STABILIZATION OF THE “TERRIBLE TRIAD” ELBOW FRACTURE-DISLOCATION
The "terrible triad" of the elbow is a complex fracture-dislocation characterized by a posterior or posterolateral dislocation of the ulnohumeral joint, accompanied by fractures of both the radial head and the coronoid process of the ulna. Historically associated with dismal outcomes due to chronic instability, arthrosis, and profound stiffness, modern orthopedic management dictates a highly systematic, biomechanically driven surgical approach.
The primary goal of surgical intervention is the restoration of concentric joint stability to permit early, active range of motion (ROM). This requires a sequential reconstruction of the elbow's primary and secondary stabilizers: the coronoid process (anterior buttress), the radial head (anterior and valgus buttress), and the lateral collateral ligament (LCL) complex (primary restraint to posterolateral rotatory instability).
Preoperative Planning and Patient Positioning
Optimal patient positioning is dictated by the anticipated surgical approach, the presence of concurrent injuries, and the surgeon's preference.
- Supine Position: Place the patient supine with the affected arm extended onto a radiolucent hand table. This position is ideal for a direct lateral approach to the elbow, providing excellent access to the radiocapitellar joint, LCL complex, and lateral coronoid.
- Lateral Decubitus Position: Alternatively, place the patient in the lateral decubitus position with the affected side up. The arm is draped free and rests over a sterile bolster.
Surgical Pearl: The lateral decubitus position is highly advantageous if a universal posterior skin incision is chosen. It allows for the elevation of full-thickness medial and lateral fasciocutaneous flaps, granting simultaneous access to the lateral structures, the medial collateral ligament (MCL), the ulnar nerve, and the posterior olecranon. This position is also preferred if the application of a hinged external fixator is anticipated.
🔪 Surgical Technique: Step-by-Step Reconstruction
The surgical sequence typically follows an "inside-out" or "deep-to-superficial" philosophy, beginning with the deepest structures (coronoid) and progressing outward (radial head, then LCL).
Phase 1: Exposure and Identification of Pathology
- Approach: Utilize either a direct lateral approach (Kocher or Kaplan interval) or a posterior midline incision with lateral flap elevation.
- Identify the "Bare Spot": Upon accessing the lateral compartment, identify the "bare spot" on the posterolateral aspect of the lateral epicondyle. This represents the avulsed origin of the LCL complex.
- Tissue Preservation: Work meticulously through the traumatic soft tissue disruption. Extend the surgical window proximally and distally only as required, preserving all intact capsuloligamentous structures.
- Tagging: Place heavy nonabsorbable tagging sutures into the detached LCL complex for later repair. If the common extensor origin is disrupted, tag it separately to facilitate an anatomical layered closure.
Phase 2: Coronoid Process Evaluation and Fixation
The coronoid process is the most critical anterior stabilizer of the ulnohumeral joint. Its restoration is paramount to preventing recurrent posterior subluxation.
- Inspection: Inspect the coronoid to determine the fracture pattern (Regan-Morrey or O'Driscoll classification) and severity.
- Exposure Enhancement: Visualization of the deep coronoid is often obscured by the fractured radial head. Because the radial head is irreparably damaged and requires excision in approximately 60% of terrible triad injuries, removing the radial head fragments early dramatically enhances the view of the anterior ulnohumeral joint.
- Fixation of Large Fragments (Type II or III): If a large basal or anteromedial facet fragment is present, reduce it anatomically. Fixation is typically achieved using one or two small-fragment (3.0-mm or 3.5-mm) lag screws directed posteroanteriorly from the dorsal surface of the ulna.
- Technique: Insert a guidewire from the dorsal ulna, visually confirming its exit point through the coronoid fracture bed. Reduce the fragment under direct vision and advance the wire, followed by definitive screw fixation.
- Plate Fixation: Larger, comminuted coronoid fragments often require specialized buttress plating to resist the sheer forces of the distal humerus.

FIGURE 57-68 Plate fixation of coronoid process utilizing a specialized anterior buttress plate.
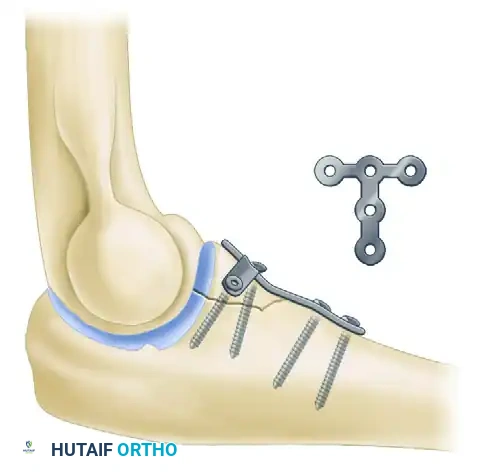
Fracture line demonstrating the critical need for anterior buttressing to prevent posterior ulnohumeral subluxation.
Surgical Warning: Application of a dedicated coronoid plate often necessitates a separate direct medial approach (e.g., over-the-top of the flexor-pronator mass or through the FCU split) to achieve orthogonal fixation. For comminuted fractures, prioritize fixing the largest articular fragment to restore the anterior buttress.
- Fixation of Small Fragments (Type I): Transverse tip fractures are generally too small for screw fixation. Repair these using a "lasso" suture technique. Pass heavy nonabsorbable sutures around the bony fragment and the attached anterior capsule. Pass the suture limbs through transosseous drill holes (created with an eyed Kirschner wire) exiting the dorsal ulna, and tie them securely over a bone bridge.
Phase 3: Radial Head Management
The radial head acts as a vital secondary stabilizer to valgus stress and longitudinal radioulnar translation.
- Osteosynthesis (ORIF): If the radial head fracture consists of one or two large, non-comminuted fragments, attempt anatomical reduction. Hold the reduction with small pointed reduction forceps and provisionally stabilize with K-wires. Utilize small-fragment headless compression screws (e.g., Herbert screws), ensuring they are countersunk below the articular cartilage to prevent radiocapitellar impingement.
- Arthroplasty (Replacement): If the fracture exhibits severe comminution (three or more fragments), central impaction, extensive cartilage loss, or an associated non-reconstructable radial neck fracture, stable anatomical reduction is impossible. In these cases, excise the radial head.
- Sizing: Insert trial components of a modular metallic radial head prosthesis.
- Assessment: Move the elbow through a full ROM. The prosthesis must restore radiocapitellar contact without "overstuffing" the joint. Overstuffing leads to capitellar wear, loss of flexion, and lateral elbow pain. Once the correct size is confirmed, impact the definitive stem and assemble the modular head.
Phase 4: Lateral Collateral Ligament (LCL) Repair
With the bony architecture restored, the lateral soft tissue envelope must be tensioned and repaired.
- Reattachment: Repair the previously tagged LCL complex to its anatomical footprint (the isometric "bare spot" on the lateral epicondyle).
- Fixation Method: Use heavy nonabsorbable sutures passed through transosseous drill holes in the lateral condyle, or utilize metallic/PEEK suture anchors. Ensure the elbow is held in 90 degrees of flexion and full pronation during knot tying to appropriately tension the ligament and close the posterolateral rotatory interval.
Phase 5: Assessment of Stability and Closure
- Dynamic Examination: Before closure, release the tourniquet (if used) and examine the elbow under fluoroscopy. Move the joint through an arc of flexion-extension from 20 to 130 degrees.
- Concentric Reduction: Confirm that the ulnohumeral and radiocapitellar joints remain concentrically reduced without any posterior or posterolateral subluxation.
- Managing Residual Instability: If residual instability is observed:
- Re-evaluate the quality of the coronoid fixation.
- Check the sizing of the radial head prosthesis (is it too small?).
- Assess the tension of the LCL repair.
- If all lateral and anterior structures are secure, the instability is likely driven by medial incompetence. Proceed to repair the disrupted medial structures (MCL and flexor-pronator mass) via a medial approach.
- If instability persists despite all repairs, apply a dynamic hinged external fixator to protect the reconstruction while allowing early motion.
- Closure: Close the fascial layers, subcutaneous tissue, and skin. Apply a well-padded posterior splint with the elbow in the most stable position—typically 90 degrees of flexion and full forearm pronation.
Postoperative Care and Rehabilitation
The delicate balance between preventing stiffness and protecting the surgical reconstruction dictates the postoperative protocol.
- Immobilization: The posterior splint is maintained for 1 to 10 days, depending strictly on the intraoperative stability achieved and the presence of polytrauma.
- Early Motion: In the vast majority of patients, ROM exercises are initiated on the first postoperative day.
- Dynamic Stabilization: Active and active-assisted exercises are highly encouraged. Muscle contraction of the flexor-pronator mass and the common extensor origin acts as a dynamic stabilizer to the elbow joint, compressing the articular surfaces.
- Positional Restrictions: Full forearm rotation (pronation and supination) is permitted, provided the elbow is flexed to 90 degrees. Patients must strictly avoid the terminal 30 degrees of extension (the most unstable position for posterolateral rotatory instability) for the first 4 weeks. Unrestricted shoulder and wrist exercises are encouraged immediately to prevent regional stiffness.
Complications of Terrible Triad Injuries
Complications following complex elbow fracture-dislocations are frequent and can severely compromise function. They include deep infection, radioulnar synostosis, severe arthrofibrosis, symptomatic hardware, and chronic residual instability.
- Post-Traumatic Arthrosis: Anatomical reduction of all intra-articular fractures is an absolute prerequisite to minimizing late-onset arthritic changes. Despite optimal care, some degree of extension loss (typically 10 to 15 degrees) is expected and should be discussed with the patient preoperatively.
- Heterotopic Ossification (HO): Ectopic calcification is exceedingly common, often manifesting as calcium deposition within the collateral ligaments and joint capsule. While mild calcification rarely requires intervention, severe heterotopic ossification can bridge the joint space, leading to complete bony ankylosis.
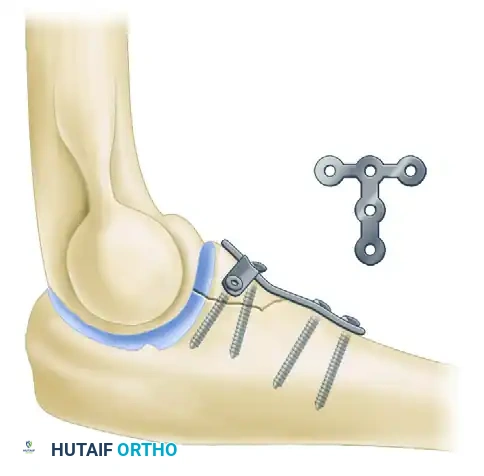
FIGURE 57-69 Extensive heterotopic ossification after a terrible triad fracture-dislocation and radial head excision, resulting in profound stiffness.
Clinical Pearl: HO is typically visible on radiographs 3 to 4 weeks post-injury. Its severity correlates directly with the magnitude of the initial trauma, the degree of soft tissue stripping, and the duration of postoperative immobilization. Prophylaxis (e.g., Indomethacin or localized radiation) should be considered in high-risk patients.
MANAGEMENT OF OLECRANON FRACTURES
Olecranon fractures represent a disruption of the extensor mechanism of the elbow. Because the olecranon is entirely intra-articular and subcutaneous, these injuries demand precise management to restore the articular congruity and the functional power of the triceps.
The overarching goal of treatment is the restoration of painless, functional motion. Displaced fractures invariably result in a loss of active elbow extension. Anatomical reduction and rigid internal fixation are vital not only for restoring triceps function but also for preventing post-traumatic ulnohumeral arthrosis. Furthermore, stable fixation is mandatory to permit the implementation of an early ROM program, which is the only reliable method to decrease the high incidence of post-traumatic arthrofibrosis.
Nonoperative Treatment
Nonoperative management is strictly reserved for a specific subset of injuries:
* Indications: Nondisplaced or minimally displaced fractures (less than 2 mm of step-off) where the patient demonstrates the ability to actively extend the elbow against gravity, proving the extensor mechanism is functionally intact.
* Protocol: The elbow is immobilized in a well-padded splint at 90 degrees of flexion for 3 to 4 weeks. This is followed by gentle passive motion, progressing systematically to active-assisted, and finally, active motion.
Operative Treatment Strategies
The vast majority of olecranon fractures are displaced due to the unopposed proximal pull of the triceps muscle, necessitating surgical intervention. Critical to the preoperative plan is the radiographic recognition of concurrent elbow injuries, such as radial head fractures or subtle ulnohumeral subluxations (e.g., transolecranon fracture-dislocations).
1. Tension Band Wiring (TBW)
The tension band wiring technique is the classic workhorse for specific olecranon fracture patterns.
- Biomechanics: The theoretical principle of TBW is to convert the tensile distraction forces acting on the dorsal cortex (generated by the triceps during flexion) into dynamic compressive forces at the articular surface. Note: While widely taught, recent in vivo biomechanical studies have struggled to definitively demonstrate this complete conversion to compression forces; nonetheless, it remains a highly effective stabilization method.
- Indications: TBW is highly effective for simple, transverse olecranon fractures without articular comminution.
- Contraindications: It is strictly contraindicated in fractures that are oblique, highly comminuted, or located distal to the center of rotation of the trochlear notch. In these patterns, TBW will lead to articular collapse, narrowing of the greater sigmoid notch, and subsequent joint subluxation.
2. Plate Osteosynthesis
For fractures not amenable to TBW, plate fixation is the gold standard.
- Indications: Comminuted fractures, oblique fracture lines, Monteggia-variant fracture-dislocations, and fractures extending distally into the ulnar diaphysis.
- Technique: A pre-contoured, anatomically designed locking plate is applied to the dorsal surface of the ulna. This acts as a neutralization or buttress plate, rigidly holding the articular fragments in anatomical alignment while resisting the deforming forces of the triceps.
3. Excision and Triceps Advancement
In rare scenarios, internal fixation may be impossible or ill-advised.
- Indications: Severe, non-reconstructable proximal articular comminution; extremely low-demand, elderly, or infirm patients; or as a salvage procedure following catastrophic failure of previous internal fixation.
- Technique: The proximal comminuted fragments are excised. The triceps tendon is then advanced and secured directly to the intact distal olecranon using heavy transosseous sutures or suture anchors.
- Biomechanical Consideration: Recent biomechanical data strongly suggest that reattaching the triceps to the posterior margin of the remaining olecranon articular surface, rather than the anterior margin, optimizes the lever arm and leads to significantly greater postoperative triceps strength.
Complications of Olecranon Fractures
- Symptomatic Hardware: Because the dorsal border of the ulna is subcutaneous, hardware prominence (especially the K-wires and figure-of-eight wire in TBW) is the most common complication, often requiring a secondary procedure for removal once union is achieved.
- Wound Breakdown: The thin soft tissue envelope is prone to dehiscence and superficial infection. Meticulous handling of the skin flaps and layered closure are essential.
- Nonunion: Distraction forces across the fracture site from premature active extension or inadequate fixation rigidity can contribute to delayed union or nonunion, necessitating revision osteosynthesis with bone grafting.
