Introduction & Epidemiology
Osteoarthritis (OA) of the shoulder joint is a debilitating condition characterized by progressive articular cartilage degeneration, subchondral bone remodeling, and osteophyte formation, leading to pain, stiffness, and functional impairment. While "shoulder osteoarthritis" is often colloquially used to refer to glenohumeral osteoarthritis (GHOA), it is crucial for the orthopedic surgeon to differentiate between the distinct pathological entities affecting the glenohumeral (GH) and acromioclavicular (AC) joints, as outlined in the seed content.
GHOA represents a spectrum of degenerative changes primarily affecting the articulation between the humeral head and the glenoid fossa of the scapula. The protective hyaline cartilage that normally cushions these bone ends gradually erodes, leading to bone-on-bone articulation. This process can be idiopathic (primary GHOA) or secondary to prior trauma (fractures, dislocations), inflammatory arthritides (rheumatoid arthritis, gout), avascular necrosis, rotator cuff arthropathy, infection, or developmental dysplasias.
Acromioclavicular joint osteoarthritis (ACOA), in contrast, involves degenerative changes at the articulation of the distal clavicle and the acromion. While often less functionally debilitating than GHOA, severe ACOA can contribute significantly to shoulder pain, particularly with overhead activities or cross-body adduction.
The prevalence of shoulder osteoarthritis increases with age, affecting millions globally. Radiographic evidence of GHOA can be found in up to 20% of the population over 65 years old, though only a subset will experience clinically significant symptoms requiring intervention. ACOA is even more common, with radiographic changes seen in a majority of individuals over 60 years. Risk factors include advanced age, genetic predisposition, obesity, repetitive overhead activities, prior shoulder trauma (e.g., AC joint separations, humeral head fractures, glenoid rim fractures), and inflammatory joint disease. Understanding the distinct anatomical and pathological nuances of each form of shoulder OA is paramount for accurate diagnosis, appropriate staging, and effective treatment planning.

Surgical Anatomy & Biomechanics
A profound understanding of shoulder anatomy and biomechanics is non-negotiable for the orthopedic surgeon managing shoulder osteoarthritis. The shoulder girdle is a complex system involving the glenohumeral, acromioclavicular, sternoclavicular, and scapulothoracic joints, each contributing to the remarkable range of motion and stability required for upper extremity function.
Osteology
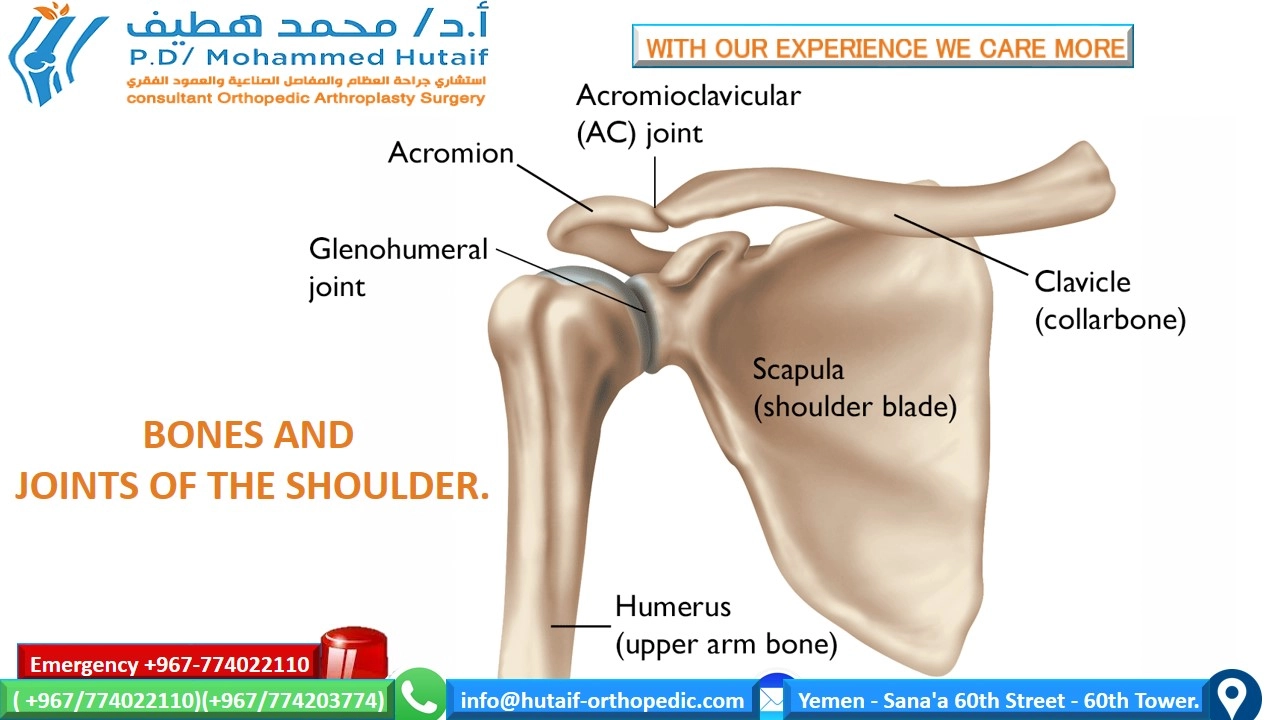
The three primary bones forming the shoulder joint are the:
*
Humerus:
The proximal humerus features the
humeral head
, which articulates with the glenoid fossa. Its spherical contour, typically 30-45 degrees of retroversion relative to the epicondylar axis, is critical for smooth articulation. The
anatomical neck
separates the head from the greater and lesser tuberosities, which serve as insertion points for the rotator cuff tendons. The
surgical neck
is distal to the tuberosities and is a common site for fractures. The
bicipital groove
(intertubercular sulcus) houses the long head of the biceps tendon.
*
Scapula:
A flat, triangular bone providing the
glenoid fossa
, a shallow, pear-shaped socket that articulates with the humeral head. The glenoid is relatively small, covering only about 25-30% of the humeral head surface, emphasizing the critical role of soft tissue stabilizers. The
glenoid labrum
, a fibrocartilaginous rim, deepens the socket by approximately 50% and serves as an attachment site for the glenohumeral ligaments. The
acromion
, a lateral projection from the scapular spine, forms the roof of the shoulder and articulates with the clavicle. The
coracoid process
, an anterior projection, serves as an attachment for multiple muscles and ligaments. The
scapular spine
divides the posterior scapula into supraspinous and infraspinous fossae.
*
Clavicle:
An S-shaped bone that provides the only bony attachment of the upper extremity to the axial skeleton. Its lateral end articulates with the acromion (AC joint), and its medial end articulates with the sternum (SC joint). The clavicle acts as a strut, facilitating optimal scapular positioning and rotation.
Articular Cartilage
Normal articular cartilage, particularly hyaline cartilage covering the humeral head and glenoid, is crucial for low-friction motion and load transmission. This highly specialized connective tissue is composed primarily of chondrocytes, collagen (predominantly type II), and proteoglycans. In GHOA, this cartilage undergoes progressive degradation, characterized by fibrillation, fissuring, softening, and eventually complete loss, exposing subchondral bone. This process alters the biomechanical properties of the joint, increasing friction and leading to symptomatic pain and stiffness.
Joint Capsule & Ligaments
The glenohumeral joint is inherently unstable due to the incongruity of its articular surfaces. Static stability is provided by the joint capsule and glenohumeral ligaments:
*
Capsule:
A fibrous sac surrounding the joint, reinforced by anterior ligaments and rotator cuff tendons. It is often contracted in OA, contributing to stiffness.
*
Glenohumeral Ligaments (SGHL, MGHL, IGHL complex):
These are thickenings of the anterior capsule. The
inferior glenohumeral ligament (IGHL) complex
, consisting of an anterior band, posterior band, and intervening axillary pouch, is the primary static stabilizer, particularly in abduction and external rotation. The
coracohumeral ligament (CHL)
, originating from the coracoid and blending with the capsule and rotator cuff, contributes to superior stability and restrains external rotation with the arm at the side.
The acromioclavicular (AC) joint is stabilized by the AC joint capsule and strong acromioclavicular ligaments (superior, inferior, anterior, posterior). Critical to AC joint stability are the coracoclavicular ligaments ( conoid and trapezoid ), which connect the clavicle to the coracoid process, preventing superior translation of the clavicle relative to the acromion.
Rotator Cuff
The rotator cuff consists of four muscles and their tendons:
supraspinatus, infraspinatus, teres minor
(SIT, inserting on the greater tuberosity), and
subscapularis
(inserting on the lesser tuberosity). These muscles provide dynamic stability to the glenohumeral joint by compressing the humeral head into the glenoid and facilitating rotation.
*
Supraspinatus:
Abduction, external rotation. Innervated by the suprascapular nerve.
*
Infraspinatus:
External rotation. Innervated by the suprascapular nerve.
*
Teres Minor:
External rotation. Innervated by the axillary nerve.
*
Subscapularis:
Internal rotation. Innervated by the upper and lower subscapular nerves.
Rotator cuff integrity is paramount for normal shoulder biomechanics. Degenerative tears, particularly in the context of GHOA, can lead to rotator cuff arthropathy (Cuff Tear Arthropathy, CTA), characterized by superior migration of the humeral head and further glenoid erosion, often necessitating reverse total shoulder arthroplasty.
Biceps Tendon
The long head of the biceps (LHB) tendon originates from the supraglenoid tubercle and superior labrum, courses through the bicipital groove, and inserts onto the radial tuberosity. While its role in shoulder stability is controversial, it contributes to glenohumeral depression and may be a source of pain in OA due to tendinopathy, subluxation, or partial tears.
Neurovascular Bundles
Knowledge of neurovascular structures is critical to prevent iatrogenic injury during surgical approaches:
*
Axillary Nerve:
Courses laterally around the surgical neck of the humerus, innervating the deltoid and teres minor. Vulnerable during inferior capsular release, humeral head resection, and posterior approaches.
*
Suprascapular Nerve:
Travels through the suprascapular notch (under the superior transverse scapular ligament) and then the spinoglenoid notch, innervating the supraspinatus and infraspinatus. Vulnerable during posterior approaches to the glenoid, extensive soft tissue dissection around the scapular spine, and glenoid screw placement in rTSA.
*
Musculocutaneous Nerve:
Pierces the coracobrachialis, innervating the biceps and coracobrachialis. Vulnerable during dissection around the coracoid process.
*
Brachial Plexus:
Located superior and posterior to the subclavian artery, vulnerable to traction injuries, especially in lateral decubitus positioning.
*
Axillary Artery and Vein:
Major vessels located deep to the pectoralis minor and medial to the humeral head.
Biomechanics of GHOA
The pathogenesis of GHOA involves a complex interplay of mechanical, biological, and inflammatory factors. Loss of articular cartilage leads to increased friction, altered joint loading, and ultimately subchondral bone remodeling, including sclerosis, cyst formation, and osteophyte development. Osteophytes, particularly inferiorly, can restrict range of motion.
Glenoid wear patterns are critical in GHOA:
*
Concentric wear (A1, A2 Walch):
Fairly uniform cartilage loss, often seen with an intact rotator cuff.
*
Posterior eccentric wear (B1, B2 Walch):
More pronounced posterior glenoid erosion, often associated with posterior subluxation of the humeral head, especially with rotator cuff dysfunction or increased humeral retroversion. A B2 glenoid involves biconcave wear.
*
Dysplastic glenoid (C Walch):
Glenoid retroversion exceeding 25 degrees, typically congenital, predisposing to early OA.
These wear patterns significantly influence surgical decision-making, particularly regarding glenoid component choice and implantation in arthroplasty. Rotator cuff deficiency exacerbates GHOA, leading to superior migration of the humeral head and characteristic rotator cuff arthropathy, shifting the indications towards reverse total shoulder arthroplasty.
Biomechanics of ACOA
ACOA involves degenerative changes in the synovial joint between the acromion and clavicle. Repetitive microtrauma, especially with overhead activities, can lead to cartilage wear, osteophyte formation, and reactive sclerosis. The degenerative process can narrow the joint space, leading to direct impingement, particularly during shoulder elevation and horizontal adduction. The loss of normal gliding mechanics contributes to pain and crepitus.
Indications & Contraindications
The management of shoulder osteoarthritis follows a stepwise approach, typically commencing with non-operative interventions. Surgical intervention is reserved for patients with persistent, debilitating symptoms refractory to conservative care.
Non-Operative Indications
Non-operative management is the initial approach for nearly all patients with symptomatic GHOA or ACOA, irrespective of radiographic severity, particularly for:
* Patients with mild to moderate pain and functional limitations.
* Individuals unwilling or medically unfit for surgery.
* Those with minimal radiographic changes.
* Patients with unrealistic expectations of surgical outcomes.
Components of Non-Operative Management:
*
Pharmacotherapy:
Non-steroidal anti-inflammatory drugs (NSAIDs) as first-line. Acetaminophen for pain relief. Adjunctive agents like tramadol may be considered.
*
Physical Therapy (PT):
Focus on maintaining range of motion, strengthening rotator cuff and scapular stabilizing muscles, postural correction, and activity modification. Goal is to optimize compensatory mechanisms and minimize stress on the arthritic joint.
*
Activity Modification:
Avoiding painful overhead activities, heavy lifting, or repetitive motions that exacerbate symptoms.
*
Intra-articular Injections:
*
Corticosteroid Injections:
Provide short-term pain relief and anti-inflammatory effects. Evidence suggests efficacy for 3-6 months, but repeated injections may be detrimental to cartilage over time.
*
Viscosupplementation (Hyaluronic Acid):
Attempts to restore the viscoelastic properties of synovial fluid. Evidence for GHOA is mixed, less robust than for knee OA.
*
Platelet-Rich Plasma (PRP) / Stem Cell Therapy:
Emerging treatments with limited, often conflicting, high-level evidence for GHOA. Currently considered experimental or for specific research protocols.
Operative Indications
Surgical intervention is indicated when patients experience severe pain, profound functional limitations (impacting activities of daily living, work, or sleep), and failure of a comprehensive course of non-operative management (typically 6-12 months).
Specific Indications for GHOA Surgery:
*
Total Shoulder Arthroplasty (TSA):
*
Primary indication:
Symptomatic, severe GHOA with an intact, functional rotator cuff and concentric glenoid wear (Walch A1/A2). Patients should have good bone quality to support glenoid component fixation.
*
Goal:
Restore pain-free range of motion and improve function by replacing both the humeral head and glenoid articular surfaces.
*
Reverse Total Shoulder Arthroplasty (rTSA):
*
Primary indication:
Symptomatic, severe GHOA in the context of a deficient or irreparable rotator cuff (rotator cuff arthropathy, CTA), significant eccentric glenoid erosion (Walch B2/C glenoids), or failed conventional TSA.
*
Goal:
Restore deltoid function and improve elevation in the absence of a functioning rotator cuff by altering the biomechanics to a medialized center of rotation. Also indicated for complex proximal humeral fractures in the elderly, and certain revision cases.
*
Hemiarthroplasty (HA):
*
Limited primary role for GHOA:
Rarely indicated as a primary procedure due to superior pain relief and functional outcomes of TSA. May be considered in younger, high-demand patients with severe GHOA and good glenoid cartilage, or in cases where glenoid replacement is contraindicated (e.g., severe glenoid bone loss, active infection, young patient with potential for early glenoid loosening).
*
Goal:
Primarily pain relief by resurfacing the humeral head.
*
Arthroscopic Debridement:
*
Limited role:
May be considered for early GHOA with specific mechanical symptoms (e.g., loose bodies, chondral flaps, impingement from osteophytes) or for patients who are not surgical candidates for arthroplasty due to medical comorbidities.
*
Goal:
Address mechanical symptoms and transiently improve pain, but generally does not alter the disease progression in advanced OA.
Specific Indications for ACOA Surgery:
*
Distal Clavicle Excision (DCE):
*
Primary indication:
Symptomatic, severe ACOA causing localized pain, crepitus, and tenderness at the AC joint, especially with cross-body adduction or overhead activities, refractory to non-operative management.
*
Goal:
Remove the degenerative articular surfaces and associated osteophytes to create a space between the distal clavicle and acromion, eliminating bone-on-bone impingement. Can be performed arthroscopically or open.
Contraindications
General Contraindications for Elective Shoulder Surgery:
*
Active Infection:
Absolute contraindication. Must be eradicated prior to arthroplasty.
*
Uncontrolled Medical Comorbidities:
Severe cardiac, pulmonary, or renal disease that significantly increases surgical and anesthetic risk.
*
Severe Neurologic Deficit:
Impairing deltoid or rotator cuff function to an extent that would compromise the outcome of the specific arthroplasty (e.g., deltoid paralysis for rTSA).
*
Unrealistic Patient Expectations:
Critical to manage expectations regarding pain relief, range of motion, and functional return.
*
Poor Patient Compliance:
Unwillingness to participate in post-operative rehabilitation.
*
Severe Psychiatric Illness:
Impairing ability to understand risks, consent, or comply with post-operative care.
Specific Contraindications/Considerations:
*
TSA:
Grossly deficient or irreparable rotator cuff (a relative contraindication, favoring rTSA), severe glenoid bone loss precluding stable glenoid component fixation.
*
rTSA:
Non-functional deltoid muscle or compromised axillary nerve function. Active infection of the shoulder. Insufficient glenoid bone stock for baseplate fixation (relative, may require bone grafting).
*
HA:
Young, active patient requiring definitive solution for pain or function (TSA generally preferred if glenoid allows).
Operative vs. Non-Operative Indications
| Condition/Severity | Non-Operative Indications | Operative Indications |
|---|---|---|
| GHOA - Early/Mild | NSAIDs, activity modification, physical therapy, corticosteroid injections | Arthroscopic debridement (for mechanical symptoms, loose bodies); Chondroplasty (limited role) |
| GHOA - Moderate | Persistent pain despite comprehensive non-operative measures, functional limitations | Hemiarthroplasty (young, high demand, good glenoid cartilage); Anatomic TSA (intact cuff, concentric wear) |
| GHOA - Severe (Intact Rotator Cuff, Concentric Wear - Walch A1/A2) | Failed prolonged (6-12 months) and optimized non-operative management, severe pain, significant functional impairment | Anatomic Total Shoulder Arthroplasty (TSA) |
| GHOA - Severe (Rotator Cuff Deficient/Cuff Tear Arthropathy, Eccentric Wear - Walch B2/C) | Failed prolonged (6-12 months) and optimized non-operative management, severe pain, significant functional impairment | Reverse Total Shoulder Arthroplasty (rTSA) |
| Failed TSA/HA | Mild symptoms, patient unwilling/unfit for revision | Revision TSA/rTSA, depending on etiology (infection, loosening, cuff failure) |
| ACOA - Symptomatic, Refractory to Non-Op | NSAIDs, activity modification, physical therapy, corticosteroid injections | Distal Clavicle Excision (DCE) (arthroscopic or open) |
| Absolute Contraindications for Elective Surgery | Active infection, uncontrolled medical comorbidities, severe psychiatric illness, unrealistic expectations, non-functional deltoid (for rTSA) | - |
Pre-Operative Planning & Patient Positioning
Thorough pre-operative planning is critical to optimize outcomes, anticipate challenges, and minimize complications in shoulder OA surgery.
Pre-Operative Assessment & Imaging
- Clinical Evaluation: A detailed history focusing on pain characteristics (location, intensity, aggravating/alleviating factors), functional limitations (ADLs, work, sport), previous treatments, and medical comorbidities. A comprehensive physical examination assesses range of motion (active and passive), strength (rotator cuff, deltoid), stability, tenderness, and neurovascular status.
-
Radiographic Imaging:
- Standard Radiographs: True AP (Grashey view), axillary lateral, and scapular Y views are essential. These allow assessment of joint space narrowing, osteophyte formation, subchondral sclerosis/cysts, humeral head migration, and glenoid morphology. For GHOA, the Walch classification (A1, A2, B1, B2, C) based on axillary views is critical for assessing glenoid version and wear patterns, guiding implant selection (anatomic vs. reverse). For ACOA, plain radiographs with specific views (Zanca view for AC joint) can demonstrate joint space narrowing, osteophytes, and distal clavicle osteolysis.
- Magnetic Resonance Imaging (MRI): Provides detailed soft tissue assessment. Essential for evaluating rotator cuff integrity (tendinopathy, partial/full-thickness tears), biceps tendon pathology, labral status, and articular cartilage quality. While not strictly necessary for advanced, bone-on-bone GHOA where the decision for arthroplasty is clear, it is invaluable for assessing potential concomitant pathology and informing surgical approach (e.g., significant cuff tear dictates rTSA).
- Computed Tomography (CT) Scan: The gold standard for assessing bone morphology, particularly glenoid bone loss, version, and retroversion. It is indispensable for pre-operative templating in arthroplasty, allowing for accurate measurement of glenoid and humeral dimensions, identification of bone defects, and virtual placement of implants to optimize sizing and positioning. 3D CT reconstructions can further enhance understanding of complex glenoid deformities.
Templating
Pre-operative templating using CT scans is paramount for all arthroplasty cases.
*
Humeral Component:
Determines appropriate stem size, head size, offset, and retroversion to optimize deltoid tension and joint stability.
*
Glenoid Component (TSA):
Essential for selecting the correct glenoid size, assessing the need for bone grafting, and planning optimal reaming to restore proper glenoid version and inclination.
*
Glenosphere/Baseplate (rTSA):
Critical for baseplate size and screw fixation length/angle, optimizing glenosphere lateralization, and minimizing impingement and scapular notching.
Patient Positioning
Proper patient positioning is essential for surgical exposure, patient safety, and surgeon ergonomics.
1.
Beach Chair Position:
*
Description:
The patient is semi-recumbent (30-70 degrees of trunk elevation) with the head supported in a neutral position (or slightly flexed/extended as needed for specific approaches, but avoiding excessive flexion or lateral bending to prevent brachial plexus strain). The back is padded, and the knees are slightly flexed. The operative arm is draped free to allow full range of motion.
*
Advantages:
Excellent exposure for both open (deltopectoral) and arthroscopic approaches, allowing for easy conversion from arthroscopy to open arthroplasty. Physiologically beneficial for the airway.
*
Disadvantages:
Risk of
cerebral hypoperfusion
(the "beach chair phenomenon"), leading to hypotension and potential for cerebral ischemia or stroke. Requires meticulous anesthetic management with continuous monitoring of blood pressure, ideally with an arterial line, and maintaining cerebral perfusion pressure. Care must be taken to prevent pressure neuropraxias (e.g., ulnar nerve at the elbow, peroneal nerve at the fibular head). The head and neck must be positioned to prevent excessive stretching of the brachial plexus.
2.
Lateral Decubitus Position:
*
Description:
The patient is positioned on their unaffected side with the operative shoulder superior. The operative arm is suspended in traction (often with weights) through a traction tower, allowing for joint distraction and access to the joint. Axillary roll placed to protect the brachial plexus and neurovascular bundle.
*
Advantages:
Provides excellent visualization for certain arthroscopic procedures, particularly for posterior structures. Less risk of hypotensive events compared to beach chair.
*
Disadvantages:
More challenging for open arthroplasty due to gravity-assisted humeral head subluxation and restricted freedom of arm manipulation. Can lead to brachial plexus traction injuries if excessive traction is applied or if the head/neck position is not neutral.
3.
Anesthesia:
*
General Anesthesia:
Standard for most shoulder arthroplasty procedures.
*
Regional Anesthesia (Interscalene Brachial Plexus Block):
Highly recommended as an adjunct to general anesthesia. Provides excellent post-operative analgesia, reducing opioid requirements and improving early rehabilitation efforts. Contraindications include respiratory compromise (phrenic nerve paralysis risk), severe coagulopathy, or local infection.
4.
Sterile Preparation & Draping:
* The entire shoulder and arm are prepped circumferentially from the base of the neck to the fingertips, allowing for full range of motion. Standard sterile drapes are applied. For arthroplasty, a specific impervious drape that isolates the arm from the body while allowing sterile manipulation is used.
Detailed Surgical Approach / Technique
The choice of surgical technique for shoulder osteoarthritis depends on the specific joint involved (GH vs. AC), the severity of the disease, the integrity of the rotator cuff, glenoid bone quality, and patient factors.
Glenohumeral Arthroplasty
The primary definitive surgical interventions for symptomatic GHOA are total shoulder arthroplasty (TSA), reverse total shoulder arthroplasty (rTSA), and less commonly, hemiarthroplasty (HA). All typically utilize a deltopectoral approach.
1. Deltopectoral Approach (Common to TSA, rTSA, HA)
- Patient Positioning: Beach chair position, operative arm draped free.
- Incision: A curvilinear incision typically 10-15 cm in length, beginning just lateral to the coracoid process and extending distally along the deltopectoral groove towards the mid-humerus.
-
Superficial Dissection:
- Skin and Subcutaneous Tissue: Incised carefully.
- Cephalic Vein: Located within the deltopectoral groove. Typically retracted laterally with the deltoid, or sometimes ligated if exposure is limited. Meticulous hemostasis around the vein is crucial.
-
Deep Dissection - Internervous Plane:
- The deltopectoral interval is identified between the deltoid muscle laterally (innervated by the axillary nerve, a branch of the posterior cord) and the pectoralis major muscle medially (innervated by the medial and lateral pectoral nerves). This is a true internervous plane.
- The deltoid is gently retracted laterally, and the pectoralis major medially.
- Careful dissection deep to the pectoralis major reveals the clavipectoral fascia, which is incised longitudinally. This exposes the coracobrachialis and short head of the biceps muscles laterally, and the axillary neurovascular bundle medially.
- The conjoined tendon (coracobrachialis and short head of biceps) is retracted medially. The musculocutaneous nerve typically enters the coracobrachialis approximately 5-8 cm distal to the coracoid tip and must be protected.
-
Subscapularis Management:
- The subscapularis muscle and tendon are exposed anterior to the joint capsule. The axillary nerve wraps posteriorly around the surgical neck, approximately 1-2 cm inferior to the inferior border of the subscapularis tendon; extreme caution is required during dissection and retraction inferiorly.
-
For TSA and HA, the subscapularis must be released to gain access to the joint. Common methods include:
- Tenotomy: A transverse cut through the subscapularis tendon, approximately 1 cm from its insertion on the lesser tuberosity. This is the most common method. Requires careful repair at the end of the procedure.
- Lesser Tuberosity Osteotomy: A small wafer of bone with the subscapularis insertion is osteotomized. Provides excellent healing potential, but adds complexity and risk of non-union.
- Peel-off/Release: The subscapularis is detached from the lesser tuberosity. Less common due to difficulty of repair.
- For rTSA, the subscapularis is often deficient or intentionally not repaired, as its function can be detrimental to the reverse prosthesis mechanics.
2. Anatomic Total Shoulder Arthroplasty (TSA)
- Indications: Severe GHOA with intact rotator cuff and concentric glenoid wear.
- Joint Exposure: After subscapularis release, the anterior capsule is opened (T-cut or inverted T-cut). The humeral head is dislocated anteriorly.
-
Humeral Preparation:
- Humeral Head Resection: A humeral head cutting guide is used to make a precise osteotomy at the anatomical neck, typically in 30-45 degrees of retroversion relative to the epicondylar axis, preserving bone for the prosthesis. The resected head is used for templating.
- Humeral Canal Preparation: Successive reamers and broaches prepare the humeral canal for the stem. The stem can be cemented or uncemented, depending on bone quality and surgeon preference.
- Humeral Component Implantation: The final stem and modular head are then implanted.
-
Glenoid Preparation:
- Cartilage Removal & Reaming: The remaining articular cartilage and underlying sclerotic bone are removed. Successive reamers are used to create a flat or slightly concave surface, correcting glenoid retroversion/anteversion to neutral or slight retroversion (0-10 degrees).
- Drilling & Peg/Keel Creation: Holes are drilled for the pegs or keel of the glenoid component.
- Glenoid Component Implantation: The polyethylene glenoid component is typically cemented into place. Meticulous cement technique is essential to achieve complete and durable fixation. Trial components are used to confirm fit and stability.
- Reduction & Stability Assessment: The humeral head and glenoid components are reduced. Range of motion is assessed, ensuring stability throughout the arc, with particular attention to subscapularis repair integrity.
- Closure: The capsule is repaired if possible. The subscapularis tendon is meticulously repaired to the lesser tuberosity using strong sutures (e.g., non-absorbable #2 suture). The deltopectoral interval is loosely closed, and subcutaneous tissues and skin are closed in layers.
3. Reverse Total Shoulder Arthroplasty (rTSA)
- Indications: Rotator cuff arthropathy, severe eccentric glenoid wear (Walch B2/C), failed TSA, complex proximal humeral fractures in the elderly.
- Joint Exposure: Similar deltopectoral approach. Subscapularis is often not repaired, as its absence can improve external rotation and the prosthesis often does not require it for stability. Humeral head dislocated.
-
Glenoid Preparation (Reverse):
- Reaming: The glenoid is reamed to a flat surface.
- Baseplate Fixation: A central post hole and peripheral screw holes are drilled. A glenoid baseplate is fixed to the scapular neck with locking screws. Stability and proper positioning (inferior inclination to reduce scapular notching) are critical.
- Glenosphere Implantation: The glenosphere (hemispherical metallic component) is attached to the baseplate. The size and lateralization of the glenosphere impact deltoid tension and range of motion.
-
Humeral Preparation (Reverse):
- Humeral Resection: Humeral head is resected, similar to TSA.
- Humeral Stem & Tray: The humeral canal is prepared for the stem. A modular humeral tray and polyethylene liner are then attached to the stem. The liner articulates with the glenosphere.
- Reduction & Stability Assessment: The components are reduced. Stability is assessed throughout range of motion, focusing on avoiding inferior dislocation (especially in adduction/internal rotation). Optimal deltoid tension is crucial.
- Closure: No subscapularis repair. Deltopectoral interval, subcutaneous tissues, and skin are closed.
4. Hemiarthroplasty (HA)
- Indications: Limited, as noted previously.
- Technique: Similar humeral preparation as TSA, but the glenoid articular surface is left untouched. The humeral head component (stem and modular head) is implanted. Pain relief is achieved by replacing the diseased humeral head articulating against the native glenoid cartilage.
Acromioclavicular Joint Excision (Distal Clavicle Excision - DCE)
- Indications: Symptomatic ACOA refractory to conservative management.
- Approach: Can be performed open or arthroscopically. Arthroscopic approach is increasingly preferred due to less soft tissue disruption and potentially faster recovery.
1. Arthroscopic Distal Clavicle Excision
- Patient Positioning: Beach chair position, arm draped free.
- Portals: Standard posterior portal (e.g., 2 cm inferior and 1 cm medial to the posterolateral corner of the acromion) and anterolateral portal (lateral to the coracoid process, for visualization and instrument insertion). Additional superior portals may be used.
-
Procedure:
- Visualization: The subacromial space is entered and bursectomy performed to clearly visualize the undersurface of the acromion and the AC joint.
- Resection: A motorized burr is used to resect the distal 6-10 mm of the clavicle, including any osteophytes. Care is taken to ensure that the superior, inferior, anterior, and posterior aspects of the distal clavicle are adequately resected to prevent residual impingement. The goal is to create a gap between the clavicle and acromion.
- Confirmation: The shoulder is taken through a full range of motion, including cross-body adduction, to ensure adequate decompression and no residual impingement.
- Closure: Portal sites are closed with simple sutures.
2. Open Distal Clavicle Excision
- Incision: A small transverse or longitudinal incision over the AC joint.
-
Procedure:
- The AC joint capsule and surrounding ligaments are incised.
- The distal clavicle is then resected using an osteotome or saw.
- The wound is closed in layers.
Complications & Management
Despite meticulous surgical technique, complications can occur with both glenohumeral arthroplasty and distal clavicle excision. Prompt recognition and appropriate management are crucial for salvage and optimizing patient outcomes.
General Surgical Complications
These apply to all surgical procedures and include:
*
Infection:
Superficial wound infection or deep periprosthetic joint infection (PJI).
*
Bleeding/Hematoma:
Can lead to increased pain, swelling, and risk of infection.
*
Neurovascular Injury:
Direct trauma or traction injury to nerves (axillary, suprascapular, musculocutaneous) or vessels (axillary artery/vein, circumflex humeral arteries).
*
Anesthetic Complications:
Related to general or regional anesthesia (e.g., pneumothorax from interscalene block, hypotension in beach chair position).
Specific GHOA Arthroplasty Complications
| Complication | Incidence (approx.) | Management / Salvage Strategy |
|---|---|---|
| Infection (Deep PJI) | 1-2% |
Early (<3-4 weeks):
Debridement, irrigation, retention of components, IV antibiotics.
Late: Two-stage revision (explantation, spacer, IV antibiotics, then reimplantation), or explantation without reimplantation. |
| Aseptic Glenoid Loosening | 5-15% (at 10 years for cemented) | Symptomatic: Revision to new TSA/rTSA (if rotator cuff compromised), bone grafting for defects. Uncemented glenoids may have higher early loosening risk. |
| Rotator Cuff Tear (Post-TSA) | 2-10% |
Acute, reparable:
Surgical repair.
Chronic, irreparable: Debridement, conversion to rTSA. |
| Periprosthetic Fracture | 1-5% |
Intraoperative:
Stem revision (longer/larger), cerclage wires, plates.
Postoperative: ORIF, revision with longer stem, allograft. |
| Stiffness/Arthrofibrosis | 5-15% | Intensive physical therapy, manipulation under anesthesia (MUA), arthroscopic capsular release. Prevention includes early mobilization. |
| Instability/Dislocation (TSA) | <1% | Closed reduction, open reduction, revision for component malposition. |
| Instability/Dislocation (rTSA) | 2-5% |
Acute:
Closed reduction (often requires general anesthesia).
Recurrent: Revision for component malposition (glenosphere lateralization, humeral offset, version), soft tissue balancing. |
| Axillary Nerve Injury | 1-2% | Observation (most are neuropraxias), EMG for prognosis, rarely exploration if no recovery. |
| Suprascapular Nerve Injury | <1% | Observation, EMG, rarely exploration. |
| Scapular Notching (rTSA) | Up to 60% (radiographic) |
Asymptomatic:
Observe.
Symptomatic/Progressive loosening: Revision with inferiorly angled glenoid, larger glenosphere, lateralization. |
| Heterotopic Ossification (HO) | 10-20% (radiographic) |
Asymptomatic:
Observe.
Symptomatic (stiffness): Physical therapy, radiation, NSAIDs (prophylaxis); surgical excision (after maturation). |
| Hardware Failure | <1% | Revision surgery for component breakage (e.g., glenoid screws, stem). |
Specific ACOA DCE Complications
| Complication | Incidence (approx.) | Management / Salvage Strategy |
|---|---|---|
| Persistent Pain / Inadequate Resection | 5-10% | Revision surgery for additional resection, steroid injection, PT. |
| AC Joint Instability (Iatrogenic) | <1% | Observation; rarely stabilization if symptomatic (e.g., excessive resection of coracoclavicular ligaments). |
| Neuropraxia (Supraclavicular Nerve) | <1% | Observation, symptom management. |
| Heterotopic Ossification | <5% | Observation; if symptomatic, physical therapy or excision. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgical procedure itself for optimizing functional outcomes after shoulder osteoarthritis surgery. Protocols are typically structured into phases, with progression based on healing, pain, and functional milestones. Individualized adjustments are frequently necessary.
General Principles
- Protection: Safeguarding surgical repairs (e.g., subscapularis, rotator cuff) and ensuring implant stability.
- Pain Management: Crucial for allowing participation in therapy. Multimodal analgesia including regional blocks, NSAIDs, and acetaminophen.
- Gradual Progression: Avoiding overstressing healing tissues while encouraging motion and strengthening.
- Patient Education: Ensuring patient understanding of restrictions, goals, and exercise techniques.
Phase I: Protection and Passive Motion (0-6 weeks post-surgery)
-
Goals:
- Control pain and swelling.
- Protect surgical repair/components.
- Initiate gentle passive range of motion (PROM) to prevent stiffness.
- Maintain mobility of elbow, wrist, and hand.
-
Immobilization:
- Glenohumeral Arthroplasty (TSA/HA): Typically a sling for 4-6 weeks, often with an abduction pillow for comfort and to reduce tension on the subscapularis repair.
- Reverse TSA (rTSA): Sling with abduction pillow for 4-6 weeks to prevent inferior dislocation and provide comfort.
- Distal Clavicle Excision (DCE): Sling for comfort for 1-2 weeks.
-
Exercises:
-
PROM:
Initiated by a therapist, typically within protected ranges.
- TSA/HA: Pendulum exercises, passive flexion (up to 90-120 degrees depending on subscapularis repair tension), passive external rotation (0-30 degrees initially, avoiding stress on subscapularis), passive internal rotation.
- rTSA: Pendulum exercises, passive flexion and abduction to tolerance. Strict avoidance of simultaneous adduction and internal rotation, which can lead to dislocation.
- Active Range of Motion (AROM): Elbow, wrist, and hand exercises (e.g., grip strengthening).
- Scapular Mobility: Gentle scapular glides.
-
PROM:
Initiated by a therapist, typically within protected ranges.
-
Restrictions:
- TSA/HA: No active shoulder elevation, external rotation, or lifting. No weight-bearing through the arm.
- rTSA: No lifting, pushing, or pulling. Strict dislocation precautions.
- DCE: No heavy lifting or overhead activities.
Phase II: Controlled Active Motion and Early Strengthening (6-12 weeks post-surgery)
-
Goals:
- Gradually restore active range of motion (AROM).
- Initiate gentle isometric strengthening.
- Improve scapular kinematics.
- Progression: Discontinue sling as tolerated.
-
Exercises:
- AROM: Gradually progress from PROM to active-assisted range of motion (AAROM) and then AROM exercises (flexion, abduction, rotation) as pain and healing allow.
- Isometric Strengthening: Submaximal isometric exercises for rotator cuff and deltoid, performed in multiple positions.
- Scapular Stabilization: Exercises to strengthen rhomboids, trapezius, and serratus anterior.
-
Restrictions:
- Avoid heavy lifting or carrying.
- No sudden, uncontrolled movements.
- Continue to respect subscapularis repair if applicable (TSA).
Phase III: Progressive Strengthening and Functional Return (12+ weeks post-surgery)
-
Goals:
- Maximize strength, endurance, and power.
- Restore full functional range of motion (within limits of the prosthesis and patient).
- Return to sport-specific or work-related activities.
- Progression: Resistance progressively increased.
-
Exercises:
- Progressive Resistive Exercises (PREs): Using bands, light weights, and bodyweight for rotator cuff, deltoid, and periscapular muscles.
- Eccentric Training: Gradual introduction of eccentric loading exercises.
- Proprioceptive Training: Balance and coordination exercises.
- Functional Activities: Tailored exercises to simulate work or sport demands.
-
Return to Activity:
- Low-impact activities: (e.g., swimming, cycling) typically allowed earlier.
- High-impact activities or overhead sports: Gradual return, often not before 6-12 months, and may be restricted based on prosthesis type and patient factors.
- Long-Term Considerations: Continued home exercise program is crucial. Regular follow-up with the surgeon to monitor implant status and overall joint health.
Specific Considerations for rTSA Rehabilitation
- Emphasis on deltoid strengthening and activation to compensate for the lack of rotator cuff function.
- Continued strict adherence to dislocation precautions (avoiding adduction, internal rotation, and extension past body in early phases) throughout rehabilitation and potentially long-term.
- Acceptance of potentially different biomechanics and motion patterns compared to anatomic TSA.
Summary of Key Literature / Guidelines
The body of literature guiding the management of shoulder osteoarthritis is extensive and continually evolving. Key principles and recommendations are often consolidated by major orthopedic societies.
GHOA Management
- Non-Operative Efficacy: Level I and II evidence supports the initial use of NSAIDs, physical therapy, and activity modification. Intra-articular corticosteroid injections provide short-term pain relief (3-6 months) but lack long-term disease-modifying effects. Viscosupplementation and PRP have less consistent evidence for GHOA compared to knee OA.
-
Total Shoulder Arthroplasty (TSA):
- Gold Standard: For symptomatic, end-stage GHOA with an intact rotator cuff and concentric glenoid wear. Numerous studies (Level I and II) demonstrate superior pain relief, functional outcomes, and patient satisfaction compared to hemiarthroplasty for primary GHOA.
- Long-Term Outcomes: Meta-analyses and large cohort studies report excellent 10-year implant survival rates (90-95%) and good to excellent clinical outcomes in appropriately selected patients. Glenoid loosening remains the most common mode of failure for anatomic TSAs.
- Glenoid Component: Cemented all-polyethylene glenoids remain the standard. Uncemented metal-backed glenoids have largely fallen out of favor due to higher rates of aseptic loosening and shorter survival. Newer hybrid glenoids (trabecular metal with polyethylene liner) are under investigation.
-
Reverse Total Shoulder Arthroplasty (rTSA):
- Paradigm Shift: Revolutionized the treatment of rotator cuff arthropathy (CTA) and GHOA with deficient rotator cuffs. Strong Level I and II evidence supports its efficacy in these populations, providing significant pain relief and improved active elevation where traditional TSA would fail.
- Indications: Consensus guidelines from the AAOS and ASES define key indications, including CTA, failed TSA with cuff deficiency, complex proximal humeral fractures in the elderly, and severe glenoid bone loss/eccentric wear (Walch B2/C glenoids).
- Outcomes: While highly effective, rTSA has specific complications such as scapular notching (radiographic incidence up to 60%, clinical significance variable), instability/dislocation (2-5%), and axillary nerve injury. Implant survival rates are generally very good at 5-10 years.
- Glenosphere Placement: Critical for optimizing outcomes and minimizing complications. Inferior tilt and lateralization of the glenosphere are advocated to reduce scapular notching and improve deltoid tension.
-
Hemiarthroplasty (HA):
- Limited Role: Primarily considered for specific scenarios such as young, active patients with severe GHOA and good glenoid cartilage, or in cases of active infection where glenoid component implantation is deferred. Outcomes are generally inferior to TSA for primary GHOA in terms of pain relief and functional improvement due to persistent glenoid pain.
-
Arthroscopic Debridement:
- Limited Efficacy: Consensus is that arthroscopic debridement, chondroplasty, and osteophyte resection have a limited and generally short-lived role for advanced GHOA. It may provide temporary relief for mechanical symptoms (loose bodies, impingement) in early OA or for non-surgical candidates, but does not alter the disease progression.
ACOA Management
- Non-Operative Management: Similar to GHOA, initial treatment involves rest, NSAIDs, physical therapy, and corticosteroid injections, with generally good results for mild to moderate symptoms.
-
Distal Clavicle Excision (DCE):
- Effective Intervention: For symptomatic ACOA refractory to non-operative treatment. Both open and arthroscopic techniques yield good to excellent pain relief and functional outcomes.
- Arthroscopic vs. Open: Multiple studies and meta-analyses suggest comparable clinical outcomes between arthroscopic and open DCE, with arthroscopic techniques potentially offering advantages in terms of smaller incision, less soft tissue disruption, and faster initial recovery. A resection of 6-10 mm of the distal clavicle is generally recommended. Complications are rare but include persistent pain and iatrogenic instability.
Guidelines and Consensus Statements
- The American Academy of Orthopaedic Surgeons (AAOS) and the American Shoulder and Elbow Surgeons (ASES) regularly publish clinical practice guidelines and position statements that synthesize the evidence and provide recommendations for the diagnosis and management of shoulder OA.
- The European Society for Surgery of the Shoulder and Elbow (SECEC/ESSSE) also provides valuable contributions to consensus on surgical techniques and rehabilitation protocols.
- Key literature often emphasizes the importance of patient selection, meticulous surgical technique, and adherence to structured rehabilitation protocols as determinants of successful outcomes for both GHOA and ACOA. Surgeon experience and adequate training are also consistently highlighted as critical factors.
