Subtrochanteric Femoral Fractures: Comprehensive Surgical Management

Key Takeaway
Subtrochanteric femoral fractures occur between the lesser trochanter and the femoral isthmus. Due to intense deforming muscle forces—specifically the iliopsoas, abductors, and adductors—these fractures present significant alignment challenges. Intramedullary nailing remains the gold standard of treatment. Mastery of trajectory control, precise entry portal preparation, and appropriate cephalomedullary locking configurations are critical to preventing malunion and ensuring optimal biomechanical stability during postoperative rehabilitation.
Comprehensive Introduction and Patho-Epidemiology
Subtrochanteric femoral fractures represent one of the most mechanically demanding and biologically challenging subsets of proximal femur fractures encountered by the orthopedic surgeon. Anatomically defined as fractures occurring in the region extending from the inferior border of the lesser trochanter to the isthmus of the femoral diaphysis, this zone is frequently operationalized in the literature as the proximal 5 centimeters of the femoral shaft. Initially characterized by Boyd and Griffin as a highly unstable variant of peritrochanteric fractures, the management of these injuries has evolved significantly, yet they continue to demand meticulous surgical planning, profound anatomical knowledge, and flawless intraoperative execution to avert catastrophic complications.
The patho-epidemiology of subtrochanteric fractures demonstrates a distinct bimodal distribution. In the younger demographic, these injuries are predominantly the sequelae of high-energy trauma, such as motor vehicle collisions or falls from significant heights. These high-energy mechanisms typically result in highly comminuted fracture patterns, significant soft tissue stripping, and concomitant multi-system injuries. The profound dissipation of kinetic energy through the thick cortical bone of the subtrochanteric region often leads to complex, multi-fragmentary wedge or segmental fractures that severely compromise the inherent stability of the medial cortical buttress. Consequently, the biologic envelope is often impaired, increasing the risk of delayed union or nonunion.
Conversely, in the elderly population, subtrochanteric fractures frequently result from low-energy mechanisms, such as simple falls from a standing height, superimposed upon osteopenic or osteoporotic bone. A critical, emerging subset within this demographic is the atypical femoral fracture (AFF), which is strongly associated with the prolonged utilization of anti-resorptive medications, particularly bisphosphonates and denosumab. The American Society for Bone and Mineral Research (ASBMR) has established strict major and minor criteria for AFFs, which typically present as transverse or short oblique fractures originating at the lateral cortex, often accompanied by localized periosteal or endosteal thickening ("beaking"). These atypical fractures present unique biological challenges, as the prolonged suppression of targeted bone remodeling severely blunts the normal physiological fracture healing response, necessitating specialized operative strategies and prolonged periods of protected weight-bearing.
Regardless of the etiology, the subtrochanteric region is uniquely unforgiving. Unlike the highly vascularized cancellous bone of the intertrochanteric region, the subtrochanteric femur is composed primarily of dense cortical bone with a relatively tenuous periosteal and endosteal blood supply. This watershed vascularity, combined with the massive biomechanical forces acting across the proximal femur, creates an environment where mechanical failure of the implant or biological failure of the fracture callus is a constant threat. Therefore, the contemporary orthopedic surgeon must approach these fractures not merely as an exercise in hardware application, but as a complex biomechanical reconstruction that respects the delicate biology of the proximal femur.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the deforming forces acting upon the proximal femur is the absolute, non-negotiable prerequisite for avoiding the classic malalignments—specifically varus, procurvatum, and external rotation—that historically plagued the treatment of subtrochanteric femoral fractures. The subtrochanteric region is subjected to the highest biomechanical stresses in the human skeleton. During normal physiological gait, the medial cortex experiences massive compressive forces, while the lateral cortex is subjected to profound tensile forces. These stresses can exceed 1,200 pounds per square inch, demanding an osteosynthesis construct capable of withstanding immense cyclical loading until robust cortical consolidation occurs.
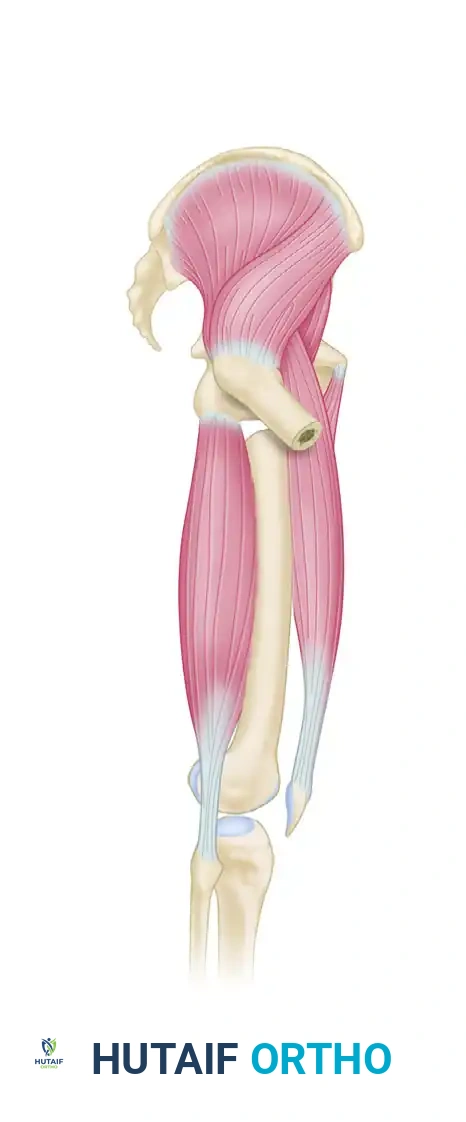
The proximal and distal fracture fragments are subjected to intense, opposing muscular pulls that predictably distort the anatomical alignment of the femur. The proximal fragment is strongly influenced by the massive abductor musculature (the gluteus medius and minimus), which insert onto the greater trochanter and forcibly abduct the segment. Simultaneously, the short external rotators pull the fragment into external rotation, while the powerful iliopsoas, inserting onto the lesser trochanter, drives the proximal segment into profound flexion. The net result of these combined vectors is a proximal fragment that rests in severe abduction, external rotation, and flexion.
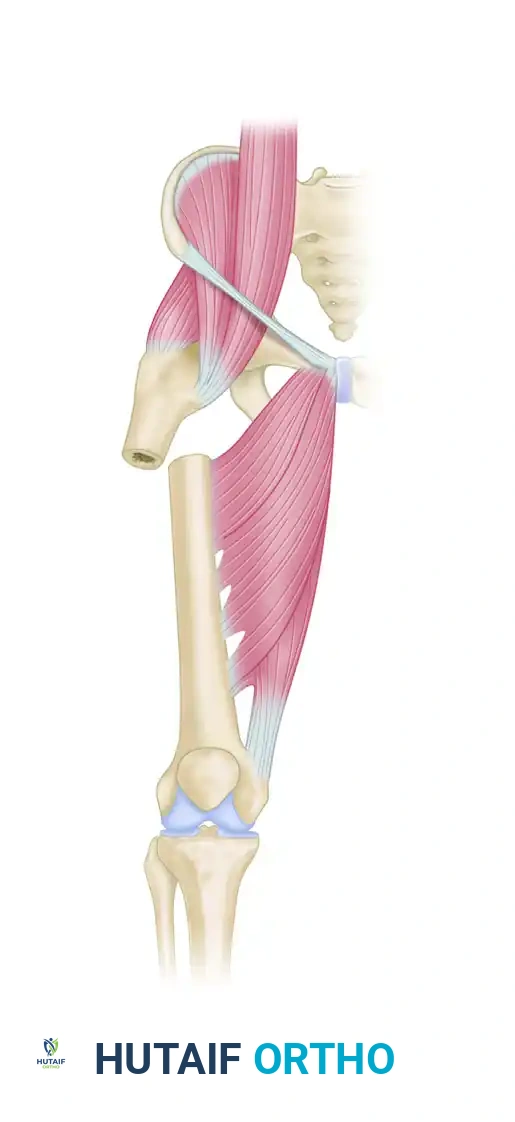
Anatomical illustration demonstrating the intact muscular forces acting across the proximal femur, highlighting the vectors of the iliopsoas, abductors, and adductors.
Deforming forces acting on a subtrochanteric femoral fracture. Note the classic flexion, abduction, and external rotation of the proximal fragment coupled with medialization and shortening of the distal fragment.
In stark contrast, the distal fragment is dominated by the adductor complex, which inserts along the linea aspera, resulting in severe medialization and adduction of the femoral shaft. Furthermore, the global deformity is exacerbated by the combined, massive pull of the quadriceps and hamstring muscle groups, which span the entire length of the femur and result in significant axial shortening of the extremity. If these deforming forces are not actively neutralized prior to the introduction of an intramedullary device, the surgeon will invariably lock the femur into a position of varus and procurvatum, severely compromising the biomechanical axis of the lower extremity and drastically increasing the risk of early implant fatigue failure.
The Russell-Taylor Classification System
To navigate this complex anatomical landscape, the Russell-Taylor Classification remains the most clinically relevant and widely utilized framework. It dictates surgical decision-making by evaluating two critical anatomical zones: the integrity of the lesser trochanter (which dictates medial calcar stability) and the extension of fracture lines into the piriformis fossa (which dictates the viability of standard entry portals).
Type I: Fractures do not extend into the piriformis fossa.
* Type IA: The lesser trochanter remains intact. These fractures possess inherent medial stability, allowing for potentially simpler reconstructive options.


- Type IB: The lesser trochanter is not intact, severely compromising medial cortical support and drastically increasing the risk of varus collapse. Reverse obliquity fractures are effectively categorized here due to their inherent biomechanical instability.

Type II: Fractures extend proximally into the piriformis fossa.
* Type IIA: The lesser trochanter is intact, but the proximal extension complicates standard piriformis entry nailing, often necessitating an alternative starting point or a specialized implant.


- Type IIB: The lesser trochanter is not intact, and the fracture extends into the piriformis fossa. This represents the most highly unstable, complex fracture pattern, absolutely requiring advanced cephalomedullary reconstruction to bypass the devastated proximal anatomy.
Exhaustive Indications and Contraindications
The management of subtrochanteric femoral fractures is almost exclusively surgical. Non-operative management is relegated to a microscopic subset of patients who are entirely non-ambulatory, possess absolute medical contraindications to anesthesia, or are in the final stages of palliative hospice care. For all other patients, surgical stabilization is mandatory to relieve pain, restore the mechanical axis, and permit early mobilization to prevent the catastrophic systemic complications of prolonged recumbency, such as deep vein thrombosis, pulmonary embolism, decubitus ulcers, and hypostatic pneumonia.
The absolute gold standard and mainstay of treatment is intramedullary nailing (IMN). Extensive biomechanical and clinical evidence unequivocally demonstrates that intramedullary implants are vastly superior to extramedullary implants (such as 95-degree dynamic condylar screws or proximal femoral locking plates) in this high-stress region. IM nails act as load-sharing devices; because they are positioned centrally within the medullary canal, they lie much closer to the mechanical axis of the femur. This central positioning drastically reduces the bending moment applied to the implant, thereby minimizing the risk of hardware fatigue and failure prior to fracture union.
While intramedullary nailing is the definitive treatment of choice, there remain highly specific, complex circumstances where extramedullary fixation is required. These include scenarios involving an obliterated medullary canal (e.g., severe Paget's disease or retained hardware that cannot be extracted), severe pediatric deformities, or highly complex proximal articular extensions where an intramedullary device would compromise the hip joint. In these rare instances, fixed-angle blade plates or modern proximal femoral locking plates, applied via minimally invasive biological plating techniques, remain highly useful in the orthopedic surgeon's armamentarium.
| Parameter | Intramedullary Nailing (Cephalomedullary) | Extramedullary Plating (Locking/Blade Plates) | Non-Operative Management |
|---|---|---|---|
| Primary Indications | Standard subtrochanteric fractures, AFFs, reverse obliquity patterns, pathologic fractures. | Obliterated medullary canal, complex proximal articular extension, retained unremovable hardware. | Non-ambulatory baseline, absolute medical contraindications to anesthesia, palliative care. |
| Biomechanical Profile | Load-sharing, short lever arm, central to mechanical axis, high resistance to bending. | Load-bearing, long lever arm, eccentric to mechanical axis, higher risk of fatigue failure. | None. Relies entirely on external splinting and prolonged skeletal traction. |
| Contraindications | Active intramedullary infection, extremely narrow canal (<8mm) not amenable to reaming. | Severe medial comminution without the ability to restore medial cortical buttress, osteoporotic bone (relative). | Ambulatory patients, poly-trauma patients requiring mobilization. |
| Advantages | Minimally invasive, preserves fracture hematoma, allows earlier weight-bearing, superior biomechanics. | Direct visualization for perfect anatomic reduction, avoids violating the piriformis fossa/abductors. | Avoids surgical and anesthetic risks. |
| Disadvantages | Difficult reduction techniques required, risk of eccentric reaming and varus malalignment. | Extensive soft tissue dissection, higher blood loss, delayed weight-bearing protocols required. | High mortality rate from prolonged recumbency, severe pain, malunion/nonunion almost certain. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful subtrochanteric fracture management. The surgeon must obtain high-quality, full-length orthogonal radiographs of the affected femur, as well as an anteroposterior (AP) radiograph of the pelvis to evaluate the uninjured contralateral side. The contralateral femur serves as the critical template for determining the native neck-shaft angle, the appropriate femoral version, and the exact length of the intramedullary nail required. In cases of high-energy trauma or highly comminuted fracture patterns, a computed tomography (CT) scan of the proximal femur is highly recommended to rule out occult extension into the femoral neck or the piriformis fossa, which would drastically alter the choice of starting portal and implant.
Templating must be performed meticulously. The surgeon should measure the isthmic diameter of the medullary canal to anticipate the required reamer sizes and the final nail diameter. It is generally recommended to over-ream the canal by 1.0 to 1.5 millimeters larger than the selected nail diameter to prevent iatrogenic hoop stresses and subsequent iatrogenic fractures during nail insertion. Furthermore, the surgeon must carefully evaluate the anterior bow (radius of curvature) of the femur. Modern intramedullary nails are manufactured with varying radii of curvature (typically ranging from 1.0 to 1.5 meters); selecting a nail with a mismatch to the patient's native anatomy can result in anterior cortical perforation distally or a failure to adequately seat the proximal portion of the nail.
The choice of patient positioning is a critical decision that is heavily influenced by the patient's body habitus, the specific characteristics of the fracture pattern, and the surgeon's comfort level. The two primary options are the supine position on a radiolucent fracture table and the lateral decubitus position on a flat radiolucent table.
Supine Positioning on a Fracture Table:
This is the preferred setup for the vast majority of subtrochanteric fractures in patients with a normal body mass index (BMI). The patient is placed supine, and the affected extremity is secured in a traction boot. The unaffected leg is typically placed in a hemilithotomy position (scissored down and away) to allow unimpeded, highly mobile access for the C-arm fluoroscopy unit. This setup allows for excellent biplanar fluoroscopic visualization and utilizes a modified medial trochanteric portal. The primary advantage is the ability to use skeletal traction to assist in restoring length and the ease of obtaining perfectly orthogonal AP and lateral fluoroscopic images without moving the patient's leg.
Lateral Decubitus Positioning:
We strongly reserve and recommend the lateral decubitus position for morbidly obese patients or those with highly complex, unstable fracture patterns requiring extensive open reduction. In obese patients, the supine position often causes the massive abdominal pannus to push the surgeon's hand, the awl, and the reamers laterally. This forced lateral trajectory inevitably creates a medialized, eccentric starting point in the greater trochanter, which mechanically forces the proximal fragment into a disastrous varus malreduction as the nail is inserted. The lateral position allows gravity to pull the adipose and soft tissues anteriorly, providing an unimpeded, perfectly collinear trajectory for the guidewire and rigid reamers. While positioning the C-arm is slightly more cumbersome, the biomechanical advantage of achieving a perfect starting portal far outweighs the logistical inconveniences.
Step-by-Step Surgical Approach and Fixation Technique
The successful intramedullary nailing of a subtrochanteric fracture relies on two absolute, non-negotiable principles: achieving anatomic, or near-anatomic, reduction prior to the commencement of reaming, and maintaining absolute trajectory control during the preparation of the proximal canal. The intramedullary nail is not a reduction tool; it is a rigid internal splint. It will permanently lock the femur in whatever alignment exists at the exact moment the rigid reamers pass across the fracture site.
1. Fracture Reduction Strategies
Due to the massive deforming forces previously described, closed reduction via longitudinal traction alone is almost universally insufficient. The surgeon must actively neutralize the flexion, abduction, and external rotation of the proximal fragment.
* Percutaneous Techniques: A ball-spike pusher, a bone hook, or a Schanz pin placed percutaneously into the proximal fragment can be used as a joystick to physically push the proximal segment out of flexion and external rotation.
* Mini-Open Techniques: The surgeon must not hesitate to make a small lateral incision to apply a collinear reduction clamp (e.g., a Jungbluth clamp or a large pointed reduction forceps) across the fracture site. Anatomic reduction of the medial cortex is paramount.
* Poller (Blocking) Screws: This is an indispensable technique. Poller screws are placed strategically in the wide proximal metaphysis to artificially narrow the medullary canal. By placing a blocking screw on the concavity of the anticipated deformity (typically posterior and medial to the desired nail path), the surgeon forces the flexible guidewire and subsequent reamers into the correct trajectory, mechanically preventing varus and procurvatum malalignment.
2. Trajectory Control and Portal Preparation
We strongly advocate for the concept of "Trajectory Control" in the treatment of these fractures. The starting point must be perfectly collinear with the medullary canal on both the AP and lateral radiographic views. For a trochanteric entry nail, the starting point is typically at the tip of the greater trochanter or slightly medial to it, depending on the specific implant design.
Once the initial guidewire is placed, the surgeon must obtain rigid anterior and lateral cortical support. We routinely utilize a specialized channel reamer or opening reamer over a rigid guide pin. Reaming through a protected tissue sleeve or utilizing a rigid trajectory control device prevents the flexible reamer shaft from migrating laterally into the softer cancellous bone of the greater trochanter—a phenomenon known as the "lateralization effect." Retrospective institutional data overwhelmingly confirms that implementing strict trajectory control and routinely using a rigid opening reamer drastically reduces the incidence of eccentric portals and subsequent varus malalignment.
3. Cephalomedullary Fixation Execution (The InterTAN Technique)
For subtrochanteric fractures, particularly those classified as Russell-Taylor IB, IIA, and IIB, the construct must be proximally locked in reconstruction mode (cephalomedullary fixation) to bypass the compromised proximal anatomy and secure fixation directly into the dense trabecular bone of the femoral head. When utilizing an integrated dual-screw cephalomedullary system like the TRIGEN InterTAN, precise stepwise execution is required to achieve optimal linear compression and rotational stability.
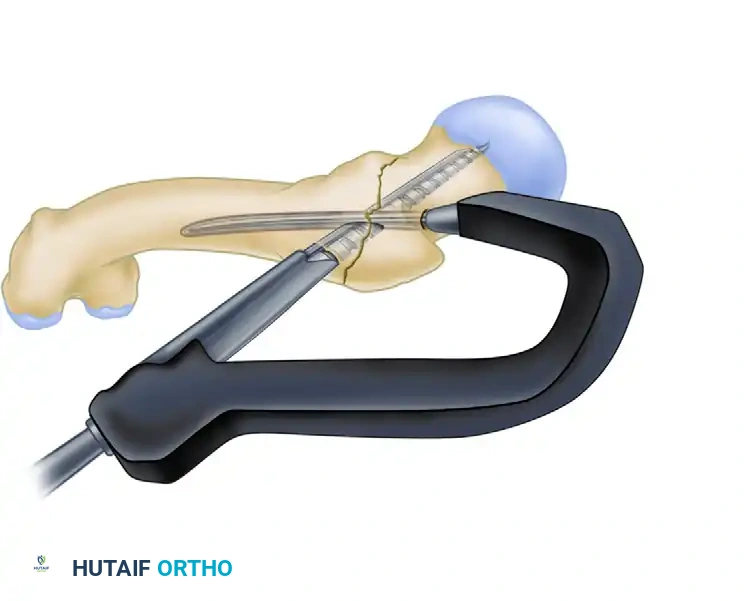
Step A: Guidewire Placement and Drilling
After the nail is seated at the correct depth (ensuring the proximal aperture aligns perfectly with the central axis of the femoral neck), the guidewire for the inferior lag screw is placed centrally within the femoral head on both AP and lateral fluoroscopic views. The trajectory is then drilled.

Drilling for the lag screw with the derotational bar in place. The derotational bar prevents the proximal fragment from spinning during the aggressive reaming process.
Step B: Lag Screw Insertion
The primary lag screw is inserted over the guidewire. This screw provides the foundational purchase within the dense subchondral bone of the femoral head. It is critical to achieve a tip-apex distance (TAD) of less than 25 millimeters to minimize the risk of hardware cut-out.
Insertion of the primary lag screw into the femoral head.
Step C: Integrated Compression Screw Insertion
The secondary, integrated compression screw is then inserted through the same proximal portal of the nail. As this smaller screw engages the primary lag screw, it creates an active, controlled linear compression across the fracture site (if the fracture pattern allows for compression) and provides exceptional, rigid rotational stability, vastly superior to single-screw constructs.

Insertion of the integrated compression screw, locking the construct and providing rotational control.
Step D: Final Construct Verification
Meticulous fluoroscopy is used to confirm the final seating of the cephalomedullary screws, ensuring no joint penetration into the acetabulum and verifying the absolute restoration of the native neck-shaft angle.

Final integrated construct demonstrating the interlocking mechanism of the cephalomedullary screws.
4. Distal Interlocking
Distal interlocking is performed using a "perfect circles" freehand technique under fluoroscopy. For subtrochanteric fractures, which are inherently length-unstable and subjected to immense rotational torque, a minimum of two distal locking screws is absolutely recommended. In cases of severe comminution or poor bone quality, dynamically locking the nail (if the system permits and the fracture is length-stable) may promote secondary bone healing via micromotion, though static locking remains the safest default to prevent catastrophic shortening.
Complications, Incidence Rates, and Salvage Management
Despite advancements in implant metallurgy and surgical technique, subtrochanteric fractures remain fraught with potential complications. The hostile biomechanical environment and the often-precarious vascular supply to the cortical diaphysis combine to create a perfect storm for both mechanical and biological failures. Recognizing these complications early and understanding the complex salvage procedures required is a vital skill set for the orthopedic traumatologist.
Varus malunion remains the most frequent and devastating technical error, often stemming from an eccentric starting point or a failure to neutralize the deforming forces prior to reaming. A varus deformity shifts the mechanical axis medially, exponentially increasing the bending moment on the intramedullary nail and almost guaranteeing eventual fatigue failure of the hardware if the fracture does not unite rapidly. Nonunion, classified as either hypertrophic (mechanical instability) or atrophic (biological failure), occurs in up to 10% of cases, particularly in atypical femoral fractures where the inherent bone biology is severely compromised by bisphosphonate therapy.
| Complication | Estimated Incidence | Primary Etiology | Salvage Management Strategy |
|---|---|---|---|
| Varus Malunion | 5% - 15% | Eccentric starting portal, failure to counteract abductors/iliopsoas during reduction. | Corrective valgus-producing subtrochanteric osteotomy, exchange nailing, or robust fixed-angle plating. |
| Nonunion (Atrophic/Hypertrophic) | 2% - 10% | Biological impairment (AFFs, smoking), inadequate stability, excessive fracture gap. | Exchange nailing (over-reaming by 2mm), application of autologous bone graft (RIA), augmentative plating. |
| Implant Failure (Nail Breakage) | 1% - 5% | Prolonged nonunion leading to fatigue failure, typically occurring at the lag screw aperture. | Hardware extraction (often requiring specialized broken nail kits), re-reaming, larger diameter revision IMN with bone grafting. |
| Hardware Cut-Out | 2% - 6% | Poor proximal screw placement (TAD > 25mm), severe osteoporosis, uncorrected varus. | Removal of hardware, revision to a longer cephalomedullary device, or conversion to total hip arthroplasty (THA) in the elderly. |
| Infection (Deep) | 1% - 3% | Open fractures, severe soft tissue compromise, prolonged operative times, medical comorbidities. | Radical surgical debridement, hardware removal (if unstable), antibiotic cement spacer/nail, culture-directed IV antibiotics. |
Salvage management for a failed subtrochanteric reconstruction is a massive undertaking. In cases of aseptic nonunion with intact hardware, the traditional approach involves exchange nailing—removing the existing nail, aggressively reaming the canal to stimulate endosteal bleeding (the "internal bone graft" effect), and inserting a larger diameter nail. However, contemporary literature increasingly supports the use of augmentative plating. This involves leaving the intramedullary nail in situ and applying a lateral compression plate across the nonunion site, often supplemented with autologous bone graft harvested via a Reamer-Irrigator-Aspirator (RIA) system. This dual-construct technique provides unparalleled biomechanical stability, neutralizing rotational and bending forces while delivering a massive biological stimulus to the dormant fracture site.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must be meticulously tailored to the individual patient, heavily dictated by the specific fracture pattern, the inherent quality of the host bone, and the surgeon's intraoperative assessment of construct stability. A generalized, one-size-fits-all approach is inappropriate and can lead to premature hardware failure or severe joint stiffness.
Phase I: Acute Post-Operative Period (0-2 Weeks)
The immediate focus is on medical stabilization, deep vein thrombosis (DVT) prophylaxis, and early mobilization to prevent the complications of recumbency. For patients with standard subtrochanteric fractures treated with a robust cephalomedullary device (such as the InterTAN) and possessing good cortical bone stock, immediate weight-bearing as tolerated (WBAT) is generally permitted and encouraged. The load-sharing nature of the IM nail and the superior rotational stability of the dual-screw proximal fixation typically support this early mechanical loading, which can actually stimulate secondary bone healing via controlled micromotion. Physical therapy focuses on passive and active-assisted range of motion (ROM) of the hip and knee, as well as isometric quadriceps and gluteal sets.
Phase II: Intermediate Rehabilitation (2-6 Weeks)
In cases of highly unstable fracture patterns (e.g., severe medial comminution, reverse obliquity with extensive distal diaphyseal extension) or profound osteoporosis, weight-bearing may need to be strictly modified. In these scenarios, patients are typically restricted to toe-touch weight-bearing (TTWB) or flat-foot weight-bearing (maximum 20 lbs of force) for the first 4 to 6 weeks. During this phase, therapy intensifies to include active ROM, progressive abductor strengthening (avoiding heavy resistance that stresses the greater trochanter), and gait training with assistive devices. Serial radiographs are obtained at the 2-week and 6-week marks to monitor for the maintenance of alignment and to rule out early varus collapse or hardware migration.
Phase III: Advanced Rehabilitation and Maturation (6-12+ Weeks)
As radiographic evidence of bridging callus emerges (typically visible by
