INTRODUCTION TO SNAPPING SYNDROMES
It is a common clinical presentation for a patient to report hearing or feeling a snapping, clicking, or popping sensation within or around their joints. In the vast majority of cases, the disability or pain is insufficient to justify surgical intervention. Most patients respond favorably to reassurance, physical therapy, and the avoidance of the specific biomechanical activities that provoke the snapping sensation.
However, when snapping syndromes become chronically painful or mechanically restrictive, they transition from a benign annoyance to a pathological entity requiring precise orthopedic evaluation. Snapping is generally categorized into extraarticular (tendon or fascial subluxation over a bony prominence) and intraarticular (loose bodies, labral tears, or chondral defects) etiologies. This comprehensive guide details the pathophysiology, clinical evaluation, and surgical management of snapping syndromes across the knee, hip, and shoulder.
SNAPPING KNEE SYNDROMES
Snapping symptoms are relatively rare in the knee compared to the hip or shoulder. When evaluating a snapping knee, the surgeon must first differentiate between true extraarticular snapping and intraarticular catching or locking. Intraarticular mechanical symptoms are typically caused by meniscal tears, loose bodies, patellofemoral maltracking, or advanced arthritic joint changes, which are managed via standard arthroscopic principles. True snapping of the knee, however, is almost exclusively extraarticular in nature.
Biceps Femoris Tendon Snapping
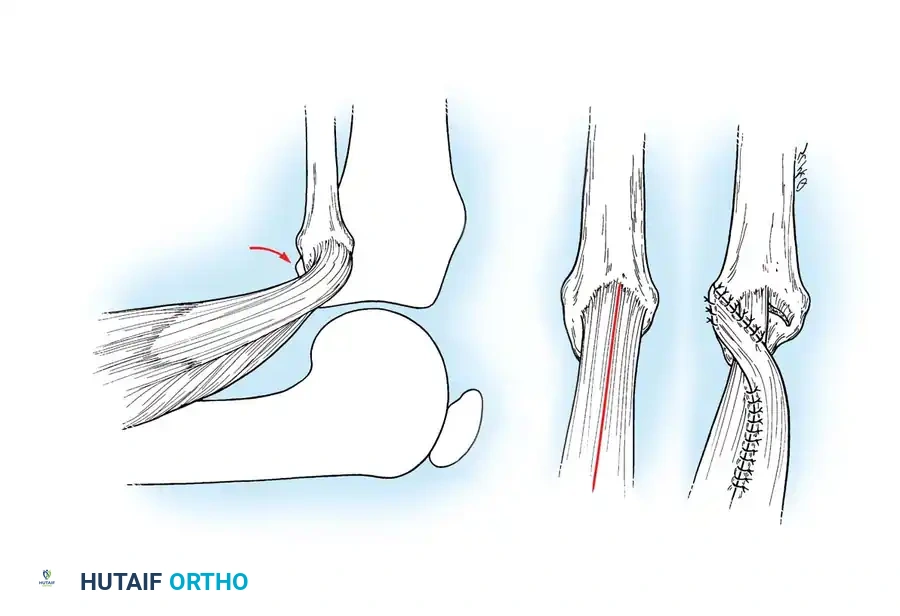
Extraarticular snapping on the lateral aspect of the knee is most frequently attributed to an abnormal anterior insertion of the biceps femoris tendon on the fibular head. During knee flexion and extension, the anomalous tendon slips over the prominent fibular head, creating a palpable and audible snap.
Clinical Pearl: Dynamic ultrasonography is highly effective in visualizing the biceps femoris tendon subluxating over the fibular head in real-time, confirming the diagnosis before surgical intervention.
If conservative management (activity modification, hamstring stretching, NSAIDs) fails, surgical realignment is indicated. Kristensen et al. and Lokiec et al. have demonstrated excellent outcomes with surgical reinsertion.
Surgical Technique: Biceps Femoris Rerouting
- Positioning: Supine with a bump under the ipsilateral hip to allow internal rotation of the leg.
- Incision: Make a longitudinal incision over the posterolateral aspect of the knee, centered over the fibular head.
- Dissection: Carefully identify and protect the common peroneal nerve, which courses posterior to the biceps femoris tendon and wraps around the fibular neck.
- Tendon Management: Identify the anomalous anterior insertion of the biceps femoris. Divide the anterior half of the tendon.
- Reattachment: Reroute and suture the divided tendon back over the posterolateral aspect of the fibular head, effectively covering the bony hump and preventing the anterior subluxation mechanism.
- Alternative: If the fibular head is excessively prominent, a partial resection of the fibular head (fibulectomy) with subsequent reattachment of the tendon and lateral collateral ligament (LCL) may be performed.
Popliteus and Hamstring Snapping
Popliteus Tendon Snapping: Cooper reported a rare snapping popliteus tendon syndrome. The snapping is typically palpable midway between the lateral epicondyle and the lateral joint line, becoming most pronounced when the knee is loaded with varus stress. While nonoperative rehabilitation is successful in most cases, refractory cases may require a popliteus tendon release or tenodesis of the popliteus tendon to the fibular collateral ligament.
Semitendinosus Snapping: Abnormal insertion of the semitendinosus tendon can cause it to snap over a bony prominence on the medial tibial condyle. Lyu and Wu recommend dividing the semitendinosus tendon at its insertion and transferring it to the semimembranosus tendon to alter its vector and eliminate the snapping.
Osteochondroma-Induced Snapping: A hamstring tendon sliding over a distal femoral osteochondroma can cause severe mechanical snapping. Excision of this benign lesion at its base is curative.
Management of Severe Extensor Mechanism Adhesions
In cases of severe trauma or prior surgery, massive scarring of the extensor mechanism can lead to painful snapping, catching, and profound loss of flexion. When standard arthroscopic lysis of adhesions fails, an open quadricepsplasty is required.
Surgical Technique: Quadricepsplasty for Extensor Contracture
- Preparation: Slowly flex the knee to 110 degrees under anesthesia to release any remaining intraarticular adhesions.
- Deep Dissection: Free the patella and the rectus femoris from the underlying femur, ensuring to leave a fibrous or periosteal covering on the anterior surface of the femur to prevent recurrent adhesions.
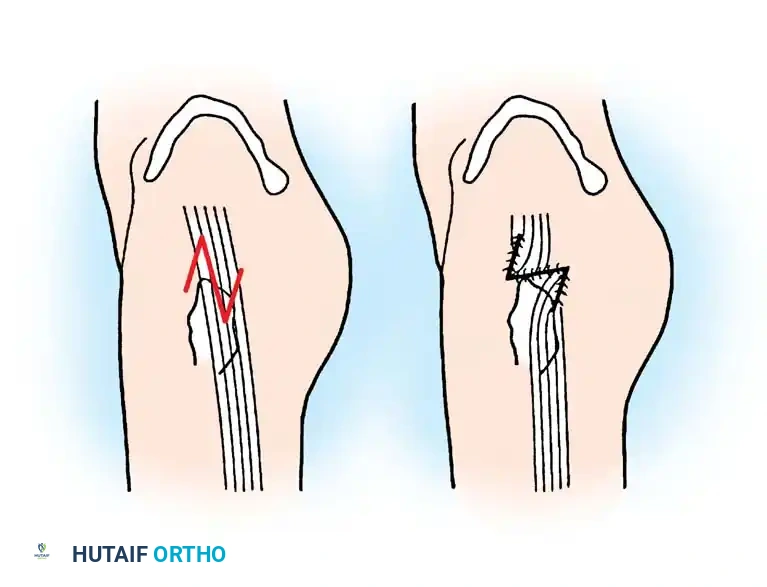
- Reconstruction: If the tendon of the rectus has been destroyed by the injury, create a neotendon by making longitudinal incisions through the scar tissue in the distal third of the thigh.
- Muscle Interposition: If the vastus medialis and lateralis are badly scarred, interpose subcutaneous tissue and fat between them and the rectus. If these muscles are relatively normal, suture them to the rectus as far distally as the distal third of the thigh.
- Tendon Lengthening: According to Nicoll, if flexion is still prevented after releasing adhesions, the rectus femoris itself is shortened. The tendon must be lengthened (e.g., via V-Y advancement), though this should be avoided if possible as it results in some loss of active extension.
- Patellar Management: In cases of gross damage to the deep surface of the patella, patellectomy may be required. The divided rectus femoris tendon is then sutured to the vastus medialis, and the vastus lateralis expansion is split and mobilized across to the vastus medialis.
- Closure: Remove the tourniquet and obtain complete hemostasis before closing the wound to prevent hematoma-induced arthrofibrosis.
Postoperative Protocol for Quadricepsplasty:
The extremity is immobilized in a splint at about 50 degrees less than the maximal flexion obtained during surgery for 2 to 3 days. A continuous passive motion (CPM) machine is then initiated. The patient remains hospitalized until 90 degrees of passive flexion is achieved. The knee is kept in full extension at night to prevent flexion contractures. Patients must be counseled to expect severe quadriceps weakness for many months, and skeletal immaturity may result in some loss of flexion as growth occurs.
SNAPPING HIP (COXA SALTANS)
The term snapping hip, or coxa saltans, designates an audible, palpable, or visible snap occurring during hip motion. It is classified into three distinct anatomical categories: External, Internal, and Intraarticular.
External Derangement (External Snapping Hip)
External snapping is the most common variant. It is caused by a tense fascial band—usually the thickened posterior border of the iliotibial (IT) band or the anterior border of the gluteus maximus muscle—catching and sliding over the superior margin of the greater trochanter as the hip is flexed, adducted, or internally rotated.
Fibrosis of the posterior fibers of the gluteus maximus (often arising from multiple intramuscular injections) can also cause severe snapping. While usually painless and managed with physical therapy and IT band stretching, painful, chronic cases require surgical lengthening.
Surgical Warning: Local anesthesia or regional block with light sedation is highly preferable to general anesthesia for external snapping hip surgery. Complete muscle relaxation under general anesthesia makes the tense band difficult to locate. Under local anesthesia, the patient can voluntarily snap the hip intraoperatively, allowing the surgeon to pinpoint the exact pathology by direct vision and palpation.
Surgical Technique: Z-Plasty of the Iliotibial Band (Brignall and Stainsby)
- Positioning: Lateral decubitus position.
- Incision: Make a longitudinal lateral incision beginning at the center of the greater trochanter, carrying it proximally for 10 to 12 cm.
- Fascial Incision: Identify the tight IT band. Make an 8-cm longitudinal incision in the fascia lata just anterior to the tight band. Ensure the incision is proximal enough so that the greater trochanter does not protrude through the defect if the suture line fails.
- Z-Plasty Flaps: Make a second incision at the proximal end of the first incision, directing it anteriorly and distally. Make a third incision at the distal end of the first incision, directing it posteriorly and proximally.
- Transposition: Dissect the flaps free from the underlying tissue. Transpose the flaps to lengthen the band.
- Closure: Close the transposed flaps with heavy absorbable sutures.
Postoperative Protocol: The patient rests in bed with the hip abducted until the wound heals sufficiently. Partial weight-bearing with crutches and a wide-based gait is initiated, progressing to full weight-bearing at 6 weeks.
Internal Derangement (Internal Snapping Hip)
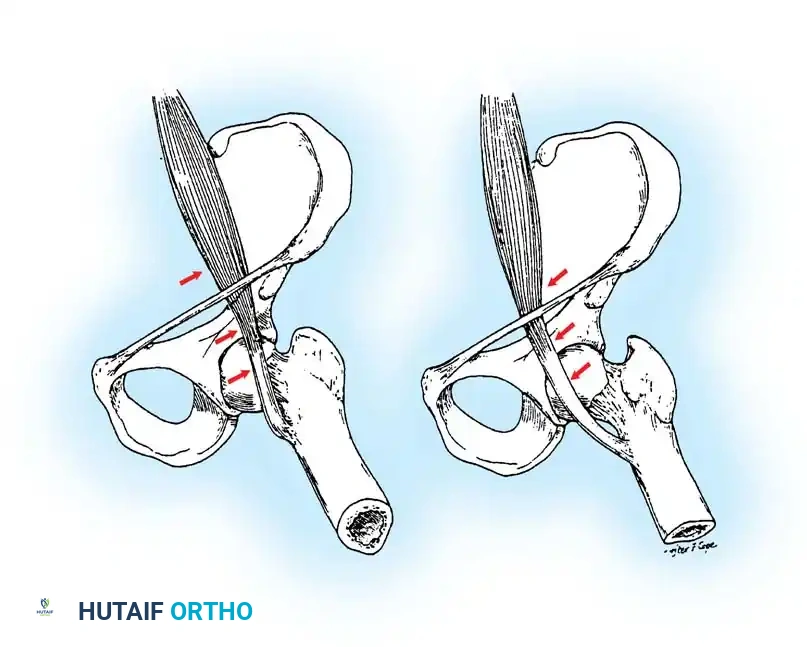
Internal snapping hip is caused by the iliopsoas tendon subluxating over the iliopectineal eminence or the femoral head. As demonstrated by Schaberg et al. and Jacobson and Allen, during hip flexion, the iliopsoas tendon shifts laterally in relation to the center of the femoral head. Upon hip extension, the tendon snaps medially across the femoral head or the pelvic brim.
Surgical Technique: Iliopsoas Tendon Lengthening
- Approach: Make a transverse inguinal incision just distal to the inguinal ligament, extending from the anterior superior iliac spine (ASIS) toward the pubis.
- Superficial Dissection: Identify and protect the lateral femoral cutaneous nerve. Retract the sartorius and rectus femoris muscles laterally.
- Deep Dissection: Develop the natural internervous plane between the rectus femoris (femoral nerve) and the adductor muscles (obturator nerve), exposing the iliopsoas muscle, its tendon, and the anterior bony pelvis.
- Release/Lengthening: Resect any bony prominences from the lesser trochanter. If a separate tendinous slip is present at the level of the iliopectineal eminence, resect it. Perform a Z-plasty lengthening or a fractional lengthening of the iliopsoas tendon at the level of the lesser trochanter.
Intraarticular Derangement of the Hip
Intraarticular snapping is characterized by a sharp clicking sensation perceptible to both the patient and the examining physician. Causes include synovial osteochondromatosis, loose bodies, labral tears, or habitual subluxation of the hip due to posterior acetabular dysplasia.
Historically managed via open arthrotomy (requiring surgical dislocation of the femoral head), the vast majority of intraarticular hip derangements are now evaluated and treated via Hip Arthroscopy. If an open procedure is mandated (e.g., massive osteochondromatosis or structural instability), a standard anterior (Smith-Petersen) or posterior (Kocher-Langenbeck) approach is utilized based on the location of the pathology.
SNAPPING SHOULDER SYNDROMES
Snapping shoulder syndrome encompasses a spectrum of intraarticular, extraarticular, and scapulothoracic pathologies. A meticulous clinical examination is paramount to isolate the anatomical source of the crepitus.
Intraarticular Snapping Shoulder
Intraarticular snapping is frequently secondary to glenohumeral instability, labral defects (Bankart lesions), SLAP tears, or loose bodies.
Clinical Pearl: The "Clunk" Test (Andrews and Gillogly)
Performed with the patient supine and the arm in full overhead abduction. The examiner places one hand posterior to the humeral head to apply anterior pressure, while the other hand provides rotation and axial loading at the humeral condyles. A palpable "clunk" or grinding indicates a labral tear or anterior instability.
Radiographic evaluation must include true anteroposterior (Grashey), axillary lateral, and supraspinatus outlet views. MRI or MR Arthrogram is the gold standard for diagnosing labral pathology, which is subsequently managed via arthroscopic debridement or stabilization.
Extraarticular Snapping Shoulder
Extraarticular snapping can arise from contracture of the deltoid muscle or entrapment of the lesser humeral tuberosity. Bristow reported a classic presentation where abduction of the shoulder produced a violent snap followed by severe pain. Intraoperatively, this is often revealed to be anomalous muscle fibers originating from the short head of the biceps passing over the lesser tuberosity during rotation. Surgical excision of the anomalous band resolves the mechanical block.
Snapping Scapula Syndrome (Scapulothoracic Crepitus)
Though not explicitly detailed in the raw extract, snapping scapula is a critical component of shoulder snapping syndromes. It is caused by the disruption of the smooth gliding motion between the anterior scapula and the posterior thoracic cage.
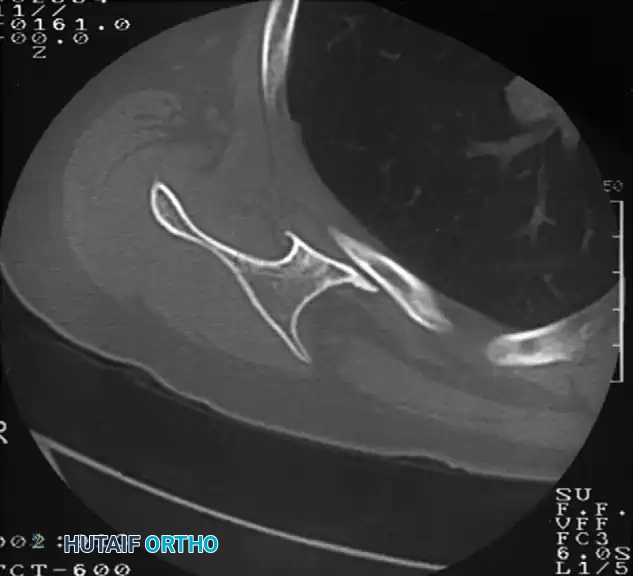
Pathologies include osteochondromas of the ventral scapula, Luschka's tubercle enlargement, or fibrotic bursitis (scapulothoracic bursitis). Advanced imaging, particularly CT scans with 3D reconstruction, is invaluable for identifying ventral scapular exostoses. Refractory cases are treated with arthroscopic or open partial scapulectomy (resection of the superomedial angle) and bursectomy, yielding high rates of symptomatic relief and restoration of normal shoulder kinematics.
CONCLUSION
The successful management of snapping syndromes relies on precise anatomical localization. While conservative therapy remains the first-line treatment, surgical interventions—ranging from fascial Z-plasties to tendon rerouting and arthroscopic debridement—provide reliable, definitive solutions for patients with chronic, debilitating mechanical symptoms. Strict adherence to postoperative rehabilitation protocols is essential to prevent recurrent adhesions and ensure the restoration of dynamic joint stability.
📚 Medical References
- Allen WC, Cope R: Coxa saltans: the snapping hip revisited, J Am Acad Orthop Surg 3:303, 1995.
- Altenberg AR: Acetabular labrum tears: cause of hip pain and degenerative arthritis, South Med J 70:174, 1977.
- Andrews JR, Gillogly S: Physical examination of the shoulder in throwing athletes. In Zarins B, Andrews JR, Carson WG Jr, eds: Injuries to the throwing arm, Philadelphia, 1985, Saunders. Bagchi K, Grelsamer RP: Partial fi bular head resection for bilateral snapping biceps femoris tendon, Orthopedics 26:1147, 2003.
- Brignall CG, Brown RM, Stainsby GD: Fibrosis of the gluteus maximus as a cause of snapping hip, J Bone Joint Surg 75A:909, 1993.
- Brignall CG, Stainsby GD: The snapping hip: treatment by Zplasty, J Bone Joint Surg 73B:253, 1991.
- Bristow WR: A case of snapping shoulder, J Bone Joint Surg 6:53, 1924.
- Cooper DE: Snapping popliteus tendon syndrome: a cause of mechanical knee popping in athletes, Am J Sports Med 27:671, 1999.
- Edelson JG: Variations in the anatomy of the scapula with reference to the snapping scapula, Clin Orthop Relat Res 322:111, 1996.
- Harper GD, McIlroy S, Bayley JI, et al: Arthroscopic partial resection of the scapula for snapping scapula: a new technique, J Shoulder Elbow Surg 8:53, 1999.
- Harper MC, Schaberg JE, Allen WC: Primary iliopsoas bursography in the diagnosis of disorders of the hip, Clin Orthop Relat Res 221:238, 1987.
- Jacobson TP, Allen WC: Surgical correction of the snapping iliopsoas tendon , Am J Sports Med 18:470, 1990.
- Kristensen G, Nielsen K, Blyme P: Snapping knee from biceps femoris tendon, Acta Orthop Scand 60:621, 1989.
- Kuhn JE, Plancher KD, Hawkins RJ: Symptomatic scapulothoracic crepitus and bursitis, J Am Acad Orthop Surg 6:267, 1998.
- Lokiec F, Velkes S, Schindler A, et al: The snapping biceps femoris syndrome, Clin Orthop Relat Res 283:205, 1992.
- Lyu SR, Wu JJ: Snapping syndrome caused by the semitendinosus tendon, J Bone Joint Surg 71A:303, 1989.
- Mozes G, Bickels J, Ovadia D, et al: The use of three-dimensional computed tomography in evaluating snapping scapula syndrome, Orthopedics 22:1029, 1999.
- Nicholson GP, Duckworth MA: Scapulothoracic bursectomy for snapping scapula syndrome, J Shoulder Elbow Surg 11:80, 2002.
- Pelsser V, Cardinal E, Hobden R, et al: Extraarticular snapping hip: sonographic fi ndings, Am J Roentgenol 176:67, 2001.
- Richards RR, McKee MD: Treatment of painful scapulothoracic crepitus by resection of the superomedial angle of the scapula: a report of three cases, Clin Orthop Relat Res 247:111, 1989.
- Schaberg JE, Harper MC, Allen WC: The snapping hip syndrome, Am J Sports Med 12:361, 1984.
- Sisto DJ, Jobe FW: The operative treatment of scapulothoracic bursitis in professional pitchers, Am J Sports Med 14:192, 1986.
- Spinner RJ, An KN, Kim K, et al: Medial or lateral dislocation (snapping) of a portion of the distal triceps: a biomechanical, anatomic explanation, J Shoulder Elbow Surg 10:561, 2001.
- Spinner RJ, Goldner RD: Snapping of the medial head of the triceps and recurrent dislocation of the ulnar nerve: anatomical and dynamic factors, J Bone Joint Surg 80A:239, 1998.
- Spinner RJ, Goldner RD, Fada RA, et al: Snapping of the triceps tendon over the lateral epicondyle, J Hand Surg 24A:381, 1999.
- Stuart PR, Epstein HP: Habitual
