Introduction to Neuromuscular Spine Deformity
The combination of hip dislocation, pelvic obliquity, and scoliosis represents a classic and highly debilitating triad in the wheelchair-bound patient with cerebral palsy (CP). These complex, interconnected deformities cause significant difficulties with pain, sitting balance, and overall independence. In the ambulatory child, progressive spinal deformity and coronal or sagittal imbalance can make standing erect difficult, if not entirely impossible. In the nonambulatory child, severe neuromuscular scoliosis leads to abnormal weight distribution, resulting in ischial or sacral skin pressure areas, decubitus ulcers, and, in advanced cases, life-threatening cardiopulmonary compromise.
The pathoanatomy of scoliosis in patients with cerebral palsy is fundamentally different from that of adolescent idiopathic scoliosis (AIS). While AIS typically presents with focal, compensatory S-shaped curves, neuromuscular curves in CP tend to be long, sweeping, thoracolumbar C-shaped curves. These are frequently accompanied by significant pelvic obliquity, which anchors the deformity and complicates seating and positioning.
Epidemiologically, the incidence of scoliosis in CP is directly proportional to the severity of neurologic and motor involvement. Scoliosis affects approximately 7% of ambulatory patients but surges to 35% in nonambulatory patients. When stratified by the topographic distribution of spasticity, approximately 50% to 75% of patients with spastic quadriplegia are affected, compared with fewer than 5% of those with hemiplegia. Madigan and Wallace demonstrated that up to 64% of institutionalized patients with CP develop scoliosis, underscoring the profound impact of severe neuromuscular impairment on spinal alignment.
Biomechanics and the Hip-Spine Controversy
The relationship between hip dislocation, pelvic obliquity, and scoliosis has been a subject of extensive orthopedic debate, particularly regarding the sequence of surgical intervention.
Drummond et al. historically posited that pelvic obliquity was the direct result of a combination of unilateral hip contracture and scoliosis. They recommended that the pelvic obliquity and spinal deformity be corrected before addressing the hip deformity, arguing that hip reconstruction in the presence of untreated pelvic obliquity would inevitably lead to the recurrence of the hip dislocation due to persistent asymmetric mechanical forces.
Conversely, Lonstein and Beck, in a landmark review of 500 children treated by the Cerebral Palsy Spine Service at Gillette Children’s Hospital, challenged this paradigm. They found absolutely no statistical correlation between the frequency of dislocated hips (whether bilateral or unilateral) and the presence or severity of pelvic obliquity. Furthermore, the frequency of hip dislocation on the same side as the elevated hemipelvis had no direct correlation with the degree of pelvic obliquity.
Clinical Pearl: The "Windswept" Hip Phenomenon
In patients presenting with "windswept" hips (one hip adducted and internally rotated, the contralateral hip abducted and externally rotated), Lonstein and Beck found no correlation between the direction of the windswept deformity and the direction of the pelvic obliquity.
The current consensus, derived from these findings, is that hip pathology is primarily the result of localized muscle imbalance around the hip joint itself (e.g., spastic adductors and flexors overpowering abductors and extensors). Meanwhile, pelvic obliquity and scoliosis are related to global muscle imbalance of the trunk and are largely independent of the position of the hips. Therefore, treatment algorithms should address the most functionally limiting deformity first, though many modern centers advocate for concurrent or closely staged management.
Sagittal Plane Deformities
Patients with cerebral palsy frequently exhibit profound sagittal plane abnormalities, which must be addressed during surgical planning.
Hyperkyphosis
Hyperkyphosis is the most common sagittal deformity, particularly prevalent in young children with weak spinal extensor muscles and poor head control. This forward-collapsing posture significantly interferes with sitting balance, eye contact, and communication. Initial management is non-operative, utilizing wheelchair modifications such as custom-molded seating, added chest supports, or reclining the seat back to utilize gravity for truncal extension. Soft body orthoses may also be employed, though they are poorly tolerated in patients with severe spasticity or gastroesophageal reflux.
Hyperlordosis
Hyperlordosis occurs less frequently and is typically a secondary, compensatory deformity. It is most often associated with severe hip flexion contractures or a rigid thoracic kyphosis. Treatment of the primary deformity (e.g., surgical release of hip flexors or correction of the thoracic spine) usually improves or completely corrects the hyperlordosis.
Clinical Evaluation and Radiographic Assessment
The evaluation of the CP patient with scoliosis requires a multidisciplinary approach, assessing not only the spine but also nutritional status, pulmonary function, seizure control, and bone density.
Radiographic evaluation must include full-length posteroanterior (PA) and lateral spine radiographs. For nonambulatory patients, these should be taken in the seated position to evaluate the effect of gravity on the curve and to accurately measure pelvic obliquity. Supine traction films or bending films are critical to assess the flexibility of the curve, which dictates the need for anterior release or aggressive posterior osteotomies.
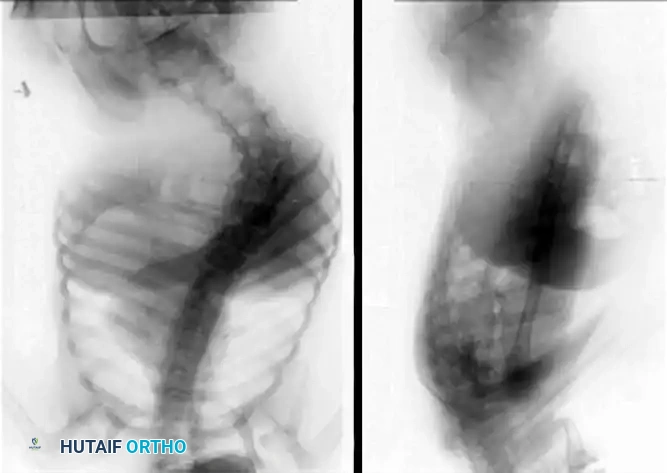
As demonstrated in the imaging above, severe thoracolumbar curves in spastic quadriplegia rapidly progress to structural pelvic obliquity, leading to asymmetric ischial seating pressures and a high risk of decubitus ulceration.
Indications for Surgical Intervention
Compared with curves in idiopathic scoliosis, neuromuscular curves in CP patients tend to occur at a younger age, are highly progressive, and almost universally require operative treatment. Curves exceeding 30 to 40 degrees in this population tend to progress relentlessly, even after skeletal maturity.
Orthotic management (e.g., TLSO) has been definitively shown to be ineffective in preventing the progression of neuromuscular scoliosis. Its use is strictly limited to temporarily improving sitting balance or delaying surgery in highly immature patients to allow for further thoracic and pulmonary development.
Operative treatment should be considered for patients in whom scoliosis or pelvic obliquity interferes with overall function, rather than being based solely on the absolute magnitude of the Cobb angle. As Rinsky stated, in all patients with neuromuscular scoliosis, the goals of treatment must be functionally oriented.
Primary Surgical Indications:
* Loss of sitting balance requiring the use of upper extremities for support.
* Progressive pelvic obliquity causing asymmetric seating and impending skin breakdown.
* Intractable back or rib-impingement pain.
* Documented curve progression >40-50 degrees in a growing child, or >50 degrees in a mature patient.
* Deteriorating pulmonary function directly attributable to thoracic deformity.
Surgical Approaches and Techniques
The overarching goals of surgery are to prevent further deformity, provide a rigidly well-balanced spine in both the coronal and sagittal planes, and correct any underlying pelvic obliquity to restore a level pelvis for sitting.
Posterior Spinal Fusion (PSF) to the Pelvis
For the vast majority of nonambulatory CP patients with pelvic obliquity, fusion must extend from the upper thoracic spine (typically T2 or T3 to prevent proximal junctional kyphosis) down to the pelvis. Stopping short of the pelvis in a patient with a sweeping neuromuscular curve and pelvic obliquity carries an unacceptably high risk of distal add-on deformity and progressive obliquity.
Surgical Warning: Pelvic Fixation
Failure to achieve rigid pelvic fixation in a nonambulatory CP patient with pelvic obliquity will result in construct failure, implant pullout, and recurrent deformity. Modern techniques mandate robust lumbo-pelvic anchoring.
Instrumentation Strategies
Historically, surgical stabilization consisted of posterior spinal instrumentation with segmental fixation using Luque wires and Galveston pelvic rods. While Wimmer et al. found no significant difference in curve correction or complication rates when comparing posterior wiring with hook constructs, modern spine surgery has largely transitioned to all-pedicle-screw constructs.
Pedicle screws offer superior three-column biomechanical purchase, allowing for powerful derotation, translation, and cantilever correction maneuvers. This rigid fixation significantly decreases the need for postoperative immobilization (casting or bracing) and reduces the pseudoarthrosis rate. For pelvic fixation, the traditional Galveston technique has been largely superseded by Iliac Screws or S2-Alar-Iliac (S2AI) screws, which provide exceptional pullout strength and are placed in line with the cranial pedicle screws, facilitating easier rod insertion.
Step-by-Step Surgical Technique: Posterior Spinal Fusion
- Positioning: The patient is placed prone on a Jackson spinal table with chest and hip pads. Care is taken to pad all bony prominences. The abdomen must hang free to reduce venous pressure and minimize intraoperative epidural bleeding.
- Exposure: A standard midline longitudinal incision is made. Subperiosteal dissection exposes the spinous processes, laminae, and transverse processes bilaterally from the upper thoracic spine to the sacrum.
- Facetectomies: Meticulous bilateral facetectomies are performed at every level to be fused. This provides posterior column release for deformity correction and creates a vascularized bed for the bone graft.
- Anchor Placement: Pedicle screws are inserted using anatomic landmarks, fluoroscopy, or robotic/navigation assistance. S2AI screws are placed bilaterally to anchor the construct into the pelvis.
- Correction Maneuvers: Pre-contoured rods (typically 5.5mm or 6.0mm Cobalt Chrome or Titanium) are seated. Correction is achieved through a combination of rod derotation, translation, and cantilever reduction. Pelvic obliquity is corrected by applying distraction on the concavity and compression on the convexity of the lumbosacral junction.
- Arthrodesis: The posterior elements are aggressively decorticated. Copious amounts of autograft (from local bone) and allograft are packed into the facet joints and along the decorticated transverse processes.
- Closure: Deep fascial layers are closed tightly over drains to prevent hematoma and reduce infection risk.
Adjunctive Lower Extremity Procedures in Spastic Deformity
While spinal alignment is the central pillar of truncal balance, the comprehensive management of the CP patient often requires concurrent or staged correction of severe distal spastic deformities. Spastic contractures of the foot and ankle can severely compromise wheelchair positioning, transfer ability, and standing balance.
When severe spastic varus or valgus deformities of the forefoot are present, soft tissue releases are indicated to provide a plantigrade, braceable foot. The following technique is frequently utilized for spastic medial column contractures.
🔪 Surgical Technique: Medial Release for Spastic Forefoot Deformity
- Incision and Exposure: Make a medial longitudinal incision over the first metatarsophalangeal (MTP) joint. Expose and identify the abductor hallucis muscle and its tendinous insertion.
- Resection: To prevent recurrent spastic tethering, resect a 2.5-cm long segment of the abductor hallucis muscle and tendon. Simple tenotomy is insufficient in severe spasticity.
- Capsular Release: If the medial capsule of the first MTP joint is contracted (contributing to hallux varus), perform a partial capsulectomy or capsular reefing depending on the specific vector of the deformity.
- Closure and Padding: Close the subcutaneous tissue and skin. Meticulously pad the medial border of the forefoot and great toe to prevent pressure necrosis.
- Immobilization: Apply a short leg cast, carefully molded with the foot in the corrected (abducted/plantigrade) position to maintain alignment during soft tissue healing.
Postoperative Protocols and Outcomes
Postoperative care for the CP patient undergoing major spinal fusion requires intensive care unit (ICU) monitoring. Extubation may be delayed depending on preoperative pulmonary function and intraoperative blood loss. Aggressive pulmonary toilet, nutritional support (often via a pre-existing gastrostomy tube), and early mobilization into a customized wheelchair are critical to preventing complications such as pneumonia and deep vein thrombosis.
Literature on Outcomes and Caregiver Satisfaction
The decision to proceed with major spinal surgery in a severely involved CP patient is complex, but literature strongly supports the intervention for quality of life.
Cassidy et al. conducted a care burden study comparing 37 patients with severe CP. Seventeen patients (mean curve 37 degrees) who underwent spinal fusion were compared with 20 patients (mean curve 76 degrees) who did not. Objectively, they found no significant differences in the need for pulmonary medication, presence of decubitus ulcers, or the absolute time required for daily care. However, subjectively, the vast majority of healthcare workers and caregivers believed that the patients who had undergone fusion were significantly more comfortable and easier to position.
These findings were corroborated and expanded upon by Tsirikos et al., who administered comprehensive questionnaires to 190 parents and 122 educators of children with CP who had undergone spinal fusion. Assessing various aspects of function, seating, and care after surgery, their study revealed overwhelming satisfaction: 96% of parents and 84% of caretakers stated they would recommend spinal surgery, citing profound improvements in the child's sitting balance, pain reduction, and overall quality of life.
