Subtalar Dislocations: Comprehensive Operative Management and Surgical Techniques

Key Takeaway
Subtalar dislocations involve the simultaneous displacement of the calcaneus, cuboid, navicular, and forefoot from the talus. Medial dislocations are most common and often reducible closed, whereas lateral dislocations frequently require open reduction due to soft tissue interposition. This guide details the biomechanics, reduction techniques, surgical approaches, and postoperative protocols essential for achieving congruent joint reduction and optimizing patient outcomes.
INTRODUCTION TO SUBTALAR DISLOCATIONS
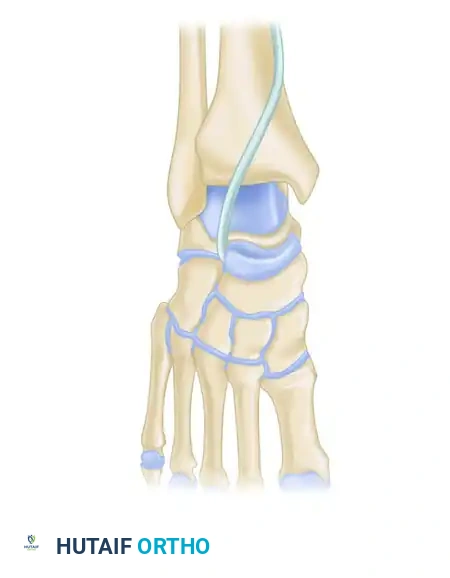
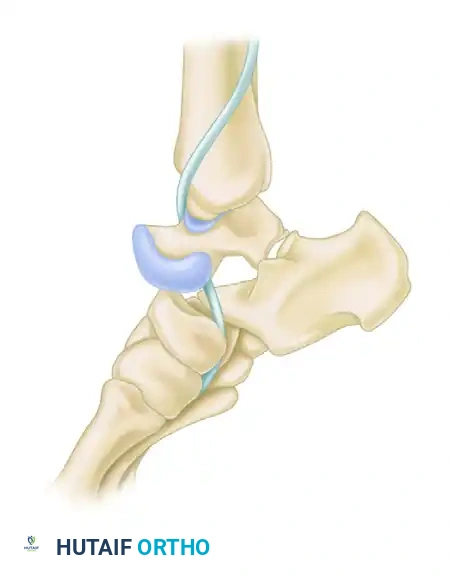
Subtalar dislocations, accurately termed peritalar dislocations, represent a severe and complex disruption of the hindfoot architecture. In this injury pattern, the calcaneus, cuboid, navicular, and the entire forefoot become simultaneously displaced from the talus. The tibiotalar and calcaneocuboid articulations typically remain intact, while the talocalcaneal (subtalar) and talonavicular joints are completely dislocated.
These injuries are relatively rare, accounting for approximately 1% to 2% of all joint dislocations, and are typically the result of high-energy trauma such as motor vehicle collisions, falls from a height, or severe athletic injuries. Prompt recognition, emergent reduction, and meticulous evaluation for associated osteochondral fractures are paramount to preventing devastating long-term complications, including avascular necrosis (AVN) of the talus, post-traumatic arthritis, and chronic hindfoot stiffness.
Clinical Pearl: The term "subtalar dislocation" is a misnomer. Because the calcaneocuboid joint remains intact, the entire acetabulum pedis (calcaneus, navicular, and ligaments) dislocates as a single unit around the talus. It is truly a peritalar dislocation.
CLASSIFICATION AND BIOMECHANICS
Subtalar dislocations are classified based on the direction of the distal foot segment relative to the talus.
Medial Subtalar Dislocations
Medial dislocations are the most common, comprising approximately 80% of all peritalar dislocations. The mechanism of injury is typically a severe inversion force applied to a plantarflexed foot. The sustentaculum tali acts as a fulcrum, levering the talus out of its anatomic position.
Clinically, the foot presents in an acquired clubfoot posture—supinated and medially displaced. The head of the talus becomes highly prominent dorsolaterally, and the skin over the talar head is frequently blanched and under extreme tension.
Clinical posture of a medial subtalar dislocation. Note the extreme prominence of the head of the talus dorsolaterally and the acquired clubfoot deformity.
Lateral Subtalar Dislocations
Lateral dislocations account for 15% to 20% of cases and result from a forceful eversion of the foot. The anterior process of the calcaneus acts as the fulcrum. The foot appears pronated and laterally displaced, resembling an acquired flatfoot deformity. The talar head is prominent medially. Lateral dislocations are associated with higher energy trauma, a greater incidence of open fractures, and a significantly higher rate of irreducibility due to soft tissue interposition.

Clinical presentation of a lateral subtalar dislocation. The foot is laterally translated, and the medial skin is severely compromised.
Anterior and Posterior Dislocations
Anterior and posterior dislocations are exceedingly rare (less than 1% combined) and are often associated with extensive ligamentous tearing and severe crushing mechanisms.
INITIAL EVALUATION AND IMAGING
Clinical Assessment
Immediate assessment must focus on the soft tissue envelope and neurovascular status. Skin tenting over the prominent talar head is a surgical emergency; failure to reduce the dislocation promptly will result in full-thickness skin necrosis. The posterior tibial and dorsalis pedis pulses must be palpated and documented. The tibial nerve is particularly vulnerable to traction injury in lateral dislocations.
Radiographic Evaluation
Standard trauma radiographs of the ankle (AP, lateral, and mortise) and foot (AP, lateral, and oblique) are required.

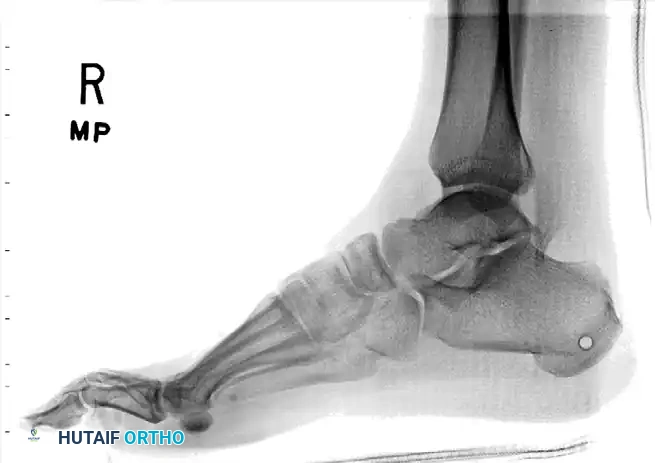
Radiographic appearance of a medial subtalar dislocation. The talonavicular and talocalcaneal joints are completely disrupted.
Radiographs demonstrating a lateral subtalar dislocation before and after reduction.
The Critical Role of Computed Tomography (CT)
The importance of obtaining a CT scan after reduction of the subtalar dislocation cannot be overstated. Patients who sustain a subtalar dislocation frequently have additional osteochondral abnormalities that are initially missed on plain radiographs.
Surgical Warning: We routinely use CT for the post-reduction evaluation of these injuries. Up to 60% of peritalar dislocations have associated fractures (e.g., talar head, navicular, calcaneal facets) that require operative treatment because of intraarticular displacement or fragments blocking congruent reduction.

After closed reduction of the dislocation, no fracture is apparent on the standard lateral radiograph.

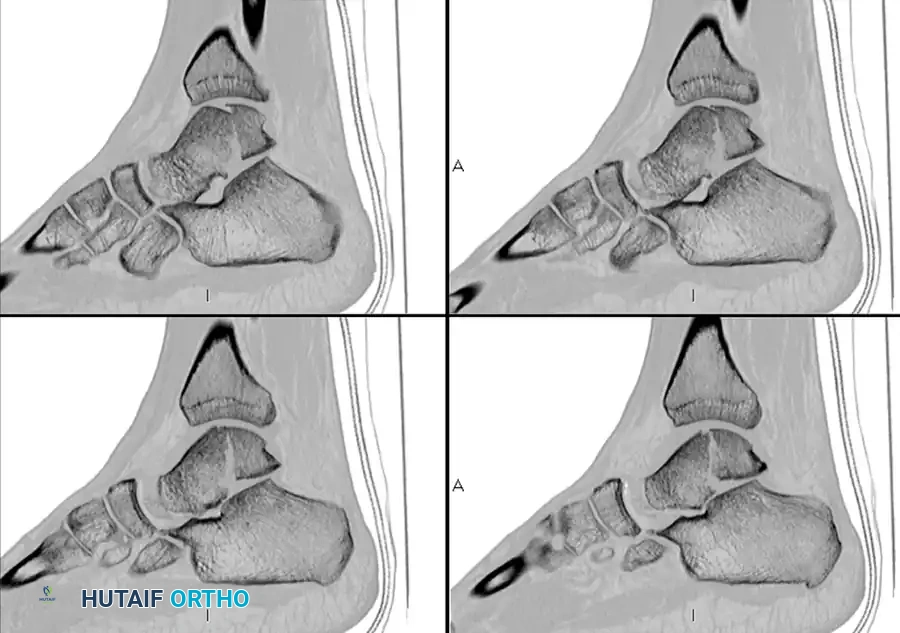
CT scans of the same patient, however, clearly demonstrate an intraarticular talar fracture requiring fixation.

Radiographic appearance after open reduction and internal fixation of the identified talar fracture.
MANAGEMENT ALGORITHM
The treatment algorithm for subtalar dislocations is dictated by the reducibility of the joint, the integrity of the soft tissues, and the presence of associated fractures.
- Closed, Reducible Dislocations (No intraarticular fragments): Treated with a non–weight-bearing cast for 6 weeks.
- Irreducible Dislocations: Require emergent open reduction to remove interposed soft tissues or bone fragments.
- Open Dislocations or Severe Soft Tissue Swelling: Successfully treated with an external fixator for 6 weeks to maintain alignment while allowing soft tissue resuscitation.
- Dislocations with Displaced Intraarticular Fractures: Require open reduction and internal fixation (ORIF) to restore joint congruity.
CLOSED REDUCTION TECHNIQUES
Closed reduction should be attempted emergently in the emergency department under conscious sedation or in the operating room under general anesthesia. Adequate muscle relaxation is critical.
Technique for Medial Dislocation
- Positioning: The patient is supine. The knee is flexed to 90 degrees to relax the gastrocnemius-soleus complex.
- Maneuver: The surgeon grasps the heel with one hand and the forefoot with the other.
- Exaggeration: The deformity is initially exaggerated by plantarflexing and further inverting the foot to disengage the navicular from the talar neck.
- Traction: Strong longitudinal traction is applied in the line of the deformity.
- Reduction: While maintaining traction, the foot is forcefully everted and dorsiflexed. A palpable "clunk" typically signifies successful reduction.
Technique for Lateral Dislocation
- Positioning: Knee flexed to 90 degrees.
- Maneuver: Exaggerate the deformity by plantarflexing and everting the foot.
- Traction: Apply longitudinal traction.
- Reduction: Forcefully invert and dorsiflex the foot.
OPEN REDUCTION: SURGICAL APPROACHES AND OBSTACLES
When closed reduction fails, soft tissue or bony interposition must be assumed. The surgical approach is dictated by the direction of the dislocation.
Irreducible Medial Dislocations
Medial subtalar dislocations without marginal fractures of the calcaneus or talus are almost always reducible by closed means. When irreducible, the block is typically lateral.
* Offending Structures: The extensor retinaculum, the extensor digitorum brevis (EDB) muscle belly, or the talonavicular joint capsule becomes interposed.
* Surgical Approach: Open reduction requires a lateral approach (Ollier or anterolateral incision) over the sinus tarsi to extract the interposed EDB or retinaculum from the subtalar joint.
Irreducible Lateral Dislocations
Lateral subtalar dislocations frequently are irreducible by closed manipulation. The talar head is driven medially through the joint capsule, trapping medial structures.
* Offending Structures: The most common offending structures blocking reduction are the posterior tibial tendon (PTT) and osteochondral fractures of the talus or navicular. The PTT often wraps around the talar neck, creating a noose effect.
* Surgical Approach: These must be approached medially. An anteromedial incision is made centered over the prominent talar head.

Intraoperative view of an irreducible lateral dislocation. The posterior tibial tendon is acting as a physical obstacle to reduction, tightly bowstrung across the talar neck.
The posterior tibial tendon is identified and marked with a rubber band. It must be carefully mobilized and lifted over the talar head.

Successful reduction of the subtalar joint after removal of the interposed posterior tibial tendon and clearance of the fracture debris.
MANAGEMENT OF SEVERE OPEN DISLOCATIONS
Patients with open fractures and associated fractures generally have a significantly poorer prognosis than those with isolated closed dislocations. High-energy open peritalar dislocations are fraught with complications, including deep infection, massive soft tissue loss, and a high rate of talar osteonecrosis (occurring in up to one-third of severe cases).

Severe open fracture-dislocation with near-complete extrusion of the talus. The soft tissue envelope is catastrophically compromised.
External Fixation
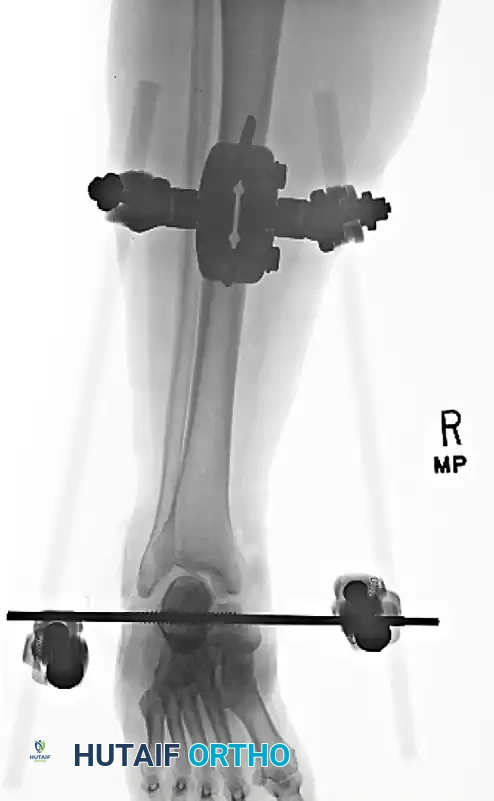
In cases of severe soft tissue swelling, gross instability post-reduction, or open injuries requiring serial debridement, spanning external fixation is the treatment of choice. A delta frame or a medial spanning fixator (tibia to first metatarsal and calcaneus) maintains length, alignment, and joint congruity while allowing access for wound care.

Application of a spanning external fixator to hold the reduction and stabilize the soft tissue envelope in a severe open dislocation.
Salvage Procedures
In long-term reviews of severe open subtalar dislocations, approximately half of the patients eventually require some form of arthrodesis due to intractable pain, AVN, or post-traumatic arthritis.
Salvage tibiocalcaneal arthrodesis utilizing a retrograde intramedullary nail and femoral head allograft for a patient with severe post-traumatic talar AVN and collapse following an open dislocation.
ASSOCIATED MIDFOOT INJURIES: NAVICULAR, CUBOID, AND CUNEIFORM FRACTURES
Subtalar dislocations rarely occur in isolation; the energy is often transmitted through the midfoot, resulting in associated fractures of the navicular, cuboid, or cuneiforms.
Navicular Body Fractures
Navicular body fractures are classified into three types, and treatment is dictated by the fracture pattern.
* Type I: Transverse fracture plane. A satisfactory reduction is usually obtainable.
* Type II & III: Comminuted and displaced. Reduction is significantly more difficult.
Surgical Technique for Navicular Fractures:
An approach is made over the anteromedial hindfoot in the interval between the anterior and posterior tibial tendons.
Surgical Warning: The periosteum of the navicular must not be aggressively elevated, as the blood supply to the navicular is tenuous and enters dorsally and plantarly. Stripping the periosteum increases the risk of AVN.
The joints are inspected and cleared of debris before fixation. Fixation is usually obtained with smooth Kirschner wires and small fragment AO screws when the size of the fragment permits.

Preoperative imaging of a complex navicular body fracture associated with midfoot disruption.

Intraoperative fluoroscopy demonstrating provisional fixation of the navicular with Kirschner wires.

Definitive fixation achieved with small fragment AO screws.

Postoperative radiograph confirming restoration of the talonavicular articular surface.
Management of Medial Column Shortening
If collapse of the navicular occurs resulting in medial column shortening, aggressive intervention is required to prevent a severe planovalgus deformity. Options include:
1. Bone Grafting: Structural autograft to restore length.
2. External Fixation: A small external fixator can be used to distract and maintain medial column length. It can be removed at 6 weeks to start range of motion, though the patient remains non-weight-bearing for 12 weeks.
3. Bridge Plating: Temporary bridge plating from the talar neck to the first metatarsal can maintain length in cases of severe comminution, though it requires a second surgery for hardware removal. Alternatively, bridge plating from the navicular to the medial and middle cuneiforms can be used, which does not interfere with talonavicular motion.
Application of a medial column external fixator to maintain length and alignment in a highly comminuted navicular fracture.
Alternative technique utilizing temporary bridge plating to span the zone of comminution and preserve medial column length.
Navicular Stress Fractures
Navicular stress fractures are frequent causes of arch pain in athletes. Because many of these fractures are not clearly identified on routine radiographs, a high index of suspicion is necessary.
* Clinical Signs: Midfoot tenderness over the navicular; irritability with eversion and inversion stress.
* Pathoanatomy: Fractures are usually located in the sagittal plane, involving the central third of the navicular bone. This area represents a relatively avascular watershed zone, as the blood supply enters from the medial, dorsal, and plantar surfaces and radiates toward the center.
* Treatment: A meta-analysis found that 6 to 8 weeks of strictly non–weight-bearing cast immobilization is the standard of care, often yielding better outcomes than surgery. Allowing the patient to bear weight is clearly inferior and leads to nonunion. If surgical treatment is required (for displaced fractures or nonunions), a percutaneous screw technique can be used for nondisplaced variants, while open bone grafting is reserved for established nonunions.
Cuboid and Cuneiform Fractures
Cuboid and cuneiform fractures are rare as isolated injuries and are often missed on initial presentation.
Clinical Pearl: Suspicion should be heightened for cuboid/cuneiform injuries if the patient presents with ecchymosis in the plantar arch. While originally described as a pathognomonic sign for Lisfranc injuries, plantar ecchymosis is equally applicable as a warning sign for severe midfoot crush injuries and cuboid fractures.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The rehabilitation protocol must balance the need for joint stability with the prevention of debilitating hindfoot stiffness.
- Immobilization Phase (0-6 Weeks):
- For closed, stable reductions: The patient is placed in a well-molded, short-leg cast and remains strictly non-weight-bearing for 6 weeks.
- For external fixators: Pin site care is performed daily. The frame remains in place for 6 weeks.
- Transition Phase (6-8 Weeks):
- At 6 weeks, the cast or external fixator is removed.
- If a congruent reduction is verified on CT and there is no residual instability, the patient is transitioned to a controlled ankle motion (CAM) boot.
- Progressive weight-bearing is initiated.
- Rehabilitation Phase (8+ Weeks):
- Aggressive physical therapy focuses on restoring subtalar and transverse tarsal motion.
- Strengthening of the peroneal and posterior tibial tendons is emphasized to provide dynamic stability to the hindfoot.
OUTCOMES AND COMPLICATIONS
The prognosis of a subtalar dislocation is directly correlated with the energy of the injury, the direction of the dislocation, and the presence of associated fractures.
- Stiffness: The most common complication. Virtually all patients will experience some loss of subtalar inversion and eversion. Early mobilization (at 6 weeks) is critical to minimizing this.
- Post-Traumatic Arthritis: High incidence in both medial and lateral dislocations, particularly if there was unrecognized osteochondral damage. Arthrodesis (subtalar or triple) may eventually be required.
- Avascular Necrosis (AVN): While less common than in talar neck fractures, AVN of the talar body occurs in up to 33% of severe, open subtalar dislocations due to the massive disruption of the peritalar anastomotic sling.
- Lateral vs. Medial Prognosis: Lateral dislocations tend to have a poorer prognosis than medial dislocations because they are associated with higher energy, more severe
You Might Also Like

