Superior Glenohumeral Dislocation Mechanism: Injury to Recovery Guide
Introduction & Epidemiology
Superior glenohumeral dislocation is an exceedingly rare and complex injury, constituting less than 1% of all shoulder dislocations. This stands in stark contrast to the vastly more common inferior (anterior or posterior) glenohumeral dislocations. The injury typically results from a high-energy mechanism, often an extreme anterior and superiorly directed force applied to an adducted upper extremity. Common scenarios include falls from a height onto the adducted arm, direct blows to the shoulder, or motor vehicle collisions. This unique mechanism forces the humeral head superiorly from the glenoid fossa, frequently impacting or fracturing the acromion, coracoid, or superior glenoid rim.
Due to the significant forces involved and the inherent stability of the superior shoulder girdle structures (coracoacromial arch, superior capsule, coracohumeral ligament, and superior glenohumeral ligament), superior glenohumeral dislocations are often accompanied by a spectrum of severe associated injuries. These include fractures of the acromion, clavicle (especially the distal clavicle), coracoid process, humeral tuberosities (greater and lesser), and glenoid rim. Furthermore, concomitant injuries to the acromioclavicular (AC) joint, rotator cuff, and brachial plexus are not uncommon, significantly influencing prognosis and treatment strategies. The rarity of this injury often leads to delayed diagnosis or misdiagnosis, highlighting the critical need for a high index of suspicion among clinicians.
Surgical Anatomy & Biomechanics
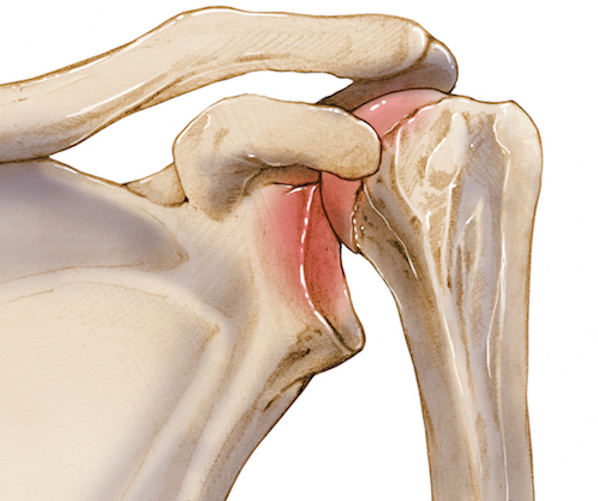
A thorough understanding of the surgical anatomy and biomechanics of the shoulder girdle is paramount in managing superior glenohumeral dislocations. The glenohumeral joint is a ball-and-socket articulation, inherently unstable due to the shallow glenoid fossa articulating with the larger humeral head. Stability is primarily provided by both static and dynamic stabilizers.
Static Stabilizers:
*
Glenoid Labrum:
A fibrocartilaginous rim that deepens the glenoid fossa, enhancing congruity. Superior dislocations often result in labral tears, particularly superior labral anterior-posterior (SLAP) lesions or detachment of the biceps anchor.
*
Joint Capsule:
A fibrous sac surrounding the joint, reinforced by glenohumeral ligaments. The superior capsule and coracohumeral ligament are crucial in preventing superior translation of the humeral head.
*
Glenohumeral Ligaments (SGHL, MGHL, IGHL):
The Superior Glenohumeral Ligament (SGHL) and Coracohumeral Ligament (CHL) are particularly relevant, acting as primary restraints to superior translation of the humeral head in adduction. Injury to these structures is integral to the dislocation mechanism.
*
Coracoacromial Arch:
Formed by the coracoid process, the coracoacromial ligament, and the acromion. This robust bony and ligamentous arch typically acts as a superior barrier, making superior dislocation challenging without disruption of this arch or significant humeral head deformation/fracture. Impaction of the humeral head against the coracoacromial arch or fractures of these components are common in superior dislocations.
Dynamic Stabilizers:
*
Rotator Cuff Muscles (Supraspinatus, Infraspinatus, Teres Minor, Subscapularis):
These muscles provide compressive forces across the joint, actively stabilizing the humeral head within the glenoid. Tears of the rotator cuff, particularly the supraspinatus, are frequently observed due to the violent superior displacement.
*
Biceps Tendon (Long Head):
Originating from the superior glenoid tubercle and labrum, its course over the humeral head and through the bicipital groove can be disrupted, displaced, or torn.
Neurovascular Structures:
The proximity of critical neurovascular structures necessitates meticulous evaluation. The
brachial plexus
lies in close proximity, with the
axillary nerve
being particularly vulnerable as it courses inferiorly around the surgical neck of the humerus, but also during superior displacement due to traction. The
axillary artery and vein
are situated anteriorly and inferiorly, at risk of injury from direct trauma or stretching.
The biomechanical mechanism typically involves an axial load applied to an adducted and often internally rotated arm. This force drives the humeral head superiorly, often with an anterior component. The humeral head is forced against the superior glenoid rim, tearing the superior capsule and ligaments, and often fracturing the superior glenoid. Concurrently, the humeral head can be driven into the coracoacromial arch, leading to fractures of the acromion, clavicle, or coracoid, or severe bruising/impaction. The disruption of the superior stabilizers (SGHL, CHL, superior labrum) and the rotator cuff facilitates the superior migration of the humeral head.
Clinical and Radiographic Evaluation
Clinical evaluation of superior glenohumeral dislocation requires a high index of suspicion. Patients typically present with significant pain and an inability to move the affected extremity. The classic physical examination findings include a foreshortened upper extremity held in a position of adduction, often with slight internal rotation. On palpation, the humeral head can often be felt in an abnormally high position, superior to the acromion, or prominent anterosuperiorly beneath the skin. Conversely, the glenoid fossa may feel empty.

A thorough neurovascular assessment is paramount given the high incidence of associated injuries. The integrity of the axillary nerve must be assessed by evaluating deltoid function (shoulder abduction) and sensation over the lateral deltoid patch. A complete neurological examination of the entire brachial plexus (musculocutaneous, median, ulnar, radial nerves) is essential, alongside palpation of peripheral pulses (radial, ulnar) and assessment of capillary refill to rule out vascular compromise.
Radiographic Evaluation:
A standard trauma series of the affected shoulder is mandatory and typically includes:
*
Anteroposterior (AP) view:
This view is often diagnostic, clearly demonstrating the humeral head superior to the acromion process. It also allows for initial assessment of associated fractures of the clavicle, acromion, and proximal humerus.
*
Scapular-Y view:
Useful for confirming the superior displacement relative to the glenoid and for identifying associated fractures of the glenoid or scapular body/spine.
*
Axillary view:
This projection is crucial for confirming the anterior or posterior component of the dislocation and for assessing the integrity of the glenoid rim and humeral head articular surface. However, it can be technically challenging or painful to obtain in this injury.
Radiographs must be meticulously scrutinized for associated fractures, which are almost universally present. These include glenoid rim fractures, humeral head impaction fractures (Hill-Sachs variant, reverse Hill-Sachs), greater and lesser tuberosity fractures, acromion fractures (especially the anterior or lateral acromion), clavicle fractures (particularly distal clavicle), and coracoid fractures.
Advanced Imaging:
*
Computed Tomography (CT) scan:
A CT scan is indispensable for preoperative planning. It provides a detailed assessment of complex fracture patterns, articular involvement, glenoid bone loss, and the precise position of the humeral head relative to the glenoid and surrounding bony structures. This information is critical for determining reducibility and planning fixation strategies. Three-dimensional (3D) reconstructions are particularly helpful for visualizing the extent of bony injury.
*
Magnetic Resonance Imaging (MRI):
While often not performed acutely due to the emergent nature of the injury, MRI can provide valuable information regarding soft tissue injuries, including rotator cuff tears, labral pathology, capsular avulsions, and potential brachial plexus involvement. It can be considered once bony stability is addressed or if neurological symptoms persist post-reduction.
Indications & Contraindications
Management of superior glenohumeral dislocation typically depends on the reducibility of the dislocation and the extent of associated injuries.
| Indications for Operative Management | Indications for Non-Operative Management |
|---|---|
| Irreducible closed dislocation (due to interposed soft tissue or bone) | Isolated superior dislocation without significant associated fractures |
| Significant associated fractures requiring fixation: | Successful closed reduction |
| - Displaced glenoid rim fractures (e.g., >2mm displacement, >25% glenoid) | Stable post-reduction with minimal associated injury |
| - Displaced humeral head fractures (e.g., greater tuberosity >5mm displacement) | Mild associated avulsion fractures (non-displaced, stable) |
| - Displaced acromial or clavicle fractures compromising the superior arch | Patient comorbidities precluding surgery (severe medical contraindications) |
| - Coracoid fractures impacting stability | |
| Neurovascular compromise requiring urgent exploration and repair | |
| Open dislocation | |
| Recurrent instability after initial closed reduction | |
| Interposed soft tissue (e.g., biceps tendon, rotator cuff) or bone block preventing reduction |
Contraindications:
Absolute contraindications to surgical intervention are rare and primarily relate to the patient's overall medical status and ability to tolerate anesthesia and surgery. Severe, uncorrectable coagulopathy or critical cardiopulmonary instability would generally contraindicate elective or semi-elective procedures. Relative contraindications may include active infection in the surgical field, severe osteopenia precluding stable fixation, or pre-existing neurological deficits that complicate assessment. The decision for operative versus non-operative management is always individualized, weighing the risks of surgery against the potential for poor functional outcomes without intervention.
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing outcomes in superior glenohumeral dislocations, given their complexity and high association with severe injuries.
Pre-operative Assessment:
1.
Comprehensive History and Physical:
Re-evaluate the mechanism of injury, prior shoulder history, and particularly focus on a detailed neurovascular examination, documenting all deficits.
2.
Advanced Imaging Review:
Thorough review of all radiographs, CT scans (with 3D reconstructions), and MRI (if obtained). Identify all associated fractures, their displacement, articular involvement, and assess for soft tissue blocks to reduction (e.g., entrapped biceps tendon, rotator cuff avulsions). Map out the fracture lines and plan potential fixation points.
3.
Surgical Team Communication:
Discuss the case with the anesthesiologist, detailing potential for significant blood loss, prolonged operative time, and the need for neuromonitoring if brachial plexus injury is suspected.
4.
Informed Consent:
Thoroughly counsel the patient regarding the nature of the injury, the complexity of the procedure, potential need for multiple fixation techniques, and significant risks including neurovascular injury (especially axillary nerve), infection, stiffness, recurrent instability, nonunion/malunion, post-traumatic arthritis, and the possibility of conversion to arthroplasty in the long term.
Patient Positioning:
The choice of patient positioning depends on the planned surgical approach and surgeon preference, aiming for optimal access and visualization of all anticipated pathology.
-
Beach Chair Position:
- Advantages: Provides excellent access to the anterior, superior, and often posterior aspects of the shoulder. Allows for easy conversion to an anterior or superior approach. Maintains physiological alignment for neurovascular assessment. Allows for a contralateral shoulder examination if needed.
- Disadvantages: Risk of cerebral hypoperfusion (though rare with careful monitoring), potential for cervical spine issues.
- Setup: Patient is semi-recumbent, typically at 45-70 degrees. Head supported in a headrest (e.g., 'Mayfield' or horseshoe). Ensure the head is stable and neutral to avoid brachial plexus stretch. The affected shoulder should be draped free to allow full range of motion. A small roll placed longitudinally along the medial border of the scapula can protract the scapula slightly, improving access.
-
Lateral Decubitus Position:
- Advantages: Useful if a posterior approach is anticipated or for gravity-assisted traction for reduction. Can be beneficial for visualizing specific aspects of the glenoid.
- Disadvantages: Limited access to some anterior structures, potential for brachial plexus traction injury with prolonged arm traction.
- Setup: Patient positioned on the unaffected side, secured with beanbag and straps. Axillary roll placed to protect the neurovascular bundle of the dependent arm. Affected arm suspended in traction for closed reduction attempts or free-draped for open approaches.
Anesthesia:
General anesthesia is typically preferred for open reduction given the complexity and potential for prolonged operative time. A regional interscalene block can be used pre-operatively for excellent post-operative pain control, but its use during surgery should be carefully considered if intraoperative neurological monitoring is planned.
Preparation:
* Pre-operative antibiotics (e.g., Cefazolin) administered within 60 minutes of incision.
* Thorough sterile preparation and draping of the shoulder and arm, allowing for manipulation of the extremity throughout the surgical field. A sterile impervious stockinette is often applied to the extremity.
* Confirm availability of a wide array of orthopedic implants for fracture fixation (plates, screws, sutures, anchors) and necessary instruments (bone hooks, osteotomes, Hohmann retractors, specialized reduction clamps).
Detailed Surgical Approach / Technique
Surgical intervention for superior glenohumeral dislocation is typically necessitated by irreducibility or significant associated fractures. The primary goals are anatomical reduction of the humeral head, stable fixation of all associated fractures, and restoration of glenohumeral and superior arch stability.
Initial Closed Reduction Attempt:
Even if an open reduction is anticipated, a gentle attempt at closed reduction under general anesthesia is often performed. This involves longitudinal traction on the adducted arm, with counter-traction applied to the axilla. Gentle manipulation, including slight abduction, adduction, and rotation, may be employed. If successful, post-reduction radiographs confirm reduction, and stability is assessed clinically. If reduction is achieved, a period of sling immobilization is followed by a structured rehabilitation protocol. However, persistent irreducible dislocation or significant bony blocks often mandate open intervention.
Open Reduction - General Principles:
Failure of closed reduction is commonly due to interposed soft tissues (e.g., rotator cuff, biceps tendon, capsule) or bony fragments (e.g., glenoid rim, humeral head fragment). The surgical approach is tailored to the specific pathology identified on pre-operative imaging.
1. Approach Selection:
*
Deltopectoral Approach:
This is the most versatile and commonly utilized approach for superior glenohumeral dislocations, especially when anterior or superior glenoid pathology, humeral head fractures, or associated clavicle/coracoid fractures are present. It provides excellent access to the entire anterior aspect of the joint, the axillary neurovascular bundle, and the proximal humerus.
*
Extension to Anterosuperior/Deltoid-Splitting:
This can be achieved by extending the incision superiorly along the anterior border of the deltoid, allowing access to the acromion, AC joint, and the superior rotator cuff. Care must be taken to avoid violating the axillary nerve, which runs approximately 5-7 cm distal to the acromial edge.
*
Anterosuperior (Sabre-Cut) Approach:
Can be used if primary pathology involves the acromion or AC joint, or for direct visualization of the superior glenoid and rotator cuff.
*
Posterior Approach:
Rarely indicated for primary superior dislocations unless there is significant posterior glenoid fracture or associated posterior instability.
2. Detailed Surgical Technique (Example: Extended Deltopectoral Approach for Irreducible Dislocation with Superior Arch Fractures):
- Incision: A curvilinear incision is made from the superior aspect of the coracoid process, extending distally along the deltopectoral groove for approximately 8-12 cm, then curving laterally along the anterior border of the deltoid, potentially extending over the acromion if AC joint or acromial fixation is needed.
- Superficial Dissection: The subcutaneous tissue and platysma (if present) are divided. Identify the cephalic vein running in the deltopectoral groove. It is typically retracted medially with the pectoralis major.
- Internervous Plane: The deltopectoral interval is identified between the deltoid muscle (innervated by the axillary nerve) laterally and the pectoralis major muscle (innervated by the medial and lateral pectoral nerves) medially. Develop this plane.
-
Deep Dissection:
- Conjoint Tendon: The conjoint tendon (short head of biceps and coracobrachialis) is identified and retracted medially. If increased exposure is needed, the conjoint tendon origin can be osteotomized from the coracoid and reattached later.
- Subscapularis: The subscapularis muscle and its tendon are identified. In superior dislocations, the subscapularis may be torn or stretched. The anterior capsule and subscapularis tendon are carefully divided (e.g., a lesser tuberosity osteotomy or a split through the tendon, medial to its insertion to preserve the medial capsule for repair).
- Axillary Nerve Identification: Prophylactic identification of the axillary nerve is paramount. It typically runs approximately 5-7 cm distal to the acromion, exiting the quadrangular space posteriorly. In superior dislocations, the nerve may be displaced or entrapped, requiring careful palpation and visualization.
-
Joint Exposure and Reduction:
- Debridement: Remove any hematoma, loose osteochondral fragments, or incarcerated soft tissue (e.g., biceps tendon).
- Visualization: Assess the glenoid fossa, humeral head, and surrounding capsule. Identify any structures blocking reduction. The humeral head will typically be superior and possibly anterior to the glenoid.
- Reduction Maneuver: Using bone hooks, strong periosteal elevators, or specialized reduction clamps, direct reduction can be performed. Gentle traction is applied to the arm, and the humeral head is maneuvered inferiorly and then onto the glenoid. This often requires carefully prying the humeral head past the superior glenoid rim or any fractured fragments. Ensure the long head of biceps tendon is reduced into its groove if it was displaced.
-
Fixation of Associated Fractures:
- Glenoid Fractures: Small, non-displaced fractures may be left. Displaced intra-articular fractures (e.g., Bankart lesions, superior glenoid rim fractures) require anatomical reduction and fixation with cannulated screws or suture anchors.
- Humeral Head/Tuberosity Fractures: Anatomical reduction and internal fixation with sutures (for non-displaced tuberosity fractures), screws, or small plates.
-
Acromial/Clavicle/Coracoid Fractures:
These need stable fixation to restore the superior arch.
- Acromion Fractures: Plates and screws (e.g., reconstruction plates, L-plates) are commonly used.
- Distal Clavicle Fractures: Plates and screws (e.g., pre-contoured distal clavicle plates) or tension band wiring for specific patterns.
- Coracoid Fractures: Small fragment screws, often requiring extension of the approach superiorly or careful medial retraction.
-
Capsular and Rotator Cuff Repair:
- Capsular Repair: After reduction and fracture fixation, the anterior capsule and subscapularis (if divided) are meticulously repaired. Repair of the superior capsule and any avulsed superior labrum/biceps anchor (SLAP repair) is crucial for preventing recurrent superior instability. Suture anchors can be used for labral and capsular repair.
- Rotator Cuff Repair: Any identified rotator cuff tears (especially supraspinatus) are repaired using transosseous sutures or suture anchors, depending on the tear pattern and tissue quality.
-
Wound Closure:
- Copious irrigation.
- Check range of motion and stability.
- Close the deltopectoral interval.
- Repair the deltoid if any portion was detached or split.
- Subcutaneous tissue and skin closure in layers. Drain placement is optional.
Complications & Management
Superior glenohumeral dislocations are associated with a high rate of significant complications due to the high-energy mechanism and inherent complexity of the injury. Early recognition and appropriate management are crucial for mitigating long-term sequelae.
| Complication | Incidence | Salvage Strategy |
|---|---|---|
| Neurovascular Injury | ||
| - Axillary Nerve Neuropraxia/Injury | 30-50% (variable) | Observation (up to 6 months), serial EMG/NCS. If no recovery, nerve exploration & repair/grafting. |
| - Brachial Plexus Injury | Rare (1-5%) | Observation, serial EMG/NCS. If persistent deficit, early referral to brachial plexus specialist for exploration/reconstruction. |
| - Axillary Artery/Vein Injury | Very rare (<1%) | Immediate vascular surgical consultation, emergent exploration, repair (primary or graft) or ligation (venous). |
| Fracture-Related Complications | ||
| - Nonunion of associated fracture | Variable (e.g., acromion 10-20%) | Revision ORIF with bone grafting (autograft/allograft), plate exchange. |
| - Malunion of associated fracture | Variable | Corrective osteotomy (if symptomatic and functional deficit), hardware removal. |
| - Post-traumatic Arthritis | Up to 20-30% long-term | Conservative management (NSAIDs, PT, injections). Arthroscopic debridement. Hemiarthroplasty or total shoulder arthroplasty. |
| Instability & Stiffness | ||
| - Recurrent Instability | 5-10% post-op | Revision stabilization (arthroscopic or open), bone block procedures for glenoid bone loss. |
| - Stiffness/Adhesive Capsulitis | 10-20% | Aggressive physical therapy, pain management. Manipulation Under Anesthesia (MUA). Arthroscopic capsular release. |
| Infection | ||
| - Surgical Site Infection (SSI) | 1-5% | Superficial: oral antibiotics, local wound care. Deep: surgical debridement, IV antibiotics, possibly implant removal. |
| Other Complications | ||
| - Heterotopic Ossification (HO) | Variable (up to 20%) | Prophylaxis with NSAIDs or radiation post-op (for high-risk cases). Excision of mature HO if symptomatic and function-limiting. |
| - Hardware Irritation/Failure | Common | Hardware removal after fracture union (if symptomatic), revision of failed hardware. |
| - Rotator Cuff Re-tear | 10-25% | Revision rotator cuff repair, possibly with augmentation (e.g., superior capsular reconstruction, patch graft). |
Specific Management Considerations:
- Neurovascular Injury: Pre-operative and post-operative neurological status must be thoroughly documented. Axillary nerve neuropraxia is common and often recovers spontaneously within 3-6 months. Persistent deficits warrant EMG/NCS studies and potential nerve exploration. Vascular injuries are limb-threatening emergencies requiring immediate consultation with a vascular surgeon.
- Post-traumatic Arthritis: Due to articular cartilage damage from the initial trauma or subsequent instability/malunion, post-traumatic arthritis is a significant long-term concern. Patients should be counseled on this risk. Management ranges from conservative measures to eventual arthroplasty (hemiarthroplasty or total shoulder arthroplasty), depending on the patient's age, activity level, and extent of arthrosis.
- Stiffness: A common complication after complex shoulder trauma and surgery. Early, controlled rehabilitation with emphasis on pain control and PROM is vital. If severe stiffness persists despite adequate therapy, manipulation under anesthesia and/or arthroscopic capsular release may be necessary.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a cornerstone of recovery after superior glenohumeral dislocation repair and must be highly individualized based on the stability of fracture fixation, quality of soft tissue repairs (capsule, labrum, rotator cuff), and patient-specific factors. The protocol typically follows a phased approach, balancing protection of healing tissues with progressive restoration of motion and strength.
General Principles:
*
Pain Management:
Aggressive pain control is essential to allow for early, protected motion.
*
Protection:
The operated extremity is protected in a sling or shoulder immobilizer for an initial period.
*
Early Motion:
Controlled, passive, and later active-assisted range of motion is introduced early to prevent stiffness.
*
Gradual Strengthening:
Progressive strengthening exercises are initiated once adequate healing and stability are achieved.
*
Proprioception and Neuromuscular Control:
Emphasized throughout the later phases to restore normal shoulder function.
Phase I: Protection and Early Controlled Motion (Weeks 0-6)
*
Goals:
Protect surgical repairs, minimize pain and swelling, initiate passive range of motion (PROM) within protected arcs, prevent stiffness.
*
Immobilization:
Sling or shoulder immobilizer worn continuously, removed only for exercises and hygiene. Duration depends on the stability of repairs (e.g., 4-6 weeks for rotator cuff/labral repair, shorter for stable bony fixation only).
*
Exercises (Daily):
*
Pendulum Exercises:
Gentle, gravity-assisted swings of the arm.
*
Passive Range of Motion (PROM):
Performed by a therapist or with the unaffected arm.
*
Forward Flexion:
To 90-120 degrees (avoiding active deltoid contraction).
*
External Rotation:
To 0-30 degrees (depending on capsular/labral repair integrity).
*
Internal Rotation:
Hand-to-sacrum/buttock.
*
Abduction:
Limited to 60-90 degrees.
*
Scapular Stabilization Exercises:
Gentle scapular squeezes without shoulder motion.
*
Elbow, Wrist, Hand ROM:
Maintained to prevent stiffness.
*
Precautions:
Avoid active shoulder elevation, external rotation past neutral, or reaching behind the back. No lifting, pushing, or pulling.
Phase II: Progressive Motion and Gentle Strengthening (Weeks 6-12)
*
Goals:
Restore full, pain-free active range of motion (AROM), begin light isometric strengthening.
*
Immobilization:
Gradually wean from sling as comfort and stability allow, typically around 6-8 weeks.
*
Exercises:
*
Active-Assisted Range of Motion (AAROM):
Progress from PROM to AAROM using pulleys, sticks, or the unaffected arm.
*
Active Range of Motion (AROM):
Gradually work towards full AROM in all planes.
*
Isometric Strengthening:
Begin gentle isometric exercises for rotator cuff (internal/external rotation) and deltoid, performed in neutral positions.
*
Scapular Stabilization:
Progress to more active scapular stabilization exercises.
*
Light Resistance Training:
Very light resistance bands can be introduced for rotator cuff and periscapular muscles as tolerated.
*
Precautions:
Continue to avoid heavy lifting or sudden, forceful movements. Avoid positions of apprehension.
Phase III: Strength and Endurance (Weeks 12-24)
*
Goals:
Develop functional strength, endurance, and proprioception.
*
Exercises:
*
Progressive Resistive Exercises (PREs):
Increase intensity and resistance for rotator cuff, deltoid, and periscapular muscles using weights, resistance bands, and machines.
*
Proprioceptive and Neuromuscular Control:
Begin exercises like rhythmic stabilization, perturbations, and unstable surface activities.
*
Core Strengthening:
Integrate core strength into shoulder rehabilitation.
*
Functional Activities:
Gradually introduce activities mimicking daily living.
*
Precautions:
Continue to monitor for pain or instability. Avoid ballistic movements until significant strength is regained.
Phase IV: Return to Activity (Weeks 24+ and beyond)
*
Goals:
Maximize strength, power, and endurance for specific work or sports activities. Gradual return to full function.
*
Exercises:
*
Sport-Specific or Work-Specific Training:
Incorporate activities that mimic the demands of the patient's desired activities.
*
Plyometrics and Power Training:
For overhead athletes or demanding occupations.
*
Maintenance Program:
Long-term exercise program to maintain strength and flexibility.
*
Return to Play/Work Criteria:
* Full, pain-free range of motion.
* Strength symmetrical to the contralateral side (or >90%).
* Excellent dynamic stability and neuromuscular control.
* Absence of apprehension or instability.
* Requires a minimum of 6-12 months for full recovery, potentially longer for high-demand individuals.
Summary of Key Literature / Guidelines
Superior glenohumeral dislocation remains a challenging and relatively under-reported injury in the orthopedic literature due to its rarity. Much of the available evidence consists of case reports, small case series, and expert opinion, making the establishment of high-level evidence-based guidelines difficult.
Key Themes from the Literature:
- High-Energy Trauma: The literature consistently highlights the high-energy nature of the mechanism of injury, often involving axial loading onto an adducted arm. This distinguishes it from other shoulder dislocations.
- Associated Injuries: The high prevalence of associated fractures (acromion, clavicle, coracoid, glenoid, humeral tuberosities) and soft tissue damage (rotator cuff, labrum, neurovascular structures) is a recurring theme. Studies emphasize the need for thorough pre-operative imaging (CT scans are crucial) to identify these concomitant injuries, as they dictate the surgical strategy and influence prognosis.
- Irreducibility: A significant proportion of superior glenohumeral dislocations are irreducible by closed means due to interposed soft tissues (e.g., long head of biceps, rotator cuff, capsule) or bony fragments. This often necessitates open reduction.
- Surgical Challenges: Open reduction and internal fixation (ORIF) are frequently required. The choice of surgical approach depends on the primary pathology. Meticulous attention to anatomical reduction of the humeral head, stable fixation of associated fractures, and comprehensive repair of the superior capsulolabral complex and rotator cuff are paramount for restoring stability and preventing recurrent instability or stiffness.
- Complications: High rates of complications are reported, particularly neurovascular injuries (axillary nerve neuropraxia being most common), post-traumatic arthritis, and stiffness. Long-term functional outcomes can be variable, often dependent on the severity of initial trauma and efficacy of surgical reconstruction.
- Rehabilitation: A structured, phased rehabilitation program, individualized to the extent of injury and repair, is crucial for optimizing functional recovery and minimizing stiffness. Protection of repairs in early phases, followed by progressive motion and strengthening, is consistently advocated.
Current Perspectives:
While no universally accepted randomized controlled trials or comprehensive societal guidelines exist specifically for superior glenohumeral dislocations, the consensus among academic orthopedic surgeons emphasizes:
1.
High Index of Suspicion:
For unusual shoulder presentations after high-energy trauma.
2.
Comprehensive Diagnostic Workup:
Including advanced imaging (CT scan) to fully delineate all injuries.
3.
Aggressive Management of Associated Injuries:
Recognition that the associated fractures and soft tissue tears are often as critical as the dislocation itself.
4.
Open Reduction and Internal Fixation:
Often required due to irreducibility or significant associated fracture displacement.
5.
Focus on Superior Stability:
Emphasizing repair of the superior capsulolabral complex and any rotator cuff tears to prevent superior migration and recurrent instability.
6.
Realistic Patient Counseling:
Regarding the complex nature of the injury, potential for complications, and often prolonged recovery period.
Further multicenter studies, though challenging due to rarity, are needed to establish higher-level evidence for optimal surgical techniques and long-term outcomes in this challenging injury pattern.
