Solve Sports Medicine Cases: Uncover Why the Correct Answer Is E

Key Takeaway
We review everything you need to understand about Solve Sports Medicine Cases: Uncover Why the Correct Answer Is E. Anterior knee pain in athletes often stems from conditions like Patellofemoral syndrome (runner's knee), Plica syndrome, or ACL tears. These conditions are diagnosed by symptoms such as overuse, instability, and specific pain locations. Treatments involve rest, strengthening vastus medialis, anti-inflammatories, and activity modification. For a holistic approach to patient care, the correct answer is e: comprehensive diagnostic and management strategies.
A 22-year-old female runner presents with a 3-month history of anterior knee pain, failing conservative management. She now complains of a "snapping" sensation medial to the patella. Based on the initial presentation and the subsequent development of focal medial symptoms, what is your primary clinical suspicion, and what specific physical exam maneuvers would you employ to confirm it?
Candidate: I suspect Patellofemoral Pain Syndrome (PFPS) that has evolved into a Medial Plica Syndrome. I would palpate for a tender, thickened band medially and try to reproduce the "snap" by flexing and extending the knee. I would also perform a standard knee exam to rule out internal derangement.
Candidates often focus solely on the knee joint or suggest an MRI immediately. They fail to mention the provocative nature of the snapping (the specific flexion arc of 30–60 degrees) and ignore the kinetic chain (hip/pelvic control) which is essential for a high-scoring answer.
Acknowledge the evolution from PFPS to secondary Medial Plica Syndrome due to chronic maltracking. Physical Exam: Perform targeted palpation of the medial femoral condyle. Demonstrate the 'Stutter Test' or active snapping by flexing the knee (30–60 degrees) while palpating the medial parapatellar area. Crucially, mention a comprehensive kinetic chain assessment: assess for dynamic valgus, Trendelenburg sign, and ITB tightness (Ober test) to explain why the plica is symptomatic (lateral patellar pull/femoral internal rotation).
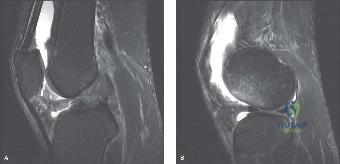
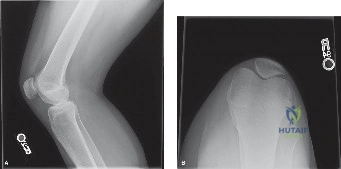
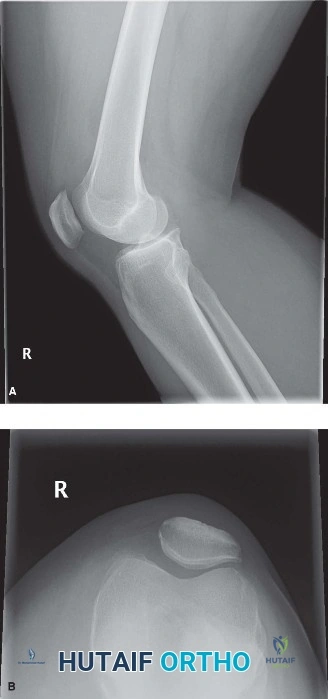
You have reviewed the patient's axial radiographs and MRI. The MRI shows a Type C medial plica and Grade II chondromalacia. The TT-TG distance is 14mm. Given this, discuss your surgical strategy and specifically address the role of lateral retinacular release.
Candidate: I would perform an arthroscopic excision of the plica. I would consider a lateral release if the patella is still tilting, but I know it's a bit controversial.
The "dangerous" answer is to suggest a prophylactic or routine lateral retinacular release. Examiners look for the candidate to actively distance themselves from this, citing the high risk of iatrogenic medial instability.
State clearly that the surgical goal is the resection of the symptomatic, fibrotic plica. Regarding the lateral retinaculum: explicitly condemn isolated lateral retinacular release for this pathology. Explain that if lateral tightness is present, lengthening is preferred over release to avoid medial subluxation. Emphasize that the TT-TG distance is normal (14mm), confirming this is a soft-tissue/kinetic chain issue, not a bony malalignment case requiring osteotomy.
Following successful arthroscopic plica excision, how do you structure the rehabilitation program to ensure this patient returns to competitive running without recurrence?
Candidate: I would start with range of motion exercises, then move to VMO strengthening. I'd tell her to gradually increase her running distance over 3 months.
A "knee-centric" rehab plan is a failure. Candidates who ignore the hip/core, or who do not mention specific criteria-based progression (e.g., VMO activation, dynamic valgus control), will score low.
Structure the answer in three phases: 1) Protection/Activation: Focus on early ROM and quad sets to prevent inhibition. 2) Kinetic Chain Optimization: This is the "Gold Standard" section—prioritize gluteus medius, maximus, and hip external rotator strengthening to correct the dynamic valgus. 3) Return to Sport: Criteria-based. Use high-cadence, midfoot strike running retraining. Prohibit hill training until she is pain-free on flat ground and demonstrates resolution of dynamic valgus on single-leg hop testing.
