Comprehensive Guide to Subtrochanteric Femoral Fractures: Epidemiology, Anatomy, & Management
Key Takeaway
Subtrochanteric femoral fractures are challenging hip injuries at the metaphyseal-diaphyseal junction. They exhibit unique biomechanical stresses and powerful muscle forces causing characteristic displacement. The thick cortical bone and reduced vascularity complicate fixation, demanding precise surgical planning. This careful approach is crucial for optimal healing outcomes and to mitigate higher rates of nonunion.
Introduction and Epidemiology
Subtrochanteric femoral fractures represent a distinct and challenging subset of hip fractures, characterized by their anatomical location, unique biomechanical environment, and propensity for complications. These fractures occur in the metaphyseal-diaphyseal junction of the femur, an area subjected to immense physiological loads and surrounded by powerful muscle groups. Accurate diagnosis, meticulous surgical planning, and precise execution are paramount for achieving optimal outcomes.
Subtrochanteric fractures account for approximately 10% to 30% of all hip fractures. While commonly associated with high-energy trauma in younger individuals and falls in the elderly, their incidence exhibits a bimodal distribution. A greater incidence is observed in individuals 20 to 40 years of age, typically resulting from high-velocity trauma such as motor vehicle collisions or falls from height. A second, larger peak occurs in persons older than 60 years of age, often associated with lower-energy mechanisms in osteoporotic bone.
The increasing prevalence of atypical femoral fractures (AFFs) associated with long-term bisphosphonate use has also contributed to the rising incidence, particularly in the elderly population. These iatrogenic fractures often present with prodromal thigh pain and specific radiographic features, including cortical thickening, a transverse fracture line originating at the lateral cortex, and medial spiking. The American Society for Bone and Mineral Research (ASBMR) criteria strictly define these fractures, emphasizing the suppression of targeted bone remodeling and the subsequent accumulation of microdamage that leads to catastrophic failure under normal physiological loads.
Surgical Anatomy and Biomechanics
A subtrochanteric femur fracture is precisely defined as a fracture occurring between the lesser trochanter and a point 5 cm distal to the lesser trochanter. This region is a critical transition zone between the cancellous bone of the proximal metaphysis and the thick cortical bone of the diaphysis.
Bony Architecture and Stress Distribution
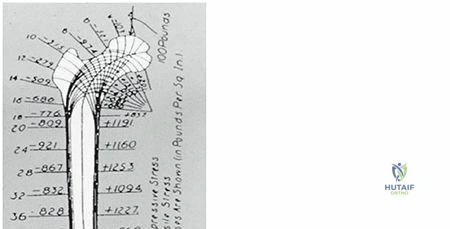
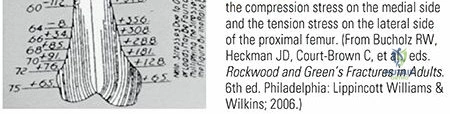
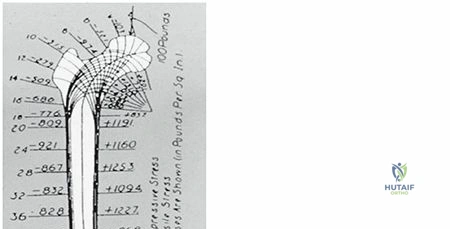
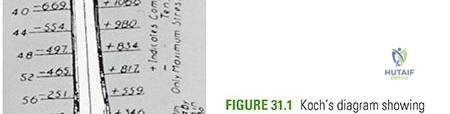
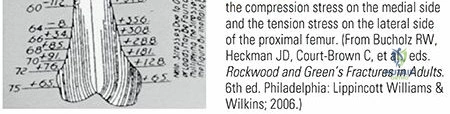
The subtrochanteric segment of the femur is subject to high biomechanical stresses. During ambulation and weight-bearing, the femur acts as a long lever arm, transmitting forces from the pelvis to the tibia. The medial and posteromedial cortices are the sites of high compressive forces, whereas the lateral cortex experiences high tensile forces. The anterolateral cortex is also a zone of significant tensile stress. The interplay of these forces, exacerbated by muscle pull, contributes to the instability and characteristic displacement patterns observed in subtrochanteric fractures. The strong cortical bone in this region makes fixation challenging, as implants must withstand significant cyclic loading.
The subtrochanteric area of the femur is composed mainly of thick cortical bone, in contrast to the more trabecular nature of the intertrochanteric region. This cortical dominance has significant implications for both vascularity and healing potential. Cortical bone, while strong, possesses comparatively less intrinsic vascularity than cancellous bone, relying heavily on periosteal and endosteal blood supplies. The potential for healing is therefore compromised, contributing to higher rates of delayed union and nonunion if surgical principles are not meticulously adhered to.
Muscle Attachments and Deforming Forces
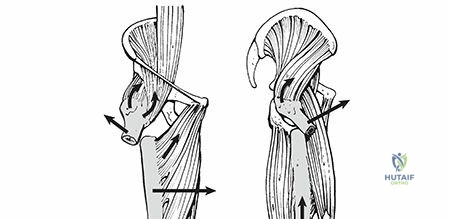
The powerful musculature surrounding the proximal femur exerts considerable deforming forces on fracture fragments, often leading to characteristic displacement patterns that complicate reduction.
- Proximal Fragment:
- Abduction: Gluteus medius and minimus, inserting on the greater trochanter, abduct the proximal fragment.
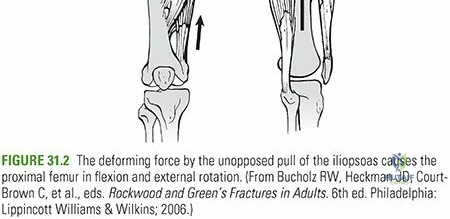
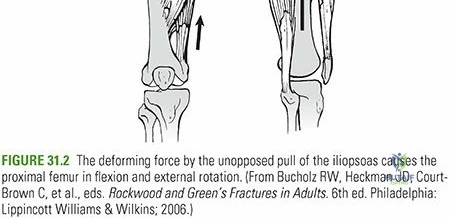
- Flexion: The iliopsoas muscle, inserting on the lesser trochanter, powerfully flexes the proximal fragment.
- External Rotation: The short external rotators (piriformis, obturator internus, superior and inferior gemelli, quadratus femoris) insert on or near the greater trochanter, externally rotating the proximal fragment.
The combined effect of these muscles results in an abducted, flexed, and externally rotated proximal fragment.
- Distal Fragment:
- Adduction: The adductor longus, brevis, and magnus pull the distal fragment medially.
- Shortening: The quadriceps and hamstring muscle groups cross both the hip and knee joints, exerting a massive longitudinal pull that results in significant limb shortening and overriding of the fracture fragments.
Understanding these vectors is the cornerstone of successful closed or limited open reduction. Overcoming the flexion and abduction of the proximal fragment often requires manipulating the distal fragment to match the proximal fragment's spatial orientation, rather than attempting to force the short, powerful proximal fragment back into anatomical alignment.
Indications and Contraindications
Operative stabilization is the absolute gold standard for subtrochanteric femur fractures. Non-operative management is plagued by unacceptable rates of nonunion, malunion, profound shortening, deep vein thrombosis, decubitus ulcers, and pulmonary complications secondary to prolonged bed rest and skeletal traction.
Non-operative management is reserved strictly for patients who are medically unfit for anesthesia or those who are non-ambulatory with minimal pain, where surgical intervention would not alter their functional baseline but would introduce significant perioperative risk.
| Management Strategy | Indications | Contraindications |
|---|---|---|
| Intramedullary Nailing | Gold standard for most subtrochanteric fractures; Atypical Femoral Fractures (AFFs); Pathologic fractures; Polytrauma patients. | Active medullary infection; Obliterated medullary canal (severe deformity/prior hardware); Pediatric patients with open physes. |
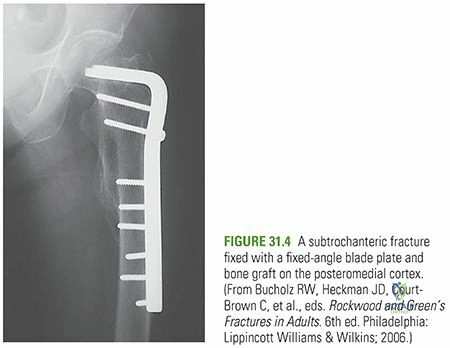
| Open Reduction Internal Fixation | Fractures extending into the piriformis fossa or greater trochanter preventing IMN starting point; Narrow intramedullary canal; Periprosthetic fractures. | Severe osteopenia compromising screw purchase; Severe soft tissue compromise over the lateral thigh. |
| Non-Operative Management | Bedbound, non-ambulatory patients with minimal pain; Patients with unacceptable anesthetic risk (ASA IV/V); Palliative care scenarios. | Ambulatory patients; Polytrauma; Open fractures; Progressive neurological deficit. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is critical to anticipate reduction difficulties, select the appropriate implant, and minimize intraoperative complications.
Radiographic Evaluation and Templating
Standard imaging includes full-length orthogonal views of the affected femur, an anteroposterior pelvis radiograph, and orthogonal views of the ipsilateral hip and knee. Contralateral full-length femur radiographs are highly recommended for templating, particularly to assess the native femoral bow (radius of curvature) and canal diameter, which are crucial for intramedullary nail selection.
For high-energy trauma or complex fracture patterns extending into the intertrochanteric region or femoral neck, a computed tomography (CT) scan is mandatory. CT imaging rules out occult femoral neck fractures, which occur in up to 10% of high-energy femoral shaft and subtrochanteric fractures, and drastically alters the surgical plan.
Patient Positioning and Setup
Surgeons generally choose between two positioning modalities based on institutional resources, assistant availability, and personal preference.
- Fracture Table (Supine or Lateral): Allows for sustained skeletal traction, facilitating length restoration and continuous fluoroscopic imaging without interference. However, the fracture table locks the patient in a static position, making dynamic reduction maneuvers (like flexing the hip to relax the iliopsoas) difficult. It also increases the risk of pudendal nerve palsy and perineal sloughing if traction is prolonged.
- Flat Radiolucent Table (Supine): Often preferred for subtrochanteric fractures because it allows the surgeon to freely manipulate the leg. The hip can be flexed and abducted to match the proximal fragment. A bump is typically placed under the ipsilateral hemipelvis. Manual traction or a femoral distractor is utilized for length. This setup is highly advantageous when limited open reduction techniques or percutaneous clamping are anticipated.
Implant Selection Principles
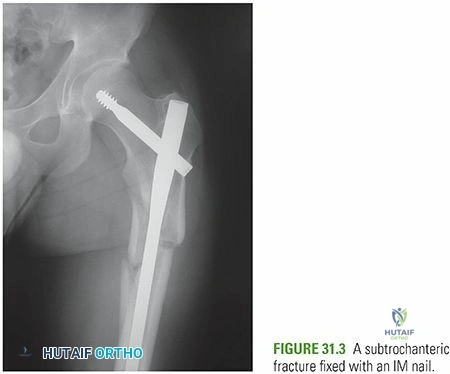
Cephalomedullary nails are the implant of choice due to their load-sharing biomechanics. By placing the implant centrally within the medullary canal, the bending moment is significantly reduced compared to lateral plate constructs.
- Standard vs Long Nails: Long nails spanning the entire femur are generally preferred to protect the entire diaphysis, particularly in osteoporotic bone or in the setting of AFFs, to prevent stress risers at the tip of a short nail.
- Starting Point: Trochanteric entry nails are currently favored over piriformis entry nails due to a lower risk of iatrogenic vascular injury to the femoral head blood supply and easier trajectory in obese patients. However, the exact starting point must be meticulously respected to avoid varus malalignment.
Detailed Surgical Approach and Technique
The overarching principle of subtrochanteric fracture surgery is achieving anatomical or near-anatomical reduction prior to reaming and implant insertion. Never ream an unreduced subtrochanteric fracture. Eccentric reaming will dictate the trajectory of the nail, permanently locking the fracture into a malreduced position (typically varus and procurvatum).
Closed Reduction Strategies
Upon positioning and sterile draping, longitudinal traction is applied to restore length. Due to the deforming forces, traction alone is rarely sufficient. The distal fragment must be manipulated to match the proximal fragment.
- Correcting Sagittal Deformity (Procurvatum): The proximal fragment is flexed by the iliopsoas. To align the distal fragment, the hip can be flexed, or a crutch/bump can be placed posterior to the distal fragment to elevate it. Alternatively, a percutaneous Schanz pin can be placed into the proximal fragment to act as a joystick, manually extending it to match the distal shaft.
- Correcting Coronal Deformity (Varus): The proximal fragment is abducted. The distal limb must be adducted, or percutaneous tools (like a ball spike pusher) can be introduced laterally to push the proximal fragment into adduction.
Adjunctive Reduction Techniques
When closed maneuvers fail, surgeons must swiftly transition to adjunctive techniques to avoid prolonged surgical time and excessive radiation exposure.
- Poller (Blocking) Screws: Placed strategically to narrow the medullary canal and direct the guidewire and subsequent nail. To correct a varus deformity, a blocking screw is placed in the lateral aspect of the proximal fragment or the medial aspect of the distal fragment.
- Percutaneous Clamping: A small lateral incision is made, and a collinear reduction clamp or pointed reduction forceps is applied across the fracture site. This is highly effective for long oblique or spiral fracture patterns.
- Cerclage Wiring: For spiral fractures with a large butterfly fragment, minimally invasive cerclage wiring can anatomically reconstruct the tubular structure of the diaphysis, converting a complex fracture into a simple one prior to nailing. Modern percutaneous passers minimize periosteal stripping.
- Limited Open Reduction: If all else fails, a formal lateral approach is utilized to directly visualize and reduce the fracture. While this violates the fracture hematoma, an anatomical reduction with an open technique is biomechanically superior to a malreduced closed technique.
Intramedullary Nailing Technique
- Entry Point: A longitudinal incision is made proximal to the greater trochanter. A guide pin is advanced into the tip of the greater trochanter (or slightly medial to the tip, depending on the specific implant design) on the AP view, and centered in the proximal femur on the lateral view.
- Opening the Canal: An opening reamer is passed over the guide pin.
- Passing the Fracture: A ball-tipped guidewire is passed down the canal. It is imperative that the fracture is perfectly reduced as the wire crosses the fracture site. The wire is advanced to the level of the physeal scar in the distal femur.
- Reaming: Sequential reaming is performed, typically 1.0 to 1.5 mm larger than the selected nail diameter. During reaming, the reduction must be maintained to prevent eccentric cortical chatter.
- Nail Insertion: The selected cephalomedullary nail is inserted. Excessive force should not be used; if the nail does not advance, the reduction or canal diameter must be reassessed.
- Proximal Locking: Depending on the fracture pattern and implant, a single large helical blade or recon-style screws are placed into the femoral head. The trajectory must be central-central or inferior-central in the femoral head to maximize purchase and prevent cut-out.
- Distal Locking: Distal interlocking screws are placed via a freehand fluoroscopic technique.
Complications and Management
Subtrochanteric fractures possess one of the highest complication rates among long bone fractures due to the immense mechanical stresses and precarious vascularity of the region.
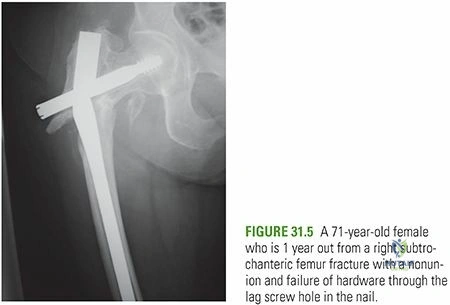
The most devastating mechanical complication is varus malreduction. Even a few degrees of varus significantly increases the bending moment on the intramedullary nail. Because the medial cortex is under compressive load, a varus gap prevents cortical load-sharing. The implant is forced to absorb the entirety of the cyclical loading during ambulation, inevitably leading to fatigue failure of the nail or the locking screws before biological union can occur.
| Complication | Estimated Incidence | Etiology and Risk Factors | Salvage and Management Strategy |
|---|---|---|---|
| Varus Malreduction | 10% - 20% | Failure to counteract abductors; Lateral starting point; Eccentric reaming. | Early recognition; Revision surgery with corrective osteotomy, exchange nailing, or supplementary plating if symptomatic or at high risk of failure. |
| Nonunion | 5% - 10% | Poor biological environment; Varus malreduction leading to instability; Atypical fracture biology (bisphosphonates). | Rule out infection. Exchange nailing (reaming to a larger diameter to stimulate biology and increase stability); Bone grafting; Augmentation with a lateral locking plate. |
| Implant Failure | 2% - 5% | Unrecognized nonunion; Persistent varus deformity; Undersized intramedullary nail. | Hardware removal, debridement of fibrous nonunion, revision fixation (often combined IMN and plate construct), and autologous bone grafting. |
| Iatrogenic Fracture | 1% - 3% | Forcible nail insertion; Mismatched radius of curvature (anterior cortical breach). | If recognized intraoperatively: bypass with a longer nail, supplementary cerclage wiring, or plate fixation. |
| Infection | 1% - 2% | Open fractures; Prolonged surgical time; Extensive open reduction. | Irrigation and debridement; Suppressive antibiotics; Hardware retention if stable and healing, or exchange to antibiotic-coated nail/spacer if unstable. |
Post Operative Rehabilitation Protocols
Successful management of subtrochanteric fractures extends beyond the operating room. A structured, phased rehabilitation protocol is essential for restoring functional mobility and preventing systemic complications.
Immediate Postoperative Phase (Weeks 0-2)
The primary goals in the immediate postoperative period are pain control, medical optimization, prevention of deep vein thrombosis (DVT), and early mobilization.
* Weight-Bearing Status: Historically, subtrochanteric fractures were kept strictly non-weight-bearing. However, modern cephalomedullary nails allow for early load-sharing. For stable fracture patterns with anatomical reduction and good bone quality, weight-bearing as tolerated (WBAT) is generally encouraged. For highly comminuted fractures, poor bone stock, or tenuous fixations, touch-down weight-bearing (TDWB) may be instituted for the first 6 weeks.
* Physical Therapy: Bed-to-chair transfers and ambulation with an assistive device (walker or crutches) begin on postoperative day one. Range of motion exercises for the hip, knee, and ankle are initiated to prevent arthrofibrosis.
* Pharmacotherapy: Chemical DVT prophylaxis (e.g., Low Molecular Weight Heparin or Direct Oral Anticoagulants) is mandatory for a minimum of 35 days, barring contraindications. Routine osteoporosis evaluation and management should be initiated, particularly in elderly patients or those with suspected AFFs.
Intermediate Rehabilitation (Weeks 2-12)
During this phase, the focus shifts to restoring muscle strength, improving gait mechanics, and weaning off assistive devices.
* Clinical Follow-up: Radiographs are typically obtained at 2, 6, and 12 weeks to assess for callus formation, maintenance of reduction, and hardware integrity.
* Physical Therapy: Progression of weight-bearing status if previously restricted. Strengthening emphasizes the hip abductors (gluteus medius), quadriceps, and core musculature. Aquatic therapy can be highly beneficial during this phase to reduce joint loading while providing global resistance.
Long Term Follow Up (Months 3-12)
Return to baseline function can take up to a year. Patients are monitored for signs of delayed union or hardware irritation. In patients with atypical femoral fractures, the contralateral femur must be continuously monitored, as bilateral involvement is seen in up to 30% of cases. Prophylactic nailing of the contralateral femur may be indicated if there is cortical thickening and prodromal pain.
Summary of Key Literature and Guidelines
The surgical management of subtrochanteric fractures is guided by a robust body of orthopedic literature. Understanding these foundational studies and guidelines is critical for evidence-based practice.
- Biomechanics of Fixation: Studies by Koval et al. and Bong et al. have definitively demonstrated the biomechanical superiority of intramedullary nailing over extramedullary plating in the subtrochanteric region. The shorter lever arm of an intramedullary device significantly reduces bending stresses, lowering the rate of implant failure.
- Reduction Techniques: Kuzyk et al. provided a landmark review on the techniques for obtaining and maintaining reduction in subtrochanteric fractures. They emphasized that the biological cost of a limited open reduction is far outweighed by the mechanical catastrophe of a malreduced closed nailing. Their work popularized the systematic use of blocking screws and percutaneous clamps.
- Atypical Femoral Fractures (AFFs): The American Society for Bone and Mineral Research (ASBMR) task force reports (2010, updated 2014) are the definitive guidelines for diagnosing and managing AFFs. Key takeaways include the necessity of full-length femur radiographs in patients on long-term bisphosphonates presenting with thigh pain, the recommendation for intramedullary nailing over plating, and the critical need to cease antiresorptive therapy and consider anabolic agents (e.g., Teriparatide) postoperatively to enhance fracture healing.
- Starting Point Trajectory: Literature comparing piriformis versus trochanteric entry points (e.g., Starr et al.) indicates that while trochanteric entry is technically easier and less morbid to the abductor mechanism, an excessively lateral starting point on the greater trochanter inevitably drives the proximal fragment into varus. Strict adherence to the specific implant's designated entry trajectory is mandatory.
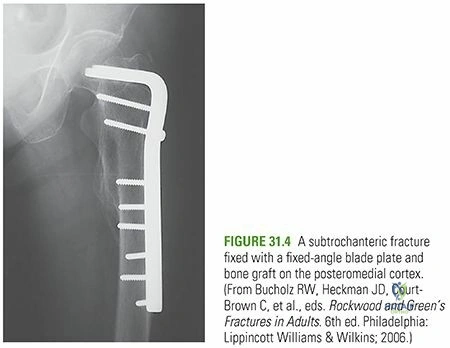
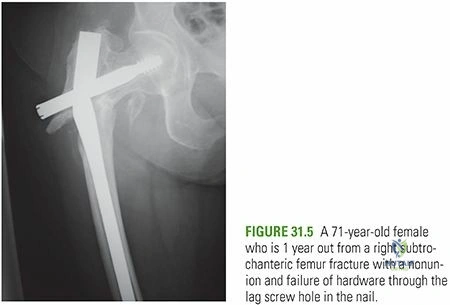
Clinical & Radiographic Imaging