INTRODUCTION TO DISTAL TIBIAL ARTICULAR INJURIES
The management of unstable ankle fracture-dislocations and tibial pilon (plafond) fractures represents one of the most formidable challenges in orthopedic trauma surgery. These injuries encompass a broad spectrum of skeletal disruption, ranging from low-energy rotational fractures to devastating high-energy axial compression injuries typically sustained in motor vehicle collisions or falls from significant heights.
Historically, aggressive early open reduction and internal fixation (ORIF) of high-energy pilon fractures led to catastrophic soft tissue complications, including deep infection, wound necrosis, and amputation. Consequently, modern orthopedic principles dictate a deep respect for the soft tissue envelope, heavily favoring a staged approach to reconstruction. This comprehensive guide delineates the biomechanics, classification, preoperative planning, and step-by-step surgical execution required to achieve optimal outcomes in these complex injuries.
BIOMECHANICS AND MECHANISM OF INJURY
The morphology of a distal tibial fracture is directly dictated by the vector and magnitude of the deforming force, as well as the position of the foot at the moment of impact.
- Rotational Forces: Low-energy rotational variants typically carry a more favorable prognosis. Lauge-Hansen described a pronation-dorsiflexion injury resulting in an oblique medial malleolar fracture, a large anterior lip fracture, a supra-articular fibular fracture, and a posterior tibial fracture. Similarly, Giachino and Hammond identified a pattern driven by external rotation, dorsiflexion, and abduction, yielding an oblique medial malleolus fracture combined with an anterolateral tibial plafond fracture. These injuries generally exhibit minimal metaphyseal comminution and forgiving soft tissue envelopes.
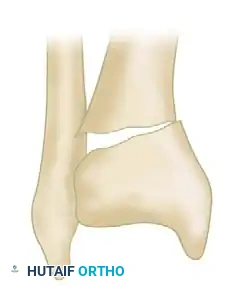
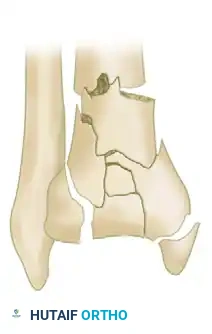
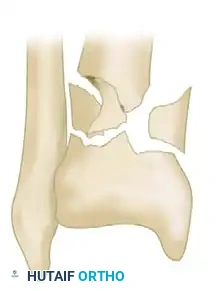
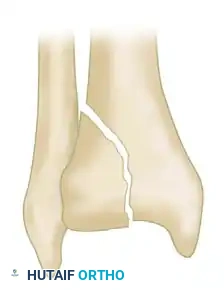
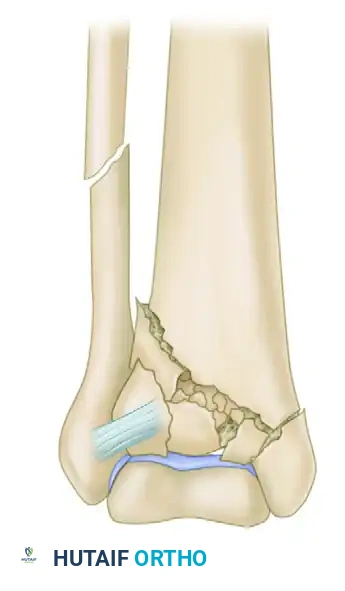
- Axial Compression Forces: High-energy axial loads drive the talus into the distal tibial articular surface like a die-punch. This results in severe articular impaction, explosive metaphyseal comminution, and diaphyseal extension. The fibula is fractured in approximately 85% of these cases, and concomitant talar chondral or osteochondral injuries are frequent.
💡 Clinical Pearl: The "Ground-Glass" Phenomenon
Dickson, Montgomery, and Field identified a highly prognostic subset of severe pilon fractures characterized by "ground-glass" comminution—defined as more than three articular fragments smaller than 2 mm on CT scan. In their series, post-traumatic arthritis developed in 38% of ankles with ground-glass comminution, compared to 0% in those without it, underscoring the limits of anatomical reconstruction in explosive injuries.
CLASSIFICATION SYSTEMS
Accurate classification is paramount for determining prognosis, guiding surgical strategy, and facilitating academic communication. While interobserver reliability for these systems is moderate, they remain indispensable.
The AO/OTA Classification
The Orthopaedic Trauma Association (OTA) system provides the most comprehensive anatomical description of distal tibial fractures, dividing them into three primary types based on articular involvement:
-
Type A (Extra-articular): Fractures involving the distal metaphysis without extension into the tibiotalar joint. Subdivided into A1 (simple), A2 (wedge), and A3 (complex/multifragmentary).
-
Type B (Partial Articular): A portion of the articular surface remains in continuity with the tibial diaphysis. Subdivided into B1 (pure split), B2 (split depression), and B3 (multifragmentary depression).
-
Type C (Complete Articular): The articular surface is entirely disconnected from the diaphysis. Subdivided into C1 (articular simple, metaphysis simple), C2 (articular simple, metaphysis multifragmentary), and C3 (articular multifragmentary).
The Rüedi and Allgöwer Classification
This classic system categorizes pilon fractures based on the degree of displacement and comminution:
-
Type I: Nondisplaced cleavage fractures involving the joint surface.
-
Type II: Cleavage-type fractures with significant displacement of the articular surface but minimal comminution.

-
Type III: Severe injuries associated with extensive metaphyseal and articular comminution.

Further morphological variations include isolated split depressions and severe metaphyseal comminution, which dictate the necessity for bone grafting and buttress plating.


CLINICAL EVALUATION AND SOFT TISSUE ASSESSMENT
The ultimate determinant of surgical timing is the condition of the soft tissue envelope. High-energy pilon fractures are frequently associated with severe closed soft tissue trauma or open wounds.
- Vascular and Neurological Exam: Rule out vascular injury, compartment syndrome, and closed degloving injuries (Morel-Lavallée lesions).
- Fracture Blisters: The presence of fracture blisters indicates severe cutaneous damage. Clear fluid blisters represent epidermal separation, whereas blood-filled blisters indicate deeper dermal injury and a higher risk of full-thickness necrosis.
- Classification of Soft Tissue Injury: Open fractures must be graded using the Gustilo-Anderson system. Closed injuries should be meticulously graded using the Tscherne classification (Grades 0-III).
- Patient Optimization: Smoking, poorly controlled diabetes, peripheral vascular disease, and alcoholism exponentially increase the risk of postoperative wound complications and nonunion.
PREOPERATIVE IMAGING AND PLANNING
Standard anteroposterior (AP), lateral, and mortise radiographs of the ankle are mandatory. However, plain films drastically underestimate the complexity of articular impaction.
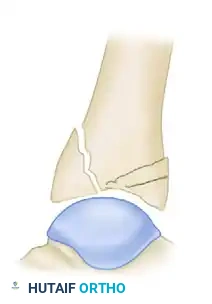
- Traction Radiographs: Applying longitudinal traction (via a calcaneal pin or spanning external fixator) during radiography demonstrates the degree to which ligamentotaxis can reduce the fracture.
- Computed Tomography (CT): A fine-cut CT scan with 2D and 3D reconstructions is the gold standard. Crucially, the CT scan should be obtained after the application of a spanning external fixator. This provides an accurate map of the remaining impacted articular segments that will require direct open reduction, as ligamentotaxis alone cannot elevate central die-punch fragments.
STABILIZATION OF UNSTABLE ANKLE FRACTURE-DISLOCATION
In scenarios of severe instability, profound soft tissue compromise, or polytrauma where immediate definitive fixation is contraindicated, temporary stabilization is required. The Childress transarticular pinning technique is a rapid, effective damage-control maneuver.
🚨 Surgical Warning: Transarticular Pinning
Transarticular pinning violates the subtalar and tibiotalar joints. It should be reserved strictly for highly unstable fracture-dislocations where a spanning external fixator is unavailable or contraindicated, or as a temporary measure in austere environments.
🔪 Surgical Technique: Transarticular Pinning (Childress)
- Positioning and Reduction: Place the patient supine. Perform a closed reduction of the fracture-dislocation under fluoroscopic guidance. Obtain true AP and lateral radiographic views to confirm the restoration of the mechanical axis.
- Guidewire Placement: Tape a Kirschner wire longitudinally on the medial side of the ankle, exactly in the midline, to serve as a radiographic reference marker.
- Pin Insertion: Using the taped K-wire as a fluoroscopic guide, introduce a 2.8-mm smooth Steinmann pin into the midline of the plantar sole, precisely 2.5 cm posterior to the calcaneocuboid joint.
- Advancement: Aim the pin directly toward the anatomical center of the tibial plafond. Advance the pin through the calcaneus, across the talus, and approximately 10 cm into the distal tibial metaphysis.
- Verification: Confirm the trajectory and fracture reduction with orthogonal C-arm views.
- Pin Management: Leave 1.3 cm of the Steinmann pin protruding through the plantar skin. Pad the pin site meticulously to prevent pressure necrosis.
- Immobilization: Apply a well-padded, long-leg plaster cast. Crucial detail: Do not incorporate the protruding end of the pin directly into the rigid cast material, as micro-motion can lead to pin-tract infection.
Postoperative Protocol for Childress Pinning:
The long-leg cast is transitioned to a short-leg cast at 4 to 6 weeks. The Steinmann pin is removed in the clinic at 4 to 8 weeks, contingent upon radiographic callus formation and the inherent stability of the fracture pattern. Strict non-weight-bearing (NWB) is enforced until the pin is removed.
SURGICAL MANAGEMENT OF TIBIAL PILON FRACTURES
The ultimate goals of pilon fracture surgery are:
1. Anatomical restoration of the articular surface.
2. Restoration of mechanical alignment (length, rotation, and axis).
3. Stable internal fixation to allow early range of motion.
4. Avoidance of soft tissue complications.
The Shift to Two-Stage Delayed ORIF
In the 1980s and early 1990s, early ORIF of high-energy (Rüedi-Allgöwer Type III / AO Type C3) pilon fractures yielded disastrous results. McFerran et al. reported a 54% local complication rate, with deep infections frequently necessitating free tissue transfer or amputation. Watson et al. demonstrated that basing treatment on the Tscherne soft tissue grade significantly improved outcomes.
Today, the Two-Stage Delayed Protocol is the gold standard for high-energy pilon fractures.
Stage 1: Damage Control External Fixation
Performed within 24 hours of injury. A spanning delta-frame external fixator is applied.
* Construct: Two half-pins are placed in the tibial diaphysis (well proximal to the zone of injury and future plate trajectories). A centrally threaded transfixion pin is placed through the calcaneus.
* Fibular Fixation: If the fibula is fractured, early ORIF of the fibula can be performed during this stage to restore lateral column length, provided the lateral soft tissue envelope is pristine. If lateral tissues are compromised, fibular fixation is delayed.
* Ligamentotaxis: The frame is distracted to restore length and roughly align the metaphyseal fragments.
Stage 2: Definitive ORIF
Definitive surgery is delayed for 10 to 21 days until the soft tissue envelope has recovered. The clinical indicator for readiness is the resolution of edema, marked by the appearance of the "wrinkle sign" and epithelialization of fracture blisters.
🔪 Surgical Technique: Definitive ORIF
1. Surgical Approaches:
The choice of approach is dictated by the location of the primary articular fracture lines (identified on the post-ex-fix CT scan).
* Anterolateral Approach: Utilized for valgus deformity and anterolateral (Chaput) fragments. The incision is made in line with the fourth ray, developing the interval between the Tibialis Anterior and Extensor Digitorum Longus (EDL).
* Anteromedial Approach: Utilized for varus deformity and large medial malleolar fragments. The incision runs medial to the Tibialis Anterior tendon.
* Rule of Angiosomes: If dual incisions (e.g., medial and lateral) are required, a minimum skin bridge of 7 cm must be maintained to prevent catastrophic skin necrosis.
2. Articular Reconstruction:
* The joint capsule is opened to visualize the plafond.
* Impacted central articular fragments (die-punch) are elevated using an osteotome or periosteal elevator.
* The articular surface is provisionally assembled using fine K-wires.
* Once anatomical congruity is achieved, the fragments are secured with 2.7-mm or 3.5-mm independent lag screws.
3. Metaphyseal Bone Grafting:
Elevation of impacted articular segments inevitably leaves a metaphyseal void. This defect must be filled with cancellous autograft (iliac crest), allograft, or osteoinductive bone substitutes to support the articular surface and prevent late subsidence.
4. Plate Fixation:
The reconstructed articular block is then mated to the tibial diaphysis using a pre-contoured anatomical locking plate. Minimally invasive percutaneous osteosynthesis (MIPO) techniques are highly encouraged to preserve the periosteal blood supply.
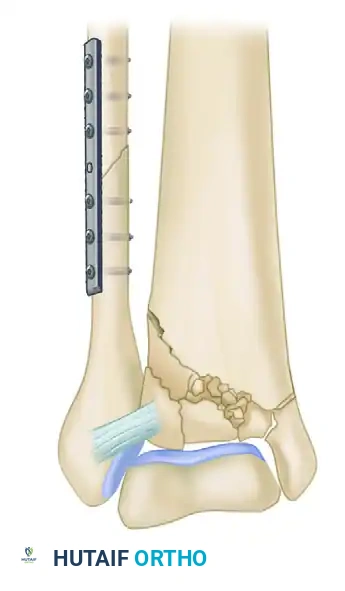

Clinical Example: Postoperative radiographs demonstrating restoration of the articular mortise and stable metaphyseal fixation using a medial locking plate and independent lag screws.
POSTOPERATIVE CARE AND REHABILITATION
- Wound Management: Incisions are closed meticulously without tension. Negative pressure wound therapy (NPWT) over closed incisions may be utilized to reduce edema and seroma formation.
- Immobilization: The ankle is splinted in neutral dorsiflexion.
- Range of Motion: Active and active-assisted range of motion (ROM) of the ankle and subtalar joints is initiated at 2 to 3 weeks postoperatively, once incisions are fully healed.
- Weight-Bearing: Patients are maintained strictly non-weight-bearing for 10 to 12 weeks. Progressive weight-bearing is initiated only after radiographic evidence of bridging callus across the metaphyseal fracture lines.
PROGNOSIS AND LONG-TERM OUTCOMES
The prognosis of tibial pilon fractures is heavily dependent on the initial energy of the injury. Poor prognostic indicators include:
* AO Type C3 / Rüedi-Allgöwer Type III comminution.
* Concomitant talar dome lesions.
* Severe soft tissue injury (open fractures or Tscherne Grade III).
* Inability to achieve an anatomical articular reduction (>2 mm step-off).
Interestingly, while anatomical reduction minimizes the risk of severe post-traumatic arthrosis, it does not guarantee a perfect clinical outcome. Studies by DeCoster et al. and Williams et al. have shown that radiographic arthrosis does not always correlate linearly with clinical ankle scores. Long-term functional outcomes, as measured by the SF-36, are often negatively impacted by persistent stiffness, chronic swelling, and socioeconomic factors.
In cases of severe, non-reconstructable articular destruction with massive soft tissue loss, primary ankle arthrodesis or even early amputation may be the most functional and definitive treatment pathway, sparing the patient years of reconstructive failures.
