
Posttraumatic Elbow Arthritis: Best Management for Young Adults
Introduction & Epidemiology
Posttraumatic elbow arthritis (PTEA) represents a challenging clinical entity, particularly in young adult patients. It is defined by the progressive degeneration of the articular cartilage and associated joint structures following a prior traumatic injury to the elbow. Common antecedent injuries include intra-articular fractures (e.g., capitellum, trochlea, radial head, coronoid, olecranon), complex elbow dislocations, fracture-dislocations (e.g., terrible triad injuries), and severe soft tissue trauma. The incidence of PTEA is difficult to precisely quantify but is a recognized long-term sequela in a significant percentage of patients sustaining severe elbow trauma, ranging from 10% to over 50% in some series, depending on the initial injury severity and follow-up duration.
For young adults, PTEA carries unique implications. This demographic typically has higher functional demands, expects a longer lifespan, and is less tolerant of pain, stiffness, or functional limitations that impact their work, recreational activities, and quality of life. The management strategy must therefore prioritize joint preservation where feasible, optimize long-term outcomes, and carefully consider the longevity and potential need for revision of any implanted prostheses. The natural history of untreated PTEA in this population typically involves progressive pain, loss of range of motion (ROM), crepitus, mechanical symptoms, and ultimately, significant functional disability. Early and accurate diagnosis, coupled with a tailored management approach, is paramount to mitigating these long-term consequences.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate surgical anatomy and biomechanics of the elbow joint is foundational to the effective management of PTEA. The elbow is a complex trochogingylmoid joint, comprising three articulations within a single capsule: the ulnohumeral, radiohumeral, and proximal radioulnar joints.
Bony Anatomy
- Humerus: The distal humerus features the trochlea medially (articulating with the ulna) and the capitellum laterally (articulating with the radial head). The olecranon and coronoid fossae accommodate the respective ulnar processes during flexion and extension. The medial and lateral epicondyles serve as origins for collateral ligaments and forearm musculature.
- Ulna: The proximal ulna forms the olecranon posteriorly and the coronoid process anteriorly, creating the trochlear notch which articulates with the humeral trochlea. The radial notch on the lateral aspect of the coronoid accommodates the radial head.
- Radius: The radial head is cylindrical, articulating with the capitellum and the radial notch of the ulna, allowing pronation and supination.
Ligamentous Stabilizers
The elbow's stability is primarily conferred by its osseous congruity and robust ligamentous complex.
*
Medial Collateral Ligament (MCL) Complex:
Composed of the anterior bundle (primary valgus stabilizer), posterior bundle, and transverse ligament. It is crucial for posteromedial stability.
*
Lateral Collateral Ligament (LCL) Complex:
Composed of the radial collateral ligament, lateral ulnar collateral ligament (LUCL - critical for posterolateral rotatory stability), and annular ligament (stabilizing the radial head).
Musculature
Muscles surrounding the elbow play roles in motion, stability, and provide internervous planes for surgical access.
*
Anterior Compartment:
Brachialis (flexion), biceps brachii (flexion, supination).
*
Posterior Compartment:
Triceps brachii (extension).
*
Medial Epicondyle Group:
Forearm flexors and pronators.
*
Lateral Epicondyle Group:
Forearm extensors and supinators.
Neurovascular Structures
Key neurovascular structures traverse the elbow, necessitating meticulous identification and protection during surgery.
*
Ulnar Nerve:
Passes through the cubital tunnel posterior to the medial epicondyle. Highly vulnerable to compression and iatrogenic injury.
*
Median Nerve:
Travels anterior to the elbow joint, deep to the bicipital aponeurosis.
*
Radial Nerve:
Divides into superficial (sensory) and deep (posterior interosseous nerve, motor) branches just anterior to the lateral epicondyle.
*
Brachial Artery:
Courses with the median nerve anteriorly, bifurcating into radial and ulnar arteries distal to the elbow.
Biomechanics
The elbow functions as a stable hinge joint, permitting flexion and extension, coupled with pronation and supination through the proximal radioulnar joint.
*
Normal ROM:
Typically 0-140 degrees of flexion-extension and approximately 80 degrees of pronation and 80 degrees of supination. A functional arc for most activities of daily living (ADLs) is considered to be 30-130 degrees of flexion and 50 degrees of pronation-supination.
*
Primary Stabilizers:
Ulnohumeral articulation, MCL, and LUCL.
*
Secondary Stabilizers:
Radial head and joint capsule.
*
Consequences of Arthritis:
PTEA results in progressive loss of joint congruity, osteophyte formation, capsular contracture, and often, secondary impingement. These changes lead to pain, crepitus, and a progressive reduction in the functional arc of motion. In some cases, articular cartilage damage can lead to altered joint mechanics and potentially instability.
Indications & Contraindications
The decision-making process for managing PTEA in young adults is complex, balancing symptom relief, functional restoration, and joint preservation with long-term durability.
Non-Operative Indications
Non-operative management is typically the first line of treatment for patients with mild to moderate symptoms, minimal functional limitation, or those with significant comorbidities precluding surgery.
*
Mild pain and functional limitation:
Symptoms manageable with conservative measures.
*
Early stage arthritis:
Minimal radiographic changes, no significant mechanical symptoms.
*
Acceptable range of motion:
Functional arc for ADLs maintained.
*
Patient preference:
Unwillingness or inability to undergo surgery.
*
Medical comorbidities:
Conditions that significantly increase surgical risk.
Conservative strategies include activity modification, non-steroidal anti-inflammatory drugs (NSAIDs), physical therapy focused on ROM and strengthening, and judicious use of intra-articular corticosteroid injections. Viscosupplementation is of unproven benefit in the elbow.
Operative Indications
Surgical intervention is considered when non-operative measures fail to provide adequate relief, or when there are significant functional impairments. In young adults, the emphasis is often on joint-preserving procedures where appropriate.
- Persistent, debilitating pain: Unresponsive to a comprehensive course of conservative treatment.
- Significant loss of functional ROM: Impairing ADLs, work, or recreational activities (e.g., less than 100 degrees total arc of flexion-extension, or restricted pronation/supination).
- Mechanical symptoms: Locking, clicking, catching due to loose bodies or impingement from osteophytes.
- Progressive radiographic changes: Worsening joint space narrowing, subchondral sclerosis, or osteophyte formation.
- Associated pathology: Symptomatic ulnar nerve compression, persistent instability (if correctable), or symptomatic osteochondral defects.
- Failed previous surgical intervention: Requiring salvage.
Contraindications
Absolute contraindications for most elective elbow surgeries include:
*
Active elbow or systemic infection:
Must be resolved prior to elective surgery.
*
Severe soft tissue compromise:
Insufficient soft tissue envelope for safe surgical access and wound closure.
*
Unrealistic patient expectations:
Inability to comprehend potential outcomes, limitations, or rehabilitation requirements.
*
Significant systemic medical comorbidities:
Uncontrolled conditions making the risks of anesthesia and surgery prohibitive.
Relative contraindications may include severe osteoporosis (for arthroplasty), history of chronic pain syndrome (e.g., CRPS), or severe neurological deficits impacting rehabilitation adherence. For total elbow arthroplasty (TEA) in particular, very young age, high-demand lifestyle (heavy manual labor, contact sports), or poor bone stock are relative contraindications due to increased risk of implant loosening and wear.
Operative vs. Non-Operative Indications Summary Table
| Feature | Non-Operative Management | Operative Management (Joint Preservation) | Operative Management (Arthroplasty - Salvage) |
|---|---|---|---|
| Pain | Mild to moderate, intermittent, tolerable | Persistent, moderate-to-severe, limiting ADLs | Severe, constant, disabling, unresponsive to other measures |
| Functional ROM | Functional arc maintained (e.g., >30-130° flexion) | Significant loss, impacting ADLs (e.g., <100° arc, limited prono/sup) | End-stage, severe stiffness, debilitating |
| Radiographic | Mild joint space narrowing, minimal osteophytes | Moderate osteophytes, loose bodies, some joint space narrowing | End-stage, severe joint destruction, bone loss, subchondral collapse |
| Mechanical Symps. | Absent or infrequent | Frequent locking, catching, painful crepitus | May be present, but severe pain and stiffness dominate |
| Patient Age | Any age, preferred for elderly with low demand | Young to middle-aged adults, active | Young adults (last resort), low-demand patients, revision candidates |
| Associated Path. | None or well-managed (e.g., mild ulnar neuropathy) | Symptomatic ulnar nerve compression, instability, malunion | Severe bone loss, irreparable instability, failed previous surgeries |
| General Health | Good, or significant comorbidities precluding surgery | Good, able to undergo surgery & rehabilitation | Good, able to undergo complex surgery & rehabilitation |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential to anticipate surgical challenges, optimize outcomes, and minimize complications in patients with PTEA.
Clinical Evaluation
A comprehensive history should detail the original injury, time to diagnosis, previous treatments (surgical and non-surgical), current pain characteristics, functional limitations, and patient expectations. Physical examination must include:
*
Inspection:
Swelling, deformity, scars, skin integrity.
*
Palpation:
Tenderness over specific bony landmarks (epicondyles, olecranon, radial head), joint line, or nerve pathways.
*
Range of Motion:
Active and passive flexion, extension, pronation, supination, comparing to the contralateral side if uninvolved. Note end-feel (bony vs. soft tissue).
*
Stability Assessment:
Varus/valgus stress testing at 0 and 30 degrees of flexion, posterolateral rotatory instability (PLRI) testing.
*
Neurovascular Exam:
Sensory and motor function of the ulnar, median, and radial nerves. Check distal pulses.
Imaging
-
Standard Radiographs:
- Anteroposterior (AP) and Lateral Views: Essential for assessing joint space narrowing, osteophyte formation (anterior coronoid, posterior olecranon, radial head), subchondral sclerosis, loose bodies, and overall alignment.
- Oblique Views: To better visualize specific compartments.
- Capitellar View (Greenspan): Useful for assessing the capitellum and radial head.
- Stress Views: If instability is suspected (e.g., valgus stress for MCL, varus stress for LCL).
-
Computed Tomography (CT) Scan:
- Crucial for PTEA: Provides detailed 3D bony anatomy, excellent for delineating osteophytes, identifying and localizing loose bodies, assessing malunion of previous fractures, and evaluating bone stock, particularly for arthroplasty planning. CT with 3D reconstructions can precisely map sites of impingement and guide osteophyte resection.
-

-
Magnetic Resonance Imaging (MRI):
- Less commonly used for primary assessment of PTEA unless soft tissue pathology (e.g., osteochondral lesions, ligamentous integrity, synovitis) is strongly suspected and cannot be adequately assessed by other means. It offers superior visualization of cartilage, ligaments, and soft tissues.
Patient Counseling
A thorough discussion with the patient is vital. It should cover the diagnosis, available treatment options (operative and non-operative), realistic goals, potential benefits, risks, and expected post-operative rehabilitation. It is crucial to manage expectations regarding pain relief, ROM improvement, and activity limitations, especially in the context of joint-preserving procedures versus arthroplasty.
Patient Positioning
The choice of patient position depends on the planned surgical approach and the extent of required exposure.
*
Lateral Decubitus Position:
*
Preferred for most comprehensive elbow surgeries.
The patient is positioned laterally, and the affected arm is placed on a padded arm holder or a sterile table, allowing for full flexion, extension, pronation, and supination. This position provides excellent access to medial, lateral, and posterior aspects of the elbow, facilitating ulnar nerve dissection, collateral ligament work, and arthrotomy. Requires careful padding of bony prominences and neural structures.
*
Supine Position with Arm Board:
* Suitable for anterior approaches or less extensive procedures, but limits access to the posterior and often medial/lateral compartments without significant patient repositioning.
*
Prone Position:
* Less commonly used for PTEA, but may be considered for extensive posterior approaches, particularly if a concomitant ipsilateral shoulder procedure is planned.
Regardless of the position, meticulous attention to padding (especially the ulnar nerve, peroneal nerve at the fibular head, and axillary padding) is paramount to prevent iatrogenic nerve compression or injury. A tourniquet is typically applied to the proximal arm.
Detailed Surgical Approach / Technique
The choice of surgical technique for PTEA in young adults hinges on the severity of arthritis, primary pathology (stiffness, pain, instability, loose bodies), and patient factors. Joint-preserving procedures are generally preferred over arthroplasty.
General Principles of Surgical Management for PTEA
- Debridement of osteophytes: Removal of impinging bone spurs, particularly at the olecranon, coronoid, radial head, and distal humerus.
- Loose body removal: Excision of any intra-articular fragments.
- Capsular release: Meticulous anterior and posterior capsulectomy to address stiffness. Medial and lateral capsular releases may also be necessary.
- Ulnar nerve neurolysis: Often indicated due to compression or tethering, especially with posterior osteophytes or valgus deformity. Transposition may be required.
- Address associated pathology: Ligament repair/reconstruction for instability, corrective osteotomy for malunion.
Arthroscopic Arthrolysis and Debridement
Arthroscopy is a minimally invasive option for less severe PTEA, particularly when stiffness is primarily due to capsular contracture, minor osteophyte formation, or loose bodies.
*
Indications:
Mild to moderate PTEA, significant stiffness with good joint congruity, symptomatic loose bodies, anterior or posterior impingement.
*
Advantages:
Smaller incisions, potentially faster recovery, less soft tissue disruption.
*
Limitations:
Difficult in cases of severe arthrofibrosis, significant osteophyte burden, severe bony deformities, or when extensive capsular release is required. Risk of neurovascular injury.
Technique
- Patient Positioning: Lateral decubitus or prone, arm secured in a traction tower.
-
Portals:
- Proximal Anteromedial (PAM): Between brachialis and medial epicondyle, median nerve risk.
- Proximal Anterolateral (PAL): Between brachioradialis and biceps, radial nerve risk.
- Direct Lateral: Just proximal to the radial head.
- Soft Spot (PL): Posterior to the lateral epicondyle, through the anconeus-triceps interval. Safest for posterior viewing/working.
- Posterolateral (PM): Posterior to the medial epicondyle, avoiding ulnar nerve.
- Fluid extravasation is a significant risk.
-
Procedure:
- Diagnostic Arthroscopy: Systematically visualize all compartments (anterior, posterior, medial, lateral).
- Synovectomy: Partial or complete synovectomy to reduce inflammation.
- Loose Body Removal: Identification and extraction of any intra-articular loose bodies.
- Osteophyte Excision: Debridement of anterior osteophytes (coronoid, radial head, humeral trochlea) and posterior osteophytes (olecranon, humeral). A burr is used, taking care to avoid damaging articular cartilage.
- Capsular Release: Anterior capsulectomy is performed with a shaver/radiofrequency wand. Posterior capsulectomy involves meticulous release while protecting the ulnar nerve.
-

- Post-Procedure: Dynamic assessment of ROM. Closure of portals.
Open Arthrolysis and Debridement (Capsular Release and Osteophyte Excision)
Open arthrolysis is often indicated for more severe PTEA with significant stiffness, extensive osteophyte formation, or when associated pathologies (e.g., ulnar nerve compression, malunion) require direct access.
Technique (e.g., Posterior Approach with Ulnar Nerve Transposition)
- Incision: A posterior midline skin incision centered over the olecranon, extending proximally along the humerus and distally along the ulna.
-
Ulnar Nerve Identification and Protection:
- The ulnar nerve is identified proximal to the cubital tunnel, carefully dissected free, and protected throughout the procedure. It is often entrapped by scar tissue or posterior osteophytes.
- Anterior Transposition: In cases of severe PTEA, recurrent ulnar nerve symptoms, or if extensive medial osteophyte removal/capsular release is performed, the ulnar nerve is typically transposed anteriorly beneath the flexor-pronator mass to prevent post-operative subluxation or compression.
-
Triceps Management:
- Triceps Sparing (Paratricipital): The triceps is elevated subperiosteally from the medial and lateral aspects of the olecranon to preserve its integrity. This provides good posterior access.
- Triceps Splitting: A longitudinal split in the triceps fascia and muscle provides direct access to the posterior humerus and olecranon fossa.
- V-Y Triceps Plastry: A V-shaped incision into the triceps tendon with distal release, allowing proximal retraction for wide exposure. The V is closed in a Y-shape for lengthening. This provides maximal posterior exposure, particularly for total elbow arthroplasty or complex reconstructions.
-
Posterior Debridement:
- The olecranon fossa is cleared of scar tissue and osteophytes. A burr or osteotome is used to debride posterior humeral osteophytes and reshape the olecranon.
- The posterior capsule is released.
-
Lateral and Medial Access (for 360-degree release):
- Lateral: The anconeus and common extensor origin are elevated. The radial head and capitellum are visualized. Lateral osteophytes and loose bodies are removed. The lateral capsule is released.
- Medial: The common flexor origin is elevated (after ulnar nerve transposition). Medial osteophytes and loose bodies are removed. The medial capsule is released. Care is taken to protect the MCL if stable; however, sometimes partial release is needed for ROM.
-
Anterior Debridement:
- After meticulous capsular release, the elbow is flexed to expose the anterior compartment.
- Osteophytes from the coronoid, radial head, and anterior trochlea are debrided using an osteotome or burr.
- Anterior capsular release is performed.
- Dynamic Assessment: After debridement and release, the elbow is taken through a full ROM to assess the achieved arc and identify any remaining impingement or restrictions.
- Closure: The capsule is generally not repaired tightly to prevent recurrence of stiffness. The triceps may be repaired if split. Subcutaneous layers and skin are closed.
Other Joint Preservation Techniques (for specific indications)
-
Interposition Arthroplasty:
- Indications: End-stage PTEA in young adults where TEA is undesirable, often in cases of poor bone stock or prior infection.
- Technique: Excision of damaged articular surfaces, followed by placement of a biological interposition material (e.g., fascia lata autograft, Achilles tendon allograft, dermal allograft) between the resected bone ends. This creates a pseudoarthrosis, aiming to reduce pain and improve motion without the use of prosthetic implants.
- Outcomes: Variable, generally better for pain relief than ROM. Graft failure and recurrent stiffness are concerns.
-
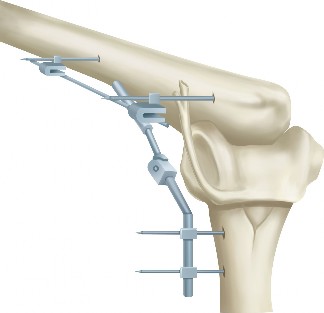
Distraction Arthroplasty:
- Indications: For painful, stiff, and unstable elbows where joint preservation is desired.
- Technique: Application of an external fixator across the elbow joint to unload the articular surfaces and maintain a gap, allowing for fibrocartilage formation. Often combined with arthrolysis.
- Outcomes: Can improve pain and ROM, but carries risks of pin tract infection, neurovascular injury, and requires prolonged external fixation. Not widely adopted due to complexity and complication profile.
-
Corrective Osteotomy:
- Indications: Symptomatic malunion of a previous fracture leading to PTEA or significant mechanical axis deviation.
- Technique: Osteotomy to correct angular or rotational deformity, restoring more normal joint mechanics. May be combined with arthrolysis.
Total Elbow Arthroplasty (TEA)
TEA is generally considered a salvage procedure for PTEA in young adults, reserved for severe, end-stage arthritis with disabling pain and loss of function when joint-preserving procedures are not feasible or have failed.
*
Indications:
End-stage PTEA, severe pain and functional loss, low-demand lifestyle, failed prior joint-preserving procedures, often in older populations. In young adults, this is a decision made with great caution due to finite implant longevity.
*
Contraindications (relative in young adults):
High-demand activities, infection, severe bone loss, neurovascular compromise.
*
Types:
Linked (constrained) and unlinked (resurfacing) prostheses. Linked prostheses are more common for posttraumatic arthritis due to often compromised ligamentous stability.
*
*
Technique:
Typically performed via a posterior approach with a V-Y triceps plasty. The humeral and ulnar canals are reamed, and prosthetic components are cemented or press-fitted. The joint is reconstructed to provide stability and a functional ROM.
Complications & Management
Elbow surgery for PTEA, particularly in the context of stiff, previously traumatized joints, is associated with a significant complication rate.
Intraoperative Complications
- Neurovascular Injury: Ulnar nerve is most vulnerable, but median and radial nerves, and the brachial artery can also be injured. Meticulous dissection and identification are critical. If identified, primary repair or grafting may be necessary.
- Fracture: Iatrogenic fracture during osteophyte removal, aggressive manipulation, or implant insertion (TEA). Requires immediate fixation.
- Excessive Bleeding: May obscure the surgical field and lead to hematoma formation. Careful hemostasis and tourniquet use are important.
Early Postoperative Complications
- Infection: Superficial or deep. Requires aggressive debridement, IV antibiotics, and possibly staged revision for deep infections (especially for TEA).
- Hematoma: May require aspiration or surgical evacuation.
- Persistent Pain/Stiffness: Incomplete release, recurrence of HO, or residual arthritis.
- Ulnar Nerve Symptoms: New-onset or worsening numbness/tingling, weakness. May require revision neurolysis or transposition.
- Wound Complications: Dehiscence, necrosis. Management depends on severity, ranging from local wound care to flap coverage.
- Complex Regional Pain Syndrome (CRPS): Early recognition and multidisciplinary treatment are crucial.
Late Postoperative Complications
- Recurrence of Stiffness/Heterotopic Ossification (HO): The most common complication after arthrolysis. Managed with prophylactic NSAIDs/radiation, early rehabilitation. If severe, may require repeat arthrolysis.
- Implant Loosening/Wear (for Arthroplasty): A significant concern in young adults due to higher activity levels. Requires revision surgery.
- Persistent Instability: Can occur after ligament release or in revision cases. May require ligament reconstruction or conversion to TEA.
- Pain: Residual arthritis, hardware irritation, or underlying unresolved pathology.
-
 - Nonunion/Malunion (after osteotomy): May require revision fixation or bone grafting.
Common Complications, Incidence, and Salvage Strategies
| Complication | Typical Incidence (Range) | Salvage Strategy |
|---|---|---|
| Recurrent Stiffness/HO | 20-50% after arthrolysis | Prophylaxis (NSAIDs, radiation post-op). Early, aggressive ROM. If established severe HO limiting function: repeat arthrolysis/HO excision (often at 6-12 months post-initial surgery), potentially with continued prophylaxis. |
| Ulnar Nerve Neuropathy | 5-20% (transient), 1-5% (persistent) | Intraoperative protection/transposition. Post-op: observation, bracing. If persistent/progressive: revision neurolysis, anterior transposition. |
| Infection | 1-5% for open surgery; <1% for arthroscopy | Acute: Irrigation & debridement, IV antibiotics. Chronic/TEA: explantation, staged revision, spacer, long-term antibiotics. |
| CRPS | <5% | Early recognition, multidisciplinary pain management (PT, OT, nerve blocks, medications). |
| Joint Instability | Variable, depends on initial pathology and collateral ligament management | Conservative management (bracing, PT). If persistent/symptomatic: collateral ligament repair/reconstruction. Failed preservation: consideration of total elbow arthroplasty (TEA) for stability. |
| Implant Loosening/Wear (TEA) | 10-20% at 10 years in young, active patients | Revision TEA (component exchange, bone grafting). If extensive bone loss or repeat failures: resection arthroplasty, fusion (rarely). |
| Fracture (periprosthetic/iatrogenic) | <5% | Depends on type and location: open reduction internal fixation (ORIF), revision of implant (if periprosthetic). |
| Neurovascular Injury (other) | <1% (radial, median nerve, brachial artery) | Immediate intraoperative repair. Post-op: observation, EMG studies. Tendon transfers for motor deficits. |
| Wound Dehiscence/Necrosis | <5% | Local wound care. If severe: debridement, primary closure, local or regional flap coverage. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is as critical as the surgical procedure itself in optimizing outcomes following PTEA surgery. The goal is to restore ROM, strength, and function while protecting the surgical repair and preventing recurrence of stiffness.
General Principles
- Early Motion: Crucial for preventing stiffness and promoting cartilage healing. Often initiated within 24-48 hours post-surgery.
- Pain Management: Adequate analgesia is essential to allow patient participation in therapy.
- Protection: Balancing early motion with protection of repaired structures (e.g., collateral ligaments, triceps repair).
- Progressive Loading: Gradual increase in resistance and activity as healing progresses.
- Heterotopic Ossification (HO) Prophylaxis: NSAIDs (e.g., indomethacin for 3-6 weeks) or localized low-dose radiation post-op, especially for high-risk patients (e.g., prior HO, severe trauma, head injury).
Phase I: Immediate Post-Operative (Weeks 0-3)
- Goals: Control pain and swelling, protect surgical site, initiate early, gentle ROM.
-
Immobilization:
- Often a soft dressing or splint for comfort and protection.
- Hinged elbow brace may be used for some procedures (e.g., collateral ligament repair, TEA) to allow protected ROM within prescribed arcs, blocking extension or flexion as needed.
-
Exercises:
- Active-Assisted ROM (AAROM): Gentle flexion and extension, pronation and supination (if not contraindicated). Gravity-assisted movements.
- Continuous Passive Motion (CPM): May be used for 4-6 hours daily, particularly after extensive arthrolysis, to improve and maintain ROM.
- Gentle hand and wrist exercises: To prevent stiffness and promote circulation.
- Weight Bearing: Non-weight bearing (NWB) for the affected extremity.
- Ulnar Nerve: If transposed, maintain elbow at 90 degrees flexion in a soft dressing initially to minimize tension.
Phase II: Early Motion and Strengthening (Weeks 3-8)
- Goals: Increase active ROM, initiate gentle strengthening, improve control.
- Bracing: Continue use of hinged brace as indicated, gradually increasing ROM limits. Wean as stability and motion improve.
-
Exercises:
- Active ROM (AROM): Progress from AAROM to full AROM as tolerated, without pain.
- Low-load, long-duration stretching: To address specific ROM deficits.
- Gentle Isometric Strengthening: Biceps, triceps, forearm flexors/extensors at multiple angles.
- Scar Management: Gentle massage, mobilization to prevent adhesions.
- Functional Activities: Begin light, non-resistive ADLs.
Phase III: Progressive Strengthening and Functional Integration (Weeks 8-16)
- Goals: Restore full ROM, progressively increase strength and endurance, prepare for return to activity.
-
Exercises:
- Progressive Resistance Exercises (PREs): Using light weights, resistance bands for biceps, triceps, forearm muscles.
- Dynamic Stretching: To improve flexibility.
- Proprioceptive Training: Balance and coordination drills for the upper extremity.
- Endurance Training: Repetitive, low-resistance exercises.
- Return to Activity: Gradual introduction of sport-specific or work-specific activities. Avoid heavy lifting or impact activities.
Phase IV: Return to Activity (Weeks 16+)
- Goals: Maximal strength, power, and endurance; safe return to full activity.
-
Exercises:
- Advanced strengthening, plyometrics (if appropriate for the procedure, less common for TEA).
- Sport-specific or work-specific conditioning.
- Criteria for Return to Activity: Full, pain-free ROM, symmetrical strength (>80% contralateral side), no instability, good endurance. For TEA, patients are often advised against heavy lifting (>5-10 lbs) and repetitive impact activities lifelong.
Special Considerations for Total Elbow Arthroplasty (TEA)
Rehabilitation after TEA is generally more protective due to concerns about implant loosening and failure.
*
Initial Immobilization:
Often in a posterior splint at 90 degrees flexion for 2-3 days, then a hinged brace allowing controlled ROM.
*
Weight Bearing Restrictions:
Strict lifelong limits on lifting (typically 1-2 kg repetitively, 5 kg occasionally).
*
Activity Restrictions:
Avoid impact sports, contact sports, or activities involving pushing up from a chair with the operative arm.
*
Focus:
Pain relief and functional ROM, rather than achieving high-level athletics.
Summary of Key Literature / Guidelines
The management of posttraumatic elbow arthritis in young adults remains an area of ongoing research and clinical debate, largely due to the challenging patient demographic and the paucity of high-level evidence, particularly randomized controlled trials. Most current recommendations are based on expert consensus, retrospective series, and biomechanical studies.
- Joint Preservation vs. Arthroplasty: The prevailing philosophy in young, active adults is to exhaust joint-preserving options before considering total elbow arthroplasty (TEA). Studies consistently show that TEA in younger, higher-demand patients has higher rates of aseptic loosening, infection, and revision compared to older, lower-demand populations. The 10-year survival rate for TEA generally ranges from 70-90% but decreases in younger individuals.
- Arthroscopic vs. Open Arthrolysis: Both arthroscopic and open arthrolysis have demonstrated effectiveness in improving ROM and reducing pain in stiff elbows, with comparable outcomes in properly selected patients. Arthroscopy offers the advantage of smaller incisions and potentially quicker initial recovery for less severe cases. However, open arthrolysis provides superior exposure for extensive osteophyte debridement, complex capsulectomy, and concomitant ulnar nerve management or malunion correction. A systematic review by Lindenhovius et al. (2010) found similar ROM improvements between open and arthroscopic techniques, but higher complication rates for open surgery. Modern arthroscopic techniques, however, have evolved.
- Heterotopic Ossification (HO) Prophylaxis: The efficacy of indomethacin and low-dose radiation therapy in preventing HO after elbow trauma and surgery is well-established. Numerous studies and meta-analyses support their use, particularly in high-risk patients. A common regimen involves indomethacin 25mg TID for 3-6 weeks or a single dose of 700 cGy radiation administered within 24-72 hours post-operatively.
- Interposition Arthroplasty: While an appealing concept for avoiding prosthetic implants, outcomes for interposition arthroplasty are mixed. Studies by various authors (e.g., Steinmann et al., Hotchkiss et al.) demonstrate variable pain relief and ROM improvement, often with graft failure and recurrent stiffness as concerns. It remains an option for selected patients with diffuse articular damage and good soft tissue coverage who are unwilling or unsuitable for TEA.
- Distraction Arthroplasty: While biomechanically sound for unloading the joint, clinical outcomes of distraction arthroplasty have been inconsistent, with high rates of pin tract infection and prolonged external fixation. Its role is limited to specific indications, primarily severe, unstable, painful elbows not amenable to other preservation techniques.
- Ulnar Nerve Management: The literature consistently recommends prophylactic ulnar nerve neurolysis or anterior transposition in cases of significant posterior osteophyte debridement or when the nerve is found to be tethered or compressed during surgery, to prevent post-operative neuropathy.
In summary, the optimal management of PTEA in young adults requires a nuanced approach, prioritizing joint-preserving procedures such as arthrolysis (open or arthroscopic) and meticulous debridement. These interventions aim to restore functional ROM and reduce pain while delaying or, ideally, precluding the need for arthroplasty. When arthroplasty becomes necessary, careful patient selection, counseling on activity restrictions, and a clear understanding of implant longevity are paramount. Continuous advancements in surgical techniques, materials, and rehabilitation protocols aim to improve long-term outcomes in this challenging patient population.
