulsion.

In the cavus foot, this windlass mechanism is pathologically exaggerated. The chronically plantarflexed first ray and contracted plantar fascia maintain the foot in a constant state of rigid elevation, contributing directly to the claw toe deformities and eliminating the foot's ability to absorb shock during early stance phase.
Muscular Imbalance and Neuromuscular Considerations
The architectural collapse in a cavus foot is driven by specific, predictable muscular mismatches. Weakness of the intrinsic foot muscles (lumbricals and interossei) eliminates the primary flexors of the MTP joints and extensors of the interphalangeal (IP) joints. Consequently, the unopposed pull of the extensor digitorum longus (EDL) hyperextends the MTP joints, while the flexor digitorum longus (FDL) and flexor hallucis longus (FHL) hyperflex the IP joints, resulting in rigid claw toes.
The peroneus longus, innervated by the superficial peroneal nerve, originates from the lateral fibula and inserts onto the plantar aspect of the medial cuneiform and first metatarsal base. Its primary function is to plantarflex the first ray and evert the foot. In HSMN, the peroneus longus typically retains its strength long after its primary antagonist, the tibialis anterior (deep peroneal nerve), has weakened. This unopposed force drives the first metatarsal into fixed plantarflexion, creating a forefoot-driven cavus.
Simultaneously, the posterior tibialis (tibial nerve), a powerful invertor and plantarflexor, often overpowers a weakening peroneus brevis (superficial peroneal nerve). The peroneus brevis normally acts to evert the hindfoot and counteract the posterior tibialis. When this balance is lost, the hindfoot is pulled into a rigid varus posture. Understanding these specific vector imbalances dictates our choice of tendon transfers, such as the peroneus longus to peroneus brevis transfer, which eliminates the deforming plantarflexion force on the first ray while simultaneously augmenting hindfoot eversion.
Osteology and the Tripod Effect
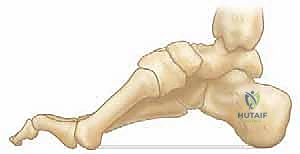
The bony architecture of the cavus foot is characterized by complex, multiplanar deformities. The hallmark is the rigidly plantarflexed first metatarsal. When the patient bears weight, this plantarflexed medial column strikes the ground prematurely. To accommodate this, the hindfoot is forced into a compensatory varus position. This phenomenon is known as the "tripod effect," where weight-bearing is pathologically concentrated on three points: the calcaneal tuberosity, the first metatarsal head, and the fifth metatarsal head.
Because the medial column is driven downward, the heel is forced into varus to allow the lateral border of the foot to contact the floor. This creates a rigid, unyielding lever throughout the entire stance phase. The lack of shock absorption leads to significantly increased contact stresses, intractable pain, and the development of thick, painful callosities under the first and fifth metatarsal heads, and along the lateral border of the foot.
The apex of the deformity must be precisely identified, as it dictates the anatomical level of surgical correction. The apex may be located in the forefoot (localizing to the first tarsometatarsal joint), the midfoot (naviculocuneiform or talonavicular joints), or the hindfoot (calcaneus). Accurate localization is achieved through meticulous clinical examination and radiographic templating, ensuring that osteotomies are performed at the true center of rotation of angulation (CORA).
Critical Neurovascular Structures
Surgical reconstruction of the cavus foot involves extensive soft tissue releases and multiple osteotomies, requiring intimate knowledge of the regional neurovascular anatomy to prevent catastrophic complications. During the medial approach for plantar fascia release (Steindler stripping), the medial plantar nerve and artery are at significant risk. These structures run immediately deep and slightly lateral to the abductor hallucis muscle belly. The deep fascia of the abductor hallucis must be carefully incised and the muscle retracted dorsally to protect the neurovascular bundle before releasing the plantar fascia from the calcaneus.
When addressing the hindfoot via a lateral approach for a calcaneal osteotomy, the sural nerve and the lesser saphenous vein must be identified and protected. The sural nerve courses superficially along the lateral aspect of the hindfoot, crossing the planned osteotomy site. Deep to the subcutaneous tissues, the peroneal tendons (longus and brevis) lie within their synovial sheath and must be mobilized and protected superiorly.
Dorsal approaches for midfoot osteotomies or the Jones procedure demand careful management of the superficial and deep peroneal nerves. Branches of the superficial peroneal nerve provide sensory innervation to the dorsum of the foot and are easily injured during skin incision and superficial dissection. The deep peroneal nerve and the dorsalis pedis artery run together in the first intermetatarsal space and must be identified and gently retracted when performing a first metatarsal dorsiflexion osteotomy or routing the extensor hallucis longus (EHL) tendon.
Exhaustive Indications and Contraindications
The decision to proceed with surgical reconstruction in a pediatric patient with a cavus foot deformity requires a nuanced assessment of the patient's symptoms, the flexibility of the deformity, the underlying diagnosis, and the anticipated natural history of the disease. The primary goal is to perform joint-sparing procedures (osteotomies and tendon transfers) before the deformity becomes rigidly fixed and arthritic, which would otherwise necessitate joint-sacrificing arthrodesis.
Surgical intervention is generally indicated when a patient presents with a progressive deformity that is no longer amenable to conservative management. This includes patients who have failed orthotic management (such as AFOs or custom insoles) and continue to experience intractable pain, recurrent ankle instability, or progressive difficulty with ambulation. The presence of recurrent, pre-ulcerative callosities under the first metatarsal head, fifth metatarsal base, or lateral border of the foot is a strong indication for surgical offloading.
Furthermore, a rapid progression of the deformity, particularly in the setting of a known neuromuscular disorder like CMT, warrants early surgical intervention. In these cases, the goal is to rebalance the foot dynamically while the joints remain supple. Delaying surgery until the joints become rigid significantly compromises the functional outcome and limits the surgeon's reconstructive options.
| Parameter | Surgical Indications | Surgical Contraindications |
|---|---|---|
| Clinical Presentation | Progressive pain, recurrent lateral ankle sprains, frequent tripping, inability to tolerate orthotics. | Asymptomatic, mild, non-progressive deformity easily managed with supportive footwear. |
| Soft Tissue Status | Intractable plantar callosities, pre-ulcerative lesions, progressive clawing of digits. | Active, untreated deep space infection or severe, unmanageable plantar ulceration (relative). |
| Deformity Flexibility | Flexible hindfoot (corrects on Coleman block test), supple midtarsal joints. | Rigid, arthritic joints in an older adolescent (indicates need for arthrodesis rather than joint-sparing osteotomies). |
| Neurological Status | Documented progression of muscle imbalance in HSMN or stable deficit in CP/Polio. | Rapidly progressive, undiagnosed neurological decline lacking a definitive workup. |
| Vascular Status | Intact pedal pulses, good capillary refill. | Severe peripheral vascular disease precluding adequate wound healing (rare in pediatrics, but critical to assess). |
Contraindications to joint-sparing corrective surgery include a completely rigid, arthritic foot in an older adolescent or young adult, where a triple arthrodesis may be the only viable salvage option. Additionally, surgery should be delayed in patients with an undiagnosed, rapidly progressive neurological condition until a definitive diagnosis and neurological baseline are established. Active infection or severe vascular compromise are absolute contraindications to elective reconstruction.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the absolute cornerstone of a successful surgical outcome. The cavus foot is a complex, three-dimensional deformity, and a generic surgical approach will inevitably lead to undercorrection or iatrogenic secondary deformities.
Clinical Evaluation and Diagnostic Workup
The clinical evaluation begins with a meticulous assessment of the deformity's flexibility. The Coleman Block Test is the single most critical physical examination maneuver in the evaluation of a cavovarus foot. It differentiates a flexible, forefoot-driven hindfoot varus from a fixed, rigid hindfoot varus. The patient is asked to stand with the lateral border of the foot (heel and lateral metatarsals) on a 1-inch wooden block, allowing the plantarflexed first metatarsal to hang freely off the medial edge.
If the hindfoot varus corrects to a neutral or valgus alignment when the first ray drops, the hindfoot is deemed flexible. This confirms that the primary driver of the deformity is the plantarflexed medial column, and surgical correction should focus on elevating the first ray (e.g., first metatarsal osteotomy) and releasing the plantar fascia. Conversely, if the hindfoot remains in varus despite offloading the first ray, the hindfoot deformity is fixed, dictating the absolute necessity of a calcaneal osteotomy to physically realign the heel.
A comprehensive neurological examination is mandatory. Muscle strength testing must systematically isolate the tibialis anterior, peroneus longus, peroneus brevis, posterior tibialis, and the triceps surae. The spine must be examined for scoliosis, kyphosis, or cutaneous stigmata of spinal dysraphism (hairy patches, dimples). In a pediatric patient presenting with bilateral cavus feet without a known family history, a referral to a pediatric neurologist for EMG/NCS and genetic testing is highly recommended prior to surgical intervention.
Radiographic Analysis and Templating
Standard weight-bearing anteroposterior (AP) and lateral radiographs of the foot and ankle are essential for preoperative templating. On the lateral radiograph, Meary's angle (the angle between the longitudinal axis of the talus and the longitudinal axis of the first metatarsal) is measured. In a normal foot, this angle is 0 degrees. In a cavus foot, the angle is significantly increased, with the apex pointing dorsally. The location of the apex (tarsometatarsal, naviculocuneiform, or talonavicular) dictates the site of the corrective midfoot osteotomy.


The calcaneal pitch angle, measured between a line along the plantar surface of the calcaneus and the horizontal weight-bearing surface, helps differentiate between different types of cavus. An abnormally high calcaneal pitch (greater than 30 degrees) indicates a calcaneocavus deformity, often associated with triceps surae weakness (e.g., poliomyelitis or over-lengthened Achilles). The Hibbs angle (angle between the longitudinal axis of the calcaneus and the first metatarsal) further quantifies the severity of the longitudinal arch elevation.
Patient Positioning and Anesthesia
The procedure is typically performed under general anesthesia with a regional nerve block (popliteal and saphenous) for postoperative pain control. The patient is positioned supine on the operating table. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the lateral border of the foot and ankle into a strictly vertical position, which greatly facilitates the lateral approach to the calcaneus.
A well-padded thigh tourniquet is applied to ensure a bloodless surgical field. The entire lower extremity from the toes to the mid-thigh is prepped and draped in a standard sterile fashion. A sterile marking pen is used to outline all planned incisions, bony landmarks, and the course of major neurovascular structures before exsanguination and tourniquet inflation.
Step-by-Step Surgical Approach and Fixation Technique
The surgical reconstruction of the pediatric cavus foot must follow a logical, stepwise progression. The "a la carte" approach dictates that the surgeon addresses the specific components of the deformity in a sequential manner, reassessing the foot's alignment after each step. The standard sequence is: soft tissue release, forefoot/midfoot bony correction, hindfoot bony correction, and finally, tendon transfers.
Soft Tissue Releases: The Steindler Stripping
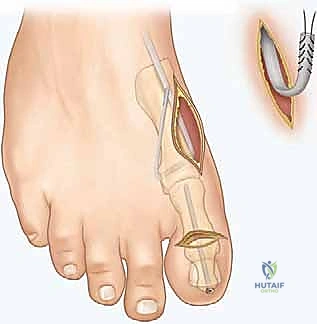
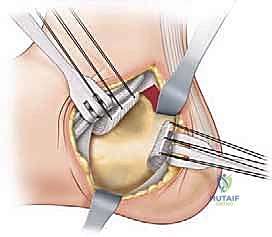
The initial step in almost all cavus foot reconstructions is the release of the contracted plantar fascia and intrinsic musculature, classically known as the Steindler stripping. A 3 to 4 cm longitudinal incision is made along the medial aspect of the calcaneus, just superior to the plantar fat pad.

Blunt dissection is carried down to the deep fascia of the abductor hallucis. This fascia is incised longitudinally, and the muscle belly is elevated dorsally using a Chandler retractor. This maneuver is critical to protect the medial plantar nerve and artery, which lie immediately deep to the muscle. Once the neurovascular bundle is secured, an elevator or heavy scissors is used to strip the origin of the plantar fascia, the short flexors, and the abductor digiti minimi directly off the medial, plantar, and lateral aspects of the calcaneal tuberosity. A thorough release will result in an immediate, palpable softening of the longitudinal arch.
Bony Reconstructions: Forefoot and Midfoot
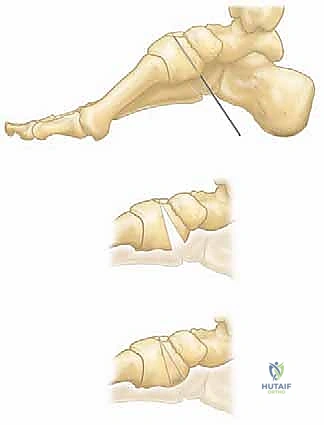
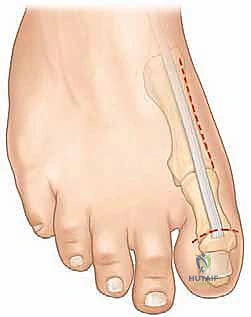
If the primary apex of the deformity is at the first tarsometatarsal joint, a dorsiflexion osteotomy of the first metatarsal base is performed. A dorsal longitudinal incision is made over the proximal first metatarsal. The EHL tendon is retracted laterally. A closing wedge osteotomy, with the base directed dorsally, is performed approximately 1 to 1.5 cm distal to the tarsometatarsal joint capsule.


The plantar cortex is carefully preserved to act as a hinge. The wedge of bone is removed, and the osteotomy is closed, elevating the metatarsal head out of its plantarflexed position. Fixation is typically achieved with crossed Kirschner wires (K-wires), a dorsal staple, or a low-profile plate and screw construct.


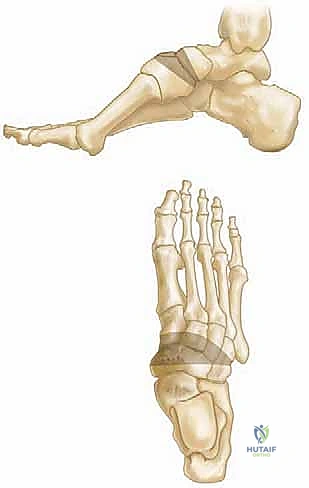
For more severe midfoot cavus deformities with the apex at the naviculocuneiform joint, a truncated wedge osteotomy (Cole procedure) or a V-osteotomy (Japas procedure) through the midfoot may be necessary. These procedures are technically demanding, requiring precise saw cuts through the midtarsal bones to shorten the dorsal column and elevate the arch, followed by rigid internal fixation with staples or plates.
Bony Reconstructions: Hindfoot
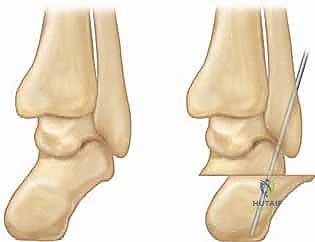
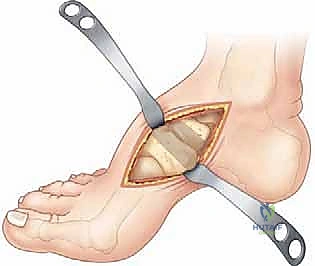
If the Coleman block test demonstrated a fixed hindfoot varus, a calcaneal osteotomy is mandatory. The two most common techniques are the Dwyer closing wedge osteotomy and the lateralizing calcaneal slide osteotomy.

An oblique incision is made over the lateral aspect of the calcaneus, posterior to the sural nerve and peroneal tendons. The periosteum is elevated, and Hohmann retractors are placed dorsally and plantarly. For a Dwyer osteotomy, a laterally based wedge of bone is removed from the posterior tuberosity, and the osteotomy is closed to correct the varus.