Patient Presentation & History
A 28-year-old male, a professional rugby player, presented to our clinic with recurrent right shoulder instability. His initial injury occurred approximately 18 months prior during a rugby tackle, resulting in a traumatic anterior glenohumeral dislocation. This was reduced in the emergency department, followed by a period of sling immobilization for three weeks and supervised physiotherapy. Despite adherence to the rehabilitation protocol, he experienced three further episodes of anterior dislocation over the subsequent 12 months, all during sporting activities involving abduction and external rotation. The most recent episode, three weeks prior to presentation, spontaneously reduced but left him with persistent apprehension and an inability to return to sport.
He reports significant pain with overhead activities and a constant fear of re-dislocation. He denies any paresthesia, weakness, or neurovascular symptoms. There is no personal or family history of generalized ligamentous laxity or connective tissue disorders. His past medical history is unremarkable, and he takes no regular medications. He is a non-smoker and consumes alcohol socially. His primary goal is to return to elite-level rugby.
Clinical Examination
Upon inspection, the right shoulder demonstrated no obvious deformity, swelling, or ecchymosis. There was no visible muscle atrophy of the deltoid or rotator cuff musculature. Previous surgical scars were absent.
Palpation revealed mild tenderness over the anterior aspect of the glenohumeral joint and the coracoid process. There was no warmth or effusion.
Active range of motion (ROM) was significantly limited by apprehension, particularly with abduction >90 degrees and external rotation >60 degrees. Passive ROM was full, but apprehension was elicited at the end-range of abduction and external rotation. Internal rotation was full and pain-free.
Specific stability tests were performed:
*
Apprehension Test:
Strongly positive at 90 degrees of abduction and maximal external rotation, eliciting significant apprehension and a guarding response.
*
Relocation Test (Fowler's sign):
Positive, with the patient's apprehension resolving upon posterior pressure applied to the humeral head.
*
Load and Shift Test:
Demonstrated increased anterior translation (grade II) compared to the contralateral shoulder, with a palpable clunk upon reduction. Posterior and inferior translation were symmetrical and within normal limits (grade I).
*
Sulcus Sign:
Negative, indicating no significant inferior laxity.
*
Jobe's Relocation Test (for posterior instability):
Negative.
*
O'Brien's Test and Speed's Test:
Negative, ruling out significant superior labral or biceps pathology.
*
AC Joint Compression Test:
Negative.
Neurovascular examination was intact. Distal pulses (radial, ulnar) were palpable and symmetrical. Sensation in the axillary, musculocutaneous, radial, ulnar, and median nerve distributions was normal. Motor strength was 5/5 in all upper extremity muscle groups tested, including deltoid (axillary nerve), biceps (musculocutaneous nerve), and triceps (radial nerve), although apprehension limited full effort with external rotation.
Imaging & Diagnostics
Initial plain radiographs obtained in the emergency department at the time of the first dislocation confirmed an anterior glenohumeral dislocation. Post-reduction films showed concentric reduction.
For the current presentation, a new series of standard shoulder radiographs was obtained, including:
*
True Anteroposterior (Grashey view):
Demonstrated an intact glenoid contour but raised suspicion for a bony defect on the anterior-inferior aspect.
*
Axillary View (Velpeau or West Point):
Crucial for evaluating the anterior glenoid rim and posterior humeral head. This view confirmed a bony Bankart lesion and revealed a moderate Hill-Sachs lesion on the posterior-superior aspect of the humeral head. The Hill-Sachs lesion appeared engaged.
*
Stryker Notch View:
Provided an optimal tangential view of the Hill-Sachs lesion, further characterizing its depth and extent.
*
Scapular Y View:
Confirmed concentric reduction and ruled out any gross scapular pathology.
To accurately quantify the bone defects and plan surgical intervention, a
Computed Tomography (CT) scan
of the right shoulder with 3D reconstruction was performed. This is considered the gold standard for assessing bony lesions in shoulder instability.

Figure 1: Representative axial CT scan image demonstrating a significant anterior-inferior glenoid bone defect.
The CT scan revealed:
* A
bony Bankart lesion
involving the anterior-inferior glenoid, with a quantified bone loss of approximately 22% of the glenoid articular surface (measured using the "Circle method" on axial views, comparing the involved glenoid to the contralateral healthy glenoid or a reconstructed "perfect circle").
* A
Hill-Sachs lesion
on the posterior-superior humeral head, measuring 25mm in length, 12mm in width, and 6mm in depth. Based on dynamic assessment on 3D CT and clinical correlation, this lesion was deemed to be "off-track" during dynamic external rotation and abduction, indicating engagement with the anterior glenoid rim.
A
Magnetic Resonance Arthrogram (MRA)
was also obtained to fully assess the soft tissue pathology and rule out other concomitant injuries. The MRA confirmed:
* An avulsion of the anterior-inferior labrum and capsule from the glenoid rim (Bankart lesion), consistent with the bony Bankart seen on CT.
* Capsular laxity, particularly anteriorly.
* No significant rotator cuff tear or biceps pathology.
* No HAGL (Humeral Avulsion of the Glenohumeral Ligaments) lesion.
* Intact superior labrum.
These imaging findings, particularly the quantified glenoid bone loss and the engaging Hill-Sachs lesion, were critical in guiding the surgical decision-making process.
Differential Diagnosis
The patient's presentation with recurrent anterior glenohumeral instability and confirmed bony pathology points strongly towards traumatic recurrent anterior instability. However, it is essential to consider other conditions that can present with similar symptoms or contribute to shoulder pathology.
| Condition | Key Features (History, Examination, Imaging) | Differentiating Factors |
|---|---|---|
| Traumatic Recurrent Anterior Glenohumeral Instability (Index Case) | History of definite traumatic primary dislocation, recurrent episodes, usually with specific arm position (abduction/ER). Positive apprehension/relocation tests. Imaging (X-ray, CT, MRI) demonstrating Bankart lesion (bony or soft tissue), Hill-Sachs lesion, glenoid bone loss. | Clear history of trauma and discrete dislocation events. Specific apprehension in abduction/ER. Imaging confirms anterior-inferior labral/capsular pathology, often with bony defects. Unidirectional instability. |
| Multidirectional Instability (MDI) | Often atraumatic onset, or minor trauma. History of generalized ligamentous laxity (Beighton score >4/9). Symptoms of 'looseness' or 'giving way' in multiple directions (anterior, posterior, inferior). Positive sulcus sign, generalized hyperlaxity on exam. Imaging may show capsular redundancy, minimal bony lesions. | Typically atraumatic or low-energy onset. Bi- or multi-directional apprehension. Positive sulcus sign. Evidence of generalized ligamentous laxity. Imaging may show subtle or no bony pathology but often significant capsular volume/laxity. |
| Rotator Cuff Tear (especially partial/subscapularis) | History of trauma (especially in older patients >40), or insidious onset. Pain with specific movements (lifting, overhead). Weakness, particularly with internal or external rotation. Positive Impingement signs (Neer, Hawkins). Imaging (MRI/MRA) shows tendon tear. | Pain is often the predominant symptom, not apprehension of dislocation. Weakness is key. Instability tests (apprehension/relocation) typically negative unless a massive cuff tear causes pseudo-paralysis. Imaging directly visualizes tendon pathology. |
| Superior Labrum Anterior Posterior (SLAP) Tear | History of overhead activities, throwing athletes, or fall onto an outstretched arm. Deep, aching pain, popping/clicking, 'dead arm' sensation. Positive O'Brien's, Speed's, and Compression-Rotation tests. Imaging (MRA) confirms superior labral pathology. | Instability tests are often negative. Pain is usually localized superiorly. Mechanism often involves compression or traction forces (e.g., FOOSH, throwing). Instability is not the primary complaint, although some SLAP tears can contribute to subtle instability. |
| Acromioclavicular (AC) Joint Osteoarthritis/Separation | Localized pain over the AC joint, especially with cross-body adduction or overhead lifting. Tenderness directly over the AC joint. Palpable step-off or deformity with AC separation. Imaging (X-ray) shows AC joint space narrowing, osteophytes, or displacement. | Pain is typically localized to the AC joint, not the glenohumeral joint. Instability tests are negative. X-rays are diagnostic for AC joint pathology. Absence of apprehension to dislocation. |
Surgical Decision Making & Classification
Given the patient's age (28 years), high-demand athletic profession (rugby), multiple recurrent anterior dislocations, significant glenoid bone loss (22%), and an engaging Hill-Sachs lesion, a non-operative approach was deemed highly unlikely to achieve a successful return to sport or prevent further instability episodes. The consensus in the literature indicates that glenoid bone loss exceeding 20-25% significantly increases the failure rate of isolated soft tissue Bankart repair.
The
Shoulder Instability Severity Index Score (ISIS Score)
was calculated:
* Age <20: No (0 points)
* Competitive Contact Sport: Yes (2 points)
* Hyperlaxity (Sulcus sign or ER >85° with arm at side): No (0 points)
* L-shaped or Inverted Pear Glenoid (on AP X-ray): Yes (bony Bankart/glenoid erosion) (2 points)
* Hill-Sachs lesion (visible on X-ray): Yes (2 points)
Total ISIS Score = 6 points. An ISIS score of >3 indicates a significantly higher risk of failure for arthroscopic Bankart repair alone, strongly suggesting the need for a bony procedure.
Based on these findings, an arthroscopic Bankart repair combined with a Remplissage procedure was initially considered. However, the glenoid bone loss of 22% is borderline for this approach, and the "off-track" Hill-Sachs lesion, while addressable by Remplissage, combined with the professional contact sport demands, prompted consideration for a more robust bony reconstruction.
The
Latarjet procedure
was ultimately selected as the optimal surgical intervention. The rationale was based on its triple-effect mechanism:
1.
Bone block effect:
Restores anterior-inferior glenoid bone stock, effectively converting the "inverted pear" glenoid back to a "normal pear."
2.
Sling effect:
The conjoined tendon (coracobrachialis and short head of biceps) acts as a dynamic restraint when the arm is abducted and externally rotated.
3.
Capsulolabral repair:
Direct repair of the capsule to the transferred coracoid block enhances stability.
This procedure provides a more robust solution for patients with significant bone loss and high-risk activity levels, offering a lower recurrence rate compared to isolated soft tissue repairs or even arthroscopic Bankart with Remplissage in this specific demographic.
Surgical Technique / Intervention
The patient was positioned in the beach chair position under general anesthesia with a regional interscalene block. The operative arm was prepped and draped free.
- Incision: A standard deltopectoral incision, approximately 5-6 cm in length, was made from the coracoid process distally.
- Exposure: The interval between the deltoid and pectoralis major was developed. The cephalic vein was identified and retracted laterally. The clavipectoral fascia was opened. The coracoid process was identified, and its anterior surface was cleared of soft tissue. The musculocutaneous nerve was identified entering the conjoined tendon, approximately 5 cm distal to the coracoid tip, and protected.
- Coracoid Osteotomy: Using an oscillating saw, the coracoid process was osteotomized at its base, distal to the attachment of the coracoclavicular ligaments. Care was taken to maintain the integrity of the conjoined tendon insertion. Two 3.2mm drill holes were pre-drilled in the coracoid block, approximately 10mm and 20mm from its tip.
- Subscapularis Split: The subscapularis muscle was identified. A longitudinal split was performed between the upper two-thirds and lower one-third of the subscapularis, extending down to the capsule. The anterior capsule was then incised to expose the glenohumeral joint.
- Glenoid Preparation: The anterior-inferior glenoid rim was exposed. The residual anterior labrum and any remnants of the anterior-inferior capsule were debrided to expose the bony defect. The glenoid neck was decorticated to promote bone healing.
- Coracoid Transfer and Fixation: The coracoid block, with the attached conjoined tendon, was transferred to the anterior-inferior glenoid defect. The inferior aspect of the coracoid block was carefully oriented flush with the native glenoid surface. The pre-drilled holes in the coracoid were aligned with pilot holes drilled into the glenoid neck. Two 3.75mm bicortical screws (e.g., cannulated partially threaded screws) were then used to secure the coracoid block firmly to the glenoid neck. Compression was achieved across the bone block to promote union.
- Capsule Repair: The remaining anterior capsule was repaired and tensioned over the transferred coracoid block to the native glenoid, creating the "sling effect" and reinforcing the anterior soft tissues.
- Subscapularis Repair: The subscapularis split was meticulously repaired.
-
Wound Closure:
The deltopectoral interval was closed, followed by subcutaneous and skin closure.
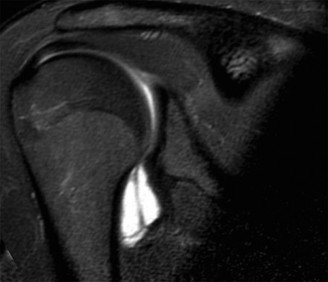
Figure 2: Intraoperative view showing the transferred coracoid bone block secured to the anterior-inferior glenoid rim with two screws during a Latarjet procedure.
Post-operatively, radiographs were obtained to confirm satisfactory positioning and fixation of the coracoid graft.
Post-Operative Protocol & Rehabilitation
The rehabilitation protocol following a Latarjet procedure focuses on protecting the surgical repair and ensuring bony integration of the coracoid block, while progressively restoring motion and strength.
Phase I: Immediate Post-operative (Weeks 0-4)
*
Immobilization:
Arm in a sling for 3-4 weeks for comfort and protection. Sling can be removed for hygiene and exercises.
*
Goals:
Pain control, protect surgical repair, promote early healing.
*
Exercises:
* Pendulum exercises: Gentle, pain-free.
* Elbow, wrist, and hand active range of motion (ROM).
* Scapular sets: Gentle isometric contractions.
* No active shoulder flexion or abduction.
* No external rotation beyond neutral.
* No internal rotation against resistance.
*
Precautions:
No active glenohumeral motion. Avoid lifting, pushing, pulling with the affected arm. Avoid sleeping on the affected side.
Phase II: Early Motion and Progressive Loading (Weeks 4-8)
*
Goals:
Restore passive ROM, initiate active-assisted ROM (AAROM), maintain joint integrity.
*
Exercises:
* Continue pendulum exercises.
* Supine passive ROM (with assistance from therapist or contralateral arm): Gradual increase in flexion, abduction (to 90-120 degrees), and external rotation (to 30-45 degrees, depending on surgeon preference).
* Active-assisted ROM for flexion and abduction using a pulley system or stick.
* Initiate isometric strengthening for rotator cuff (submaximal, pain-free).
* Scapular stabilization exercises.
*
Precautions:
No forced external rotation. Avoid lifting more than 1-2 kg. No forceful internal rotation.
Phase III: Strengthening (Weeks 8-16)
*
Goals:
Restore full active ROM, increase strength and endurance, improve neuromuscular control.
*
Exercises:
* Progress from AAROM to active ROM.
* Initiate resistance band exercises for internal and external rotation, abduction, flexion.
* Light weight training for deltoid and rotator cuff.
* Eccentric strengthening.
* Core and trunk stabilization.
* Proprioceptive training (e.g., closed kinetic chain exercises, perturbation training).
*
Precautions:
Avoid heavy lifting. Gradual progression of resistance. Ensure proper form to prevent compensation.
Phase IV: Advanced Strengthening and Return to Activity (Weeks 16-24+)
*
Goals:
Maximize strength, power, and endurance. Prepare for sport-specific activities.
*
Exercises:
* Advanced resistance training, plyometrics (e.g., medicine ball throws).
* Sport-specific drills (e.g., throwing mechanics, tackling simulations for rugby).
* Agility and proprioceptive drills.
* Gradual return to non-contact sports, then contact sports.
*
Return to Sport Criteria:
* Full, pain-free ROM.
* Strength symmetrical to the contralateral limb (at least 90%).
* No apprehension with sport-specific movements.
* Satisfactory functional testing (e.g., isokinetic testing, throwing velocity).
* Typically, return to full contact sport is allowed no earlier than 6 months post-operatively, often closer to 9 months, after radiological confirmation of bone graft union.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
- Comprehensive History is Key: Always ascertain the mechanism of injury, number of dislocations, and patient's activity level and expectations. TUBS (Traumatic, Unidirectional, Bankart, Surgery indicated) vs. AMBRI (Atraumatic, Multidirectional, Bilateral, Rehabilitation indicated, Inferior capsular shift if surgery needed) is a foundational concept.
- Quantify Bone Loss: For recurrent anterior instability, plain radiographs are insufficient. A dedicated CT scan with 3D reconstruction is essential to accurately quantify glenoid bone loss and characterize the Hill-Sachs lesion. The "Circle method" for glenoid bone loss calculation (often >20-25% as a threshold for bony reconstruction) and the "Glenoid Track" concept for Hill-Sachs engagement are critical for surgical planning.
- Recognize the "High-Risk" Patient: Young, male, contact/overhead athlete with recurrent dislocations, significant glenoid bone loss, or an engaging Hill-Sachs lesion, and a high ISIS score (>3), is at high risk for failure with arthroscopic soft tissue repair alone.
- Latarjet's Triple Effect: Understand the biomechanical advantages: bone block for glenoid restoration, conjoined tendon sling effect, and capsular repair. This provides superior stability in high-risk cases.
- Coracoid Positioning and Fixation: The coracoid graft must be positioned flush with the articular surface of the glenoid and medial to the equator to avoid impingement, while providing maximal bone stock. Bicortical screw fixation provides optimal stability and compression for bone healing.
- Neurovascular Awareness: Always be cognizant of the musculocutaneous nerve during coracoid dissection and osteotomy, and the axillary nerve during capsular management. Prophylactic identification and protection are paramount.
- Tailored Rehabilitation: A structured, progressive rehabilitation program is vital for successful outcomes. Protection of the repair in early phases, followed by gradual restoration of motion and strength, and finally sport-specific training. Emphasize delayed return to contact sports until complete healing and strength restoration.
Pitfalls:
- Underestimation of Bone Loss: Failure to obtain adequate imaging (CT scan) or misinterpreting plain radiographs can lead to underestimation of glenoid bone loss, resulting in an inadequate soft tissue repair and high recurrence rates.
- Ignoring the Engaging Hill-Sachs: An "off-track" Hill-Sachs lesion, if not addressed (e.g., by Remplissage or Latarjet, which effectively converts an off-track to an on-track lesion), can continue to engage and contribute to instability.
- Inadequate Glenoid Preparation: Insufficient decortication of the glenoid neck or incomplete removal of the soft tissue remnants from the defect can impair bone graft healing.
- Improper Coracoid Graft Placement: Placing the coracoid graft too lateral can cause cam impingement and restrict external rotation, while placing it too medial may not adequately restore the glenoid defect. Too proud or too recessed can also lead to issues.
- Premature Return to Activity: Allowing high-risk patients to return to contact sports too early, before full graft incorporation and strength recovery, significantly increases the risk of re-injury. Minimum 6 months is standard, with 9-12 months often recommended for contact athletes after a Latarjet.
- Iatrogenic Nerve Injury: The musculocutaneous nerve is at risk during coracoid osteotomy and transfer, and the axillary nerve is vulnerable during glenoid exposure and capsular repair. Meticulous dissection and nerve protection are non-negotiable.
- Missed Concomitant Pathology: Failure to identify and address other shoulder pathologies such as SLAP tears, rotator cuff tears, or generalized capsular laxity can compromise the overall outcome. An MRA is crucial for comprehensive soft tissue assessment.
