SURGICAL PROBLEMS RELATIVE TO SPECIFIC HIP DISORDERS
Extensive clinical data and biomechanical research have accumulated since the 1970s concerning the diverse pathologies for which total hip arthroplasty (THA) is indicated. While the fundamental principles of THA remain consistent, routine surgical techniques must frequently be modified to address the unique pathoanatomy and biomechanical deficits associated with specific conditions. A nuanced understanding of these entities is mandatory for the reconstructive arthroplasty surgeon to optimize implant survivorship, restore joint kinematics, and minimize perioperative complications.
ARTHRITIC DISORDERS
Osteoarthritis (Primary and Secondary)
Osteoarthritis (OA), whether primary (idiopathic) or secondary to previous trauma, dysplasia, or childhood hip disorders (e.g., Legg-Calvé-Perthes disease, Slipped Capital Femoral Epiphysis), remains the most common indication for total hip arthroplasty.
Pathoanatomy and Clinical Presentation
Patients typically present with a slightly shortened extremity, though discrepancies can exceed 1 cm if severe erosion or deformation of the femoral head or acetabulum has occurred. The hip is frequently contracted in flexion, external rotation, and adduction, which exacerbates the apparent limb length discrepancy.
Surgical Approach and Dislocation
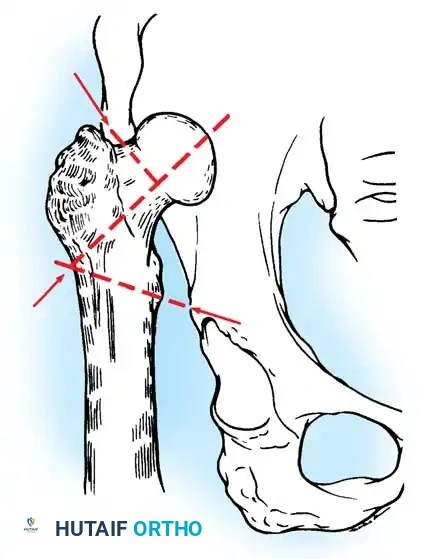
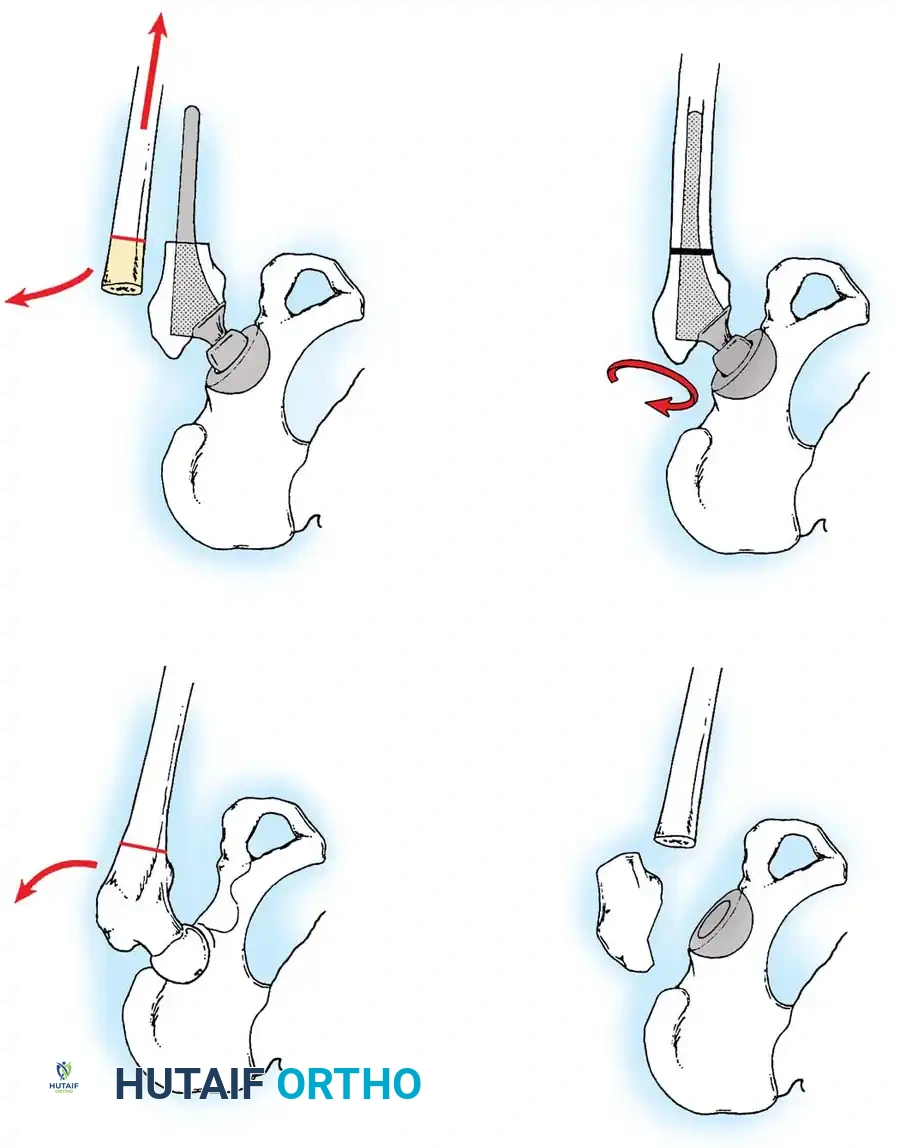
Safe dislocation of the hip is the first critical step. In advanced OA, massive marginal osteophytes often tether the femur within the acetabulum.
Surgical Warning: Never forcefully lever the femur to achieve dislocation in the presence of massive osteophytes. This places the patient at high risk for iatrogenic femoral neck or shaft fractures. Instead, perform a meticulous in situ resection of the anterior and posterior acetabular osteophytes prior to attempting dislocation. In severe cases, an in situ femoral neck osteotomy is the safest approach.
Acetabular Preparation
The subchondral bone in osteoarthritic acetabula is characteristically thick, sclerotic, and eburnated. Considerable reaming with sharp, hemispherical reamers is required to bypass this sclerotic layer and reach a bleeding cancellous bed satisfactory for biologic bone ingrowth.
Osteophytes may completely obliterate the cotyloid fossa (pulvinar), obscuring the true medial wall. If the femoral head has subluxated laterally, inferior intra-articular osteophytes can thicken the bone significantly, creating a "false bottom." The surgeon must deepen the acetabulum to its true anatomic medial wall to fully contain the cup.

Failure to medialize the acetabulum leaves the superior portion of the cup unsupported or resting on structurally inferior osteophytic bone rather than the solid iliac column. Furthermore, careful excision of all peripheral acetabular osteophytes is mandatory to prevent postoperative bony impingement, which can lead to decreased range of motion, accelerated polyethylene wear, and instability.
Femoral Preparation
While a formal trochanteric osteotomy is rarely necessary for primary OA, the greater trochanter is often hypertrophied. Trimming the anterior or posterior overhang of the trochanter may be required to prevent extra-articular impingement during internal and external rotation.
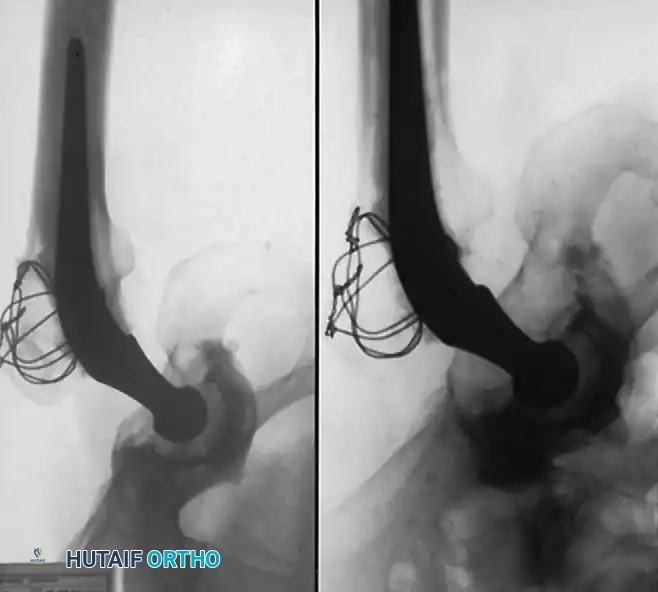
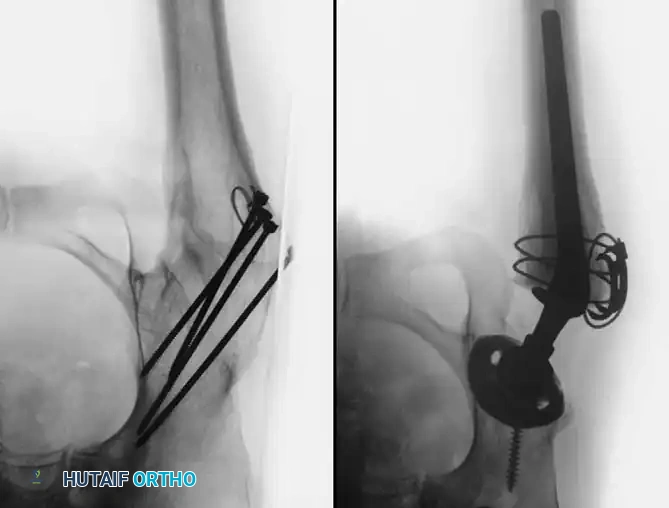
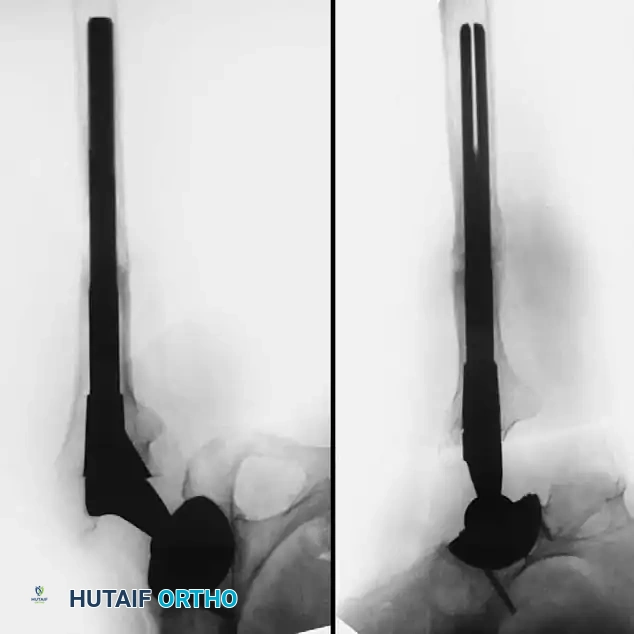
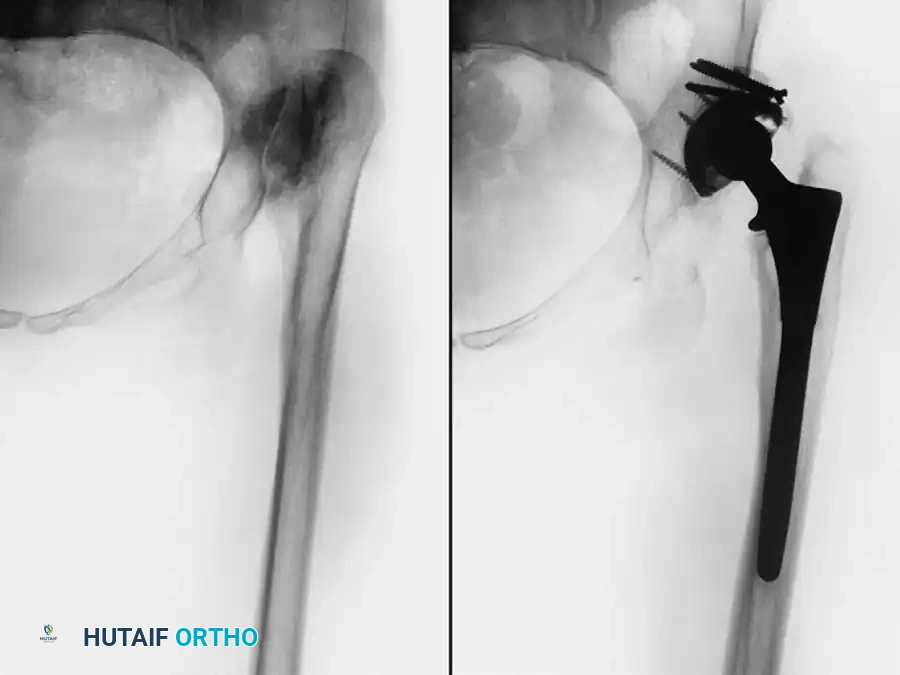
Radiographic Case Examples: Osteoarthritis and Complex Reconstructions
The following imaging series demonstrates various stages of complex acetabular and femoral preparation, highlighting the necessity of restoring offset and center of rotation.


Rheumatoid Arthritis and Inflammatory Arthropathies
Total hip arthroplasty is highly effective for relieving pain and restoring mobility in patients with rheumatoid arthritis (RA), chronic juvenile idiopathic arthritis (JIA/Still's disease), psoriatic arthritis, and systemic lupus erythematosus (SLE). Bilateral involvement is common, and these patients present unique systemic and local challenges.
Preoperative Considerations
RA patients are often profoundly disabled, presenting with poor musculature, fragile skin, vasculitis, and severe osteopenia. Chronic use of corticosteroids and disease-modifying antirheumatic drugs (DMARDs) increases the risk of perioperative infection and poor wound healing.
Clinical Pearl: Cervical spine instability is a critical concern. Radiographic evidence of cervical instability is present in up to 61% of RA patients undergoing THA, though half are asymptomatic. Preoperative flexion and extension cervical radiographs are mandatory. Fiberoptic intubation techniques are frequently required to prevent catastrophic neurologic injury during anesthesia induction.
Intraoperative Challenges
The femoral head is often partially resorbed due to inflammatory erosion or secondary osteonecrosis, and varying degrees of protrusio acetabuli are common.
Special handling of the limb is paramount. The osteopenic bone is highly susceptible to iatrogenic fracture. Retractors must be placed with extreme care; levering the femur anteriorly with a Hohmann retractor can easily fracture the anterior acetabular margin or the femoral neck.
Implant Selection and Fixation
Preparation of the femur is usually straightforward due to a widened medullary canal (Dorr Type C "stovepipe" femur), but the cortices are paper-thin and easily penetrated. The acetabulum is similarly soft, and the medial wall is easily breached during reaming.
While severe osteopenia historically favored cemented fixation, contemporary highly porous cementless components have shown excellent survivorship in RA patients. In patients with JIA, the skeleton is often underdeveloped, necessitating custom or ultra-small components. Excessive femoral anteversion and anterior bowing of the proximal femur are also common in JIA, occasionally requiring a concomitant femoral osteotomy.
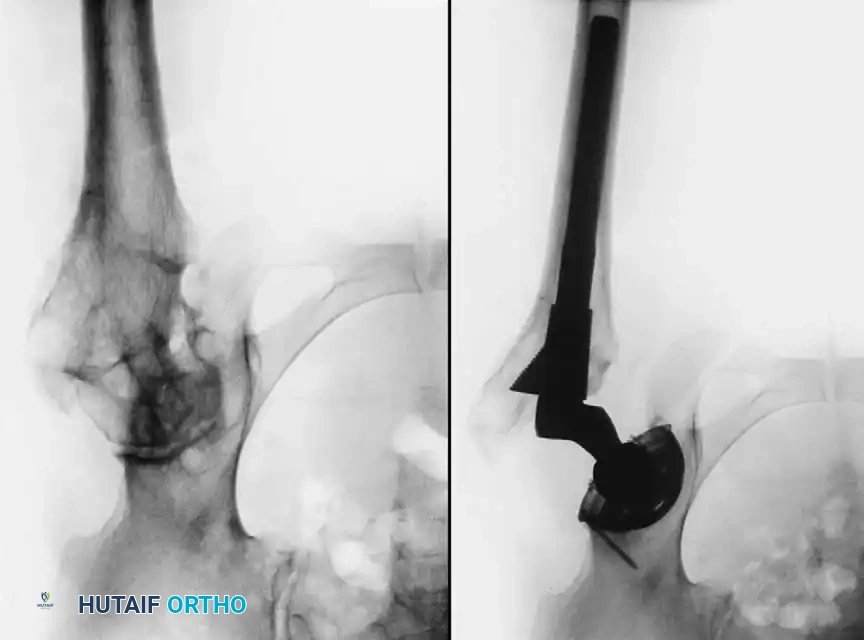
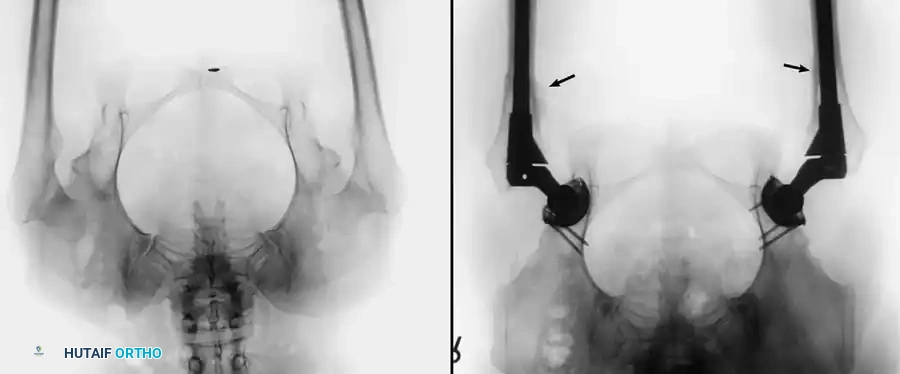
Radiographic Case Examples: Inflammatory Arthropathy and Osteopenia Management


OSTEONECROSIS (AVASCULAR NECROSIS)
Osteonecrosis of the femoral head presents a complex challenge regarding both joint preservation and arthroplasty. Etiologies include corticosteroid use, alcohol abuse, trauma, sickle cell disease, Gaucher disease, and caisson disease, though many cases remain idiopathic.
Indications and Alternatives
In early stages (Ficat Stages I and II) without subchondral collapse, joint-preserving procedures such as core decompression, vascularized fibular grafting, or proximal femoral osteotomies may be indicated. However, once subchondral collapse and secondary degenerative changes occur, THA is the treatment of choice.
Historically, THA in young patients with osteonecrosis yielded inferior results compared to older OA cohorts, largely due to first-generation cementing techniques and high activity levels. However, contemporary cementless implants with highly cross-linked polyethylene or ceramic-on-ceramic bearings have drastically improved long-term survivorship in this demographic.
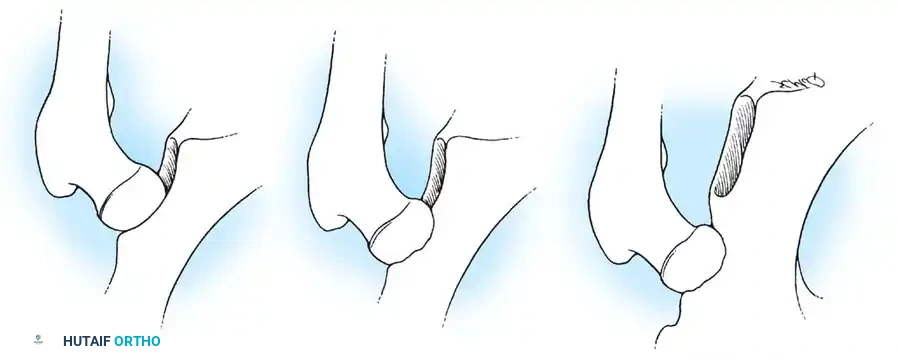
Surgical Technique and Prior Graft Management
Upon capsulotomy, the surgeon will often encounter a highly hyperemic capsule and profound synovial proliferation. A large synovial effusion is common and should not immediately be mistaken for infection, though routine cultures are prudent. Meticulous hemostasis is required.
Pitfall: If the patient has previously undergone a cortical bone grafting procedure (e.g., free or vascularized fibular graft), the intramedullary portion of the graft must be completely excised. Conventional broaches will deflect off the hard cortical graft, leading to varus malpositioning and undersizing of the femoral component.
To safely remove prior grafts, the surgeon should utilize a high-speed burr and flexible reamers. Intraoperative fluoroscopy with the broach in place is highly recommended to ensure complete graft removal, proper alignment, and optimal cortical contact.
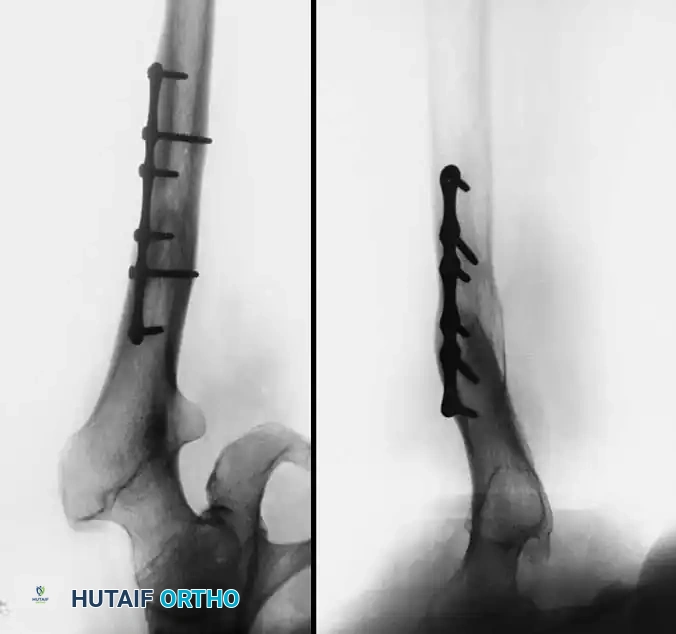
Radiographic Case Examples: Osteonecrosis and Complex Femoral Reconstructions




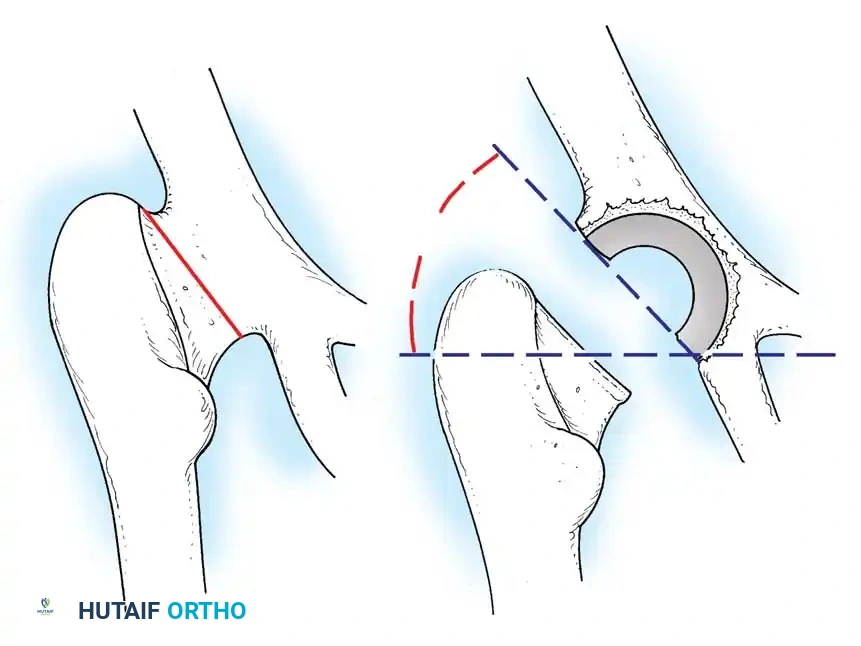
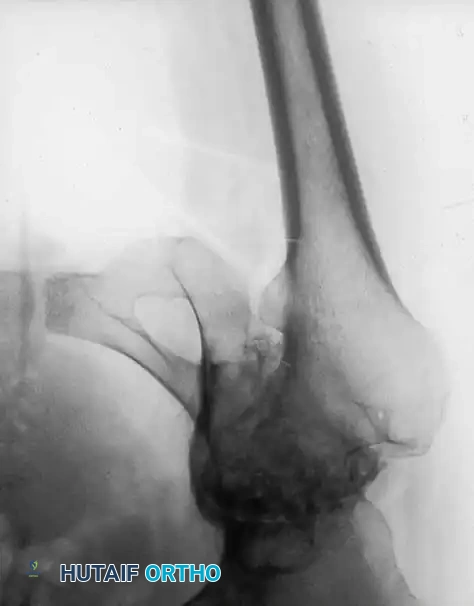
PROTRUSIO ACETABULI
Intrapelvic protrusio acetabuli is defined radiographically by the medial migration of the femoral head beyond the ilioischial (Kohler) line.
Classification
1. Primary Protrusio (Arthrokatadysis / Otto Pelvis): Typically bilateral, occurs in younger females, and leads to severe restriction of motion at an early age.
2. Secondary Protrusio: Results from conditions such as rheumatoid arthritis, ankylosing spondylitis, Paget disease, Marfan syndrome, osteomalacia, trauma (central fracture-dislocation), or migration of a previous endoprosthesis.

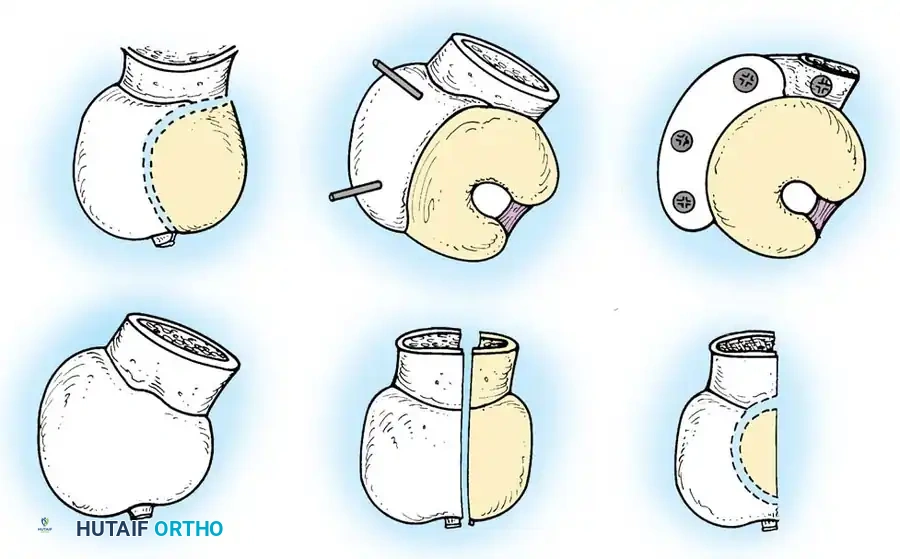
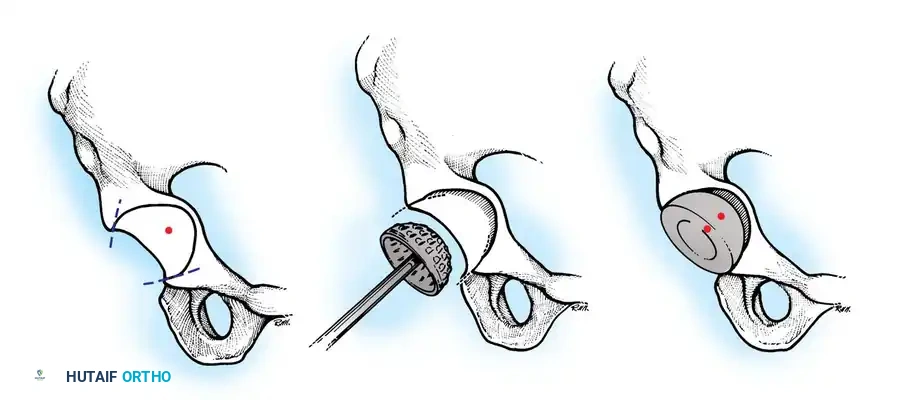
Principles of Reconstruction
The surgical management of protrusio acetabuli is technically demanding and relies on three non-negotiable biomechanical principles:
1. Restoration of the Anatomic Hip Center: The hip center of rotation must be lateralized and brought inferiorly to its true anatomic position to restore abductor mechanics and minimize joint reactive forces.
2. Peripheral Rim Fixation: The implant must be supported by the intact, structurally sound peripheral rim of the acetabulum, bypassing the deficient medial wall.
3. Medial Wall Reconstruction: Cavitary and segmental defects of the medial wall must be reconstituted, typically utilizing impaction bone grafting (autograft from the resected femoral head or allograft).

Surgical Technique
Due to the medial migration of the femur, the sciatic nerve is drawn closer to the joint than normal. It
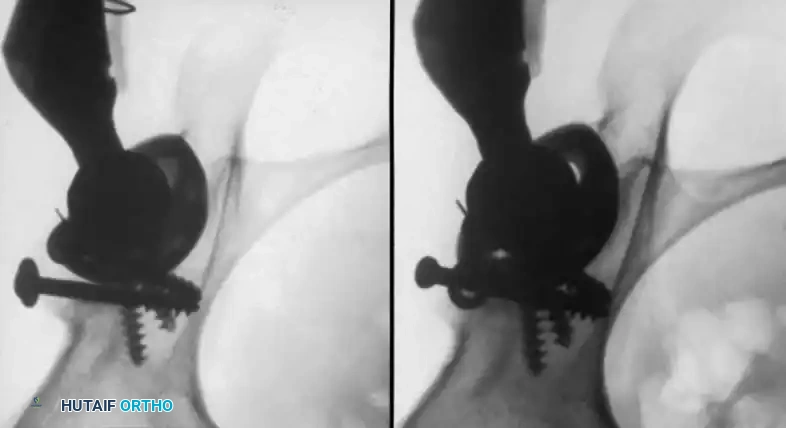
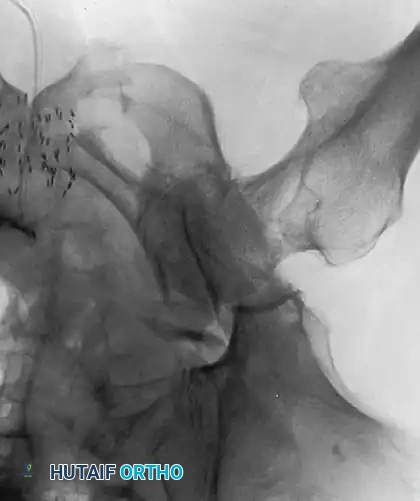
Associated Surgical & Radiographic Imaging