
Complex Elbow Dislocation: Demystifying the Posteromedial Case
Patient Presentation & History
A 48-year-old male, a recreational basketball player, presented to the emergency department following a fall during a game. He reported falling directly onto an outstretched left upper extremity, landing with his elbow in slight flexion, valgus, and forearm supination. He experienced immediate, severe pain and deformity of the left elbow, with an inability to move the limb. There was no direct impact to the head or other body parts. His medical history was significant for well-controlled hypertension and a remote history of shoulder arthroscopy, but no prior elbow injuries or surgeries. He denied any neurological deficits or numbness prior to the injury.
Clinical Examination
Upon arrival, the patient was in acute distress with significant pain.
*
Inspection:
Gross deformity of the left elbow was evident, consistent with a posterior dislocation. Marked swelling was present globally, most pronounced posteromedially, and ecchymosis was developing rapidly. The skin overlying the medial epicondyle appeared stretched but intact, without signs of tenting or impending compromise.
*
Palpation:
Tenderness was exquisite over the medial epicondyle, olecranon, and the proximal ulna. The ulnar nerve sulcus was tender, but the nerve itself was not palpable as entrapped. A palpable defect was noted posteriorly between the olecranon and the distal humerus.
*
Range of Motion (ROM):
Actively and passively, ROM was severely restricted due to pain and mechanical block. The elbow was held in approximately 30-40 degrees of flexion. Any attempt at supination or pronation was exquisitely painful and limited.
*
Neurological Assessment:
Sensation to light touch was intact in all dermatomes (C5-T1). Motor function was intact, although limited by pain, with full wrist and finger flexion/extension, and gross elbow flexion/extension power present in a limited arc. Specifically, ulnar nerve function (FCU, FDP ulnar half, intrinsic hand muscles) was assessed and found to be grossly intact.
*
Vascular Assessment:
Radial and ulnar pulses were 2+ bilaterally and symmetrically. Capillary refill was brisk in all digits. No pallor or paresthesia was reported distally.
Imaging & Diagnostics
Initial imaging focused on plain radiographs to confirm dislocation and assess for associated fractures.
-
Plain Radiographs:
- Anteroposterior (AP) and lateral views of the elbow demonstrated a posteromedial dislocation of the ulna relative to the humerus.
- A significant fracture of the anteromedial coronoid process was clearly visible on the lateral view, displacing proximally.
- No obvious radial head fracture or olecranon fracture was identified on these initial views.
- The trochlea appeared to be displaced laterally relative to the coronoid fracture fragment.
-
 -
 -

Following initial radiographs, a closed reduction attempt was made in the emergency department under conscious sedation. The elbow was gently reduced, confirmed by post-reduction radiographs. However, despite reduction, the elbow remained grossly unstable, particularly with valgus stress and supination, demonstrating persistent posteromedial subluxation. This finding strongly suggested significant ligamentous and bony disruption.
-
Computed Tomography (CT) Scan:
- Given the post-reduction instability and the suspected coronoid fracture, a CT scan of the elbow was obtained to delineate the fracture morphology, displacement, and identify any other subtle bony injuries.
- The CT confirmed a large, comminuted fracture of the anteromedial facet of the coronoid process (O'Driscoll Type III), involving more than 50% of the coronoid height. This fragment was significantly displaced and rotated.
- There was no associated radial head or olecranon fracture, which helped differentiate from a terrible triad.
- The CT also provided detailed assessment of the trochlear integrity and the overall joint alignment, confirming the posteromedial displacement pattern.
-
 -
 -
 -
- Magnetic Resonance Imaging (MRI): An MRI was not obtained pre-operatively as the diagnosis of a complex elbow dislocation with posteromedial rotatory instability (PMRRI) was established by clinical exam and CT. The need for surgical intervention was clear due to bony injury and gross instability. In cases where the extent of ligamentous injury is unclear or if occult chondral injuries are suspected, an MRI can be a valuable adjunct.
- Templating: Pre-operative templating was performed to plan for potential fixation devices for the coronoid fracture (e.g., small fragment plates, suture lasso constructs, or internal brace augmentation) and to consider the need for primary repair versus augmentation of the medial collateral ligament (MCL).
Differential Diagnosis
The presentation of elbow dislocation with associated coronoid fracture necessitates careful differentiation from other complex elbow instability patterns.
| Feature | Posteromedial Rotatory Instability (PMRRI) | Terrible Triad Injury | Simple Elbow Dislocation | Radial Head Fracture with LCL Injury (Essex-Lopresti equivalent) |
|---|---|---|---|---|
| Mechanism of Injury | Fall on outstretched hand (FOOSH) with valgus and supination. Ulna rotates posteromedially. | FOOSH with valgus and pronation. | FOOSH with hyperextension. | FOOSH with axial load and pronation/supination. |
| Key Bony Injury | Anteromedial coronoid fracture (O'Driscoll Type II/III). Typically no radial head fracture. | Coronoid fracture (often Type I/II), Radial head fracture (Mason Type II/III), Olecranon fracture sometimes. | None or avulsion fractures. | Radial head fracture (Mason Type I-III). Coronoid fracture is less common but can occur. |
| Key Ligamentous Injury | Medial Collateral Ligament (MCL) complex disruption (anterior bundle), +/- posterior bundle. Often intact LCL complex. | Lateral Collateral Ligament (LCL) complex disruption, +/- MCL involvement. | Variable, usually LCL +/- MCL disruption. | LCL complex disruption (often involving the LUCL). Distal radioulnar joint (DRUJ) disruption is hallmark of true Essex-Lopresti. |
| Direction of Dislocation | Posteromedial rotatory subluxation/dislocation of ulna relative to humerus. | Posterior or posterolateral dislocation of ulna relative to humerus. | Pure posterior or posterolateral dislocation. | No primary elbow dislocation, but radial head migrates proximally. |
| Elbow Stability Post-Reduction | Grossly unstable, especially with valgus and supination. Persistent posteromedial subluxation. | Grossly unstable, especially with varus and pronation. | Often stable after reduction in certain arcs, but can be unstable if ligamentous disruption is severe. | Elbow may be stable or subtly unstable depending on associated ligament damage. DRUJ instability is key. |
| Surgical Management | Almost universally operative. Fix coronoid, repair MCL. | Universally operative. Fix radial head, coronoid, repair LCL. | Often non-operative if stable after reduction. If unstable, LCL repair. | Operative for radial head and LCL. DRUJ stabilization if Essex-Lopresti. |
Surgical Decision Making & Classification
The decision for operative intervention was straightforward due to the gross instability of the elbow following closed reduction, coupled with a significant, displaced anteromedial coronoid fracture. This complex injury pattern, specifically posteromedial rotatory instability (PMRRI), is inherently unstable and carries a high risk of recurrent dislocation, poor functional outcomes, and premature degenerative changes if treated non-operatively or inadequately.
Key Classifications Guiding Management:
*
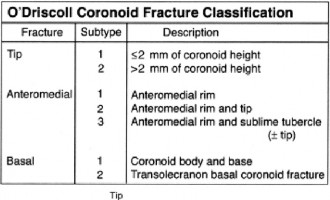
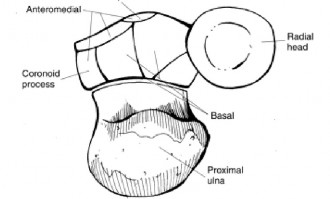
O'Driscoll's Classification of Coronoid Fractures:
This system categorizes coronoid fractures based on their anatomical location and involvement.
*
Type I:
Tip fractures.
*
Type II:
Fractures involving less than 50% of the coronoid height.
*
Type III:
Fractures involving 50% or more of the coronoid height (as seen in our case, Type III).
* The anteromedial facet subtype of Type III fractures, as presented here, is particularly critical in PMRRI as it represents the footprint for the anterior bundle of the MCL and provides the primary buttress against posteromedial rotation. Our patient’s fracture fell into the Type III category, indicating significant involvement of the main coronoid body and critical for stability.
*
Hotchkiss Classification of Elbow Instability:
While not a specific fracture classification, Hotchkiss broadly categorizes elbow instability. This case fits the description of a
complex instability
, characterized by both bony and ligamentous lesions leading to persistent instability after reduction.
*
Regan-Morrey / Mason Classification of Radial Head Fractures:
These were relevant for consideration, but ruled out in our case as there was no radial head fracture. Their absence helped narrow the diagnosis away from a terrible triad.
Given the O'Driscoll Type III anteromedial coronoid fracture and the documented gross instability of the MCL complex, operative stabilization was the definitive treatment. The surgical goals were anatomical reduction and stable fixation of the coronoid fracture, repair or reconstruction of the medial collateral ligament, and restoration of overall elbow stability through the full arc of motion.
Surgical Technique / Intervention
The patient was taken to the operating room for open reduction and internal fixation of the coronoid fracture and medial collateral ligament repair.
-
Anesthesia and Positioning:
- General endotracheal anesthesia was administered.
- The patient was positioned in the lateral decubitus position with the affected left arm draped free on a sterile arm board, allowing for full pronation, supination, flexion, and extension. A tourniquet was applied to the upper arm.
-
Surgical Approach:
- A medial utility incision was utilized, centered over the medial epicondyle and extending proximally along the medial supracondylar ridge and distally along the ulnar subcutaneous border.
- The ulnar nerve was identified proximally in the medial epicondylar groove and carefully mobilized and transposed anteriorly to protect it throughout the procedure. This is a crucial step to prevent iatrogenic injury and facilitate exposure.
- The medial collateral ligament complex was thoroughly inspected. As expected, the anterior bundle of the MCL was avulsed from its humeral origin and/or severely attenuated, consistent with the valgus instability. The posterior bundle and posterior capsule were also significantly disrupted.
- The flexor-pronator mass was partially detached from the medial epicondyle to gain access to the joint capsule and the coronoid fracture site. The posterior capsule was incised longitudinally to expose the posteromedial compartment.
-
Coronoid Fracture Fixation:
- The joint was opened, and the large anteromedial coronoid fracture fragment was clearly visualized. The fragment was manipulated back into anatomical position, carefully reducing it to the ulna.
- Initial reduction was maintained with a provisional K-wire.
- The chosen fixation method was a suture lasso technique combined with a small fragment buttress plate . Two non-absorbable sutures were passed through drill holes in the intact ulna, lassoing the coronoid fragment and securing it proximally. This provided robust compression.
- Additionally, a 1.5mm or 2.0mm pre-contoured low-profile buttress plate was applied to the anteromedial aspect of the ulna, spanning the fracture, to provide additional stability and counteract rotational forces. Screw length was carefully chosen to avoid articular penetration.
- Intraoperative fluoroscopy was used to confirm anatomical reduction and satisfactory implant placement.
-
Medial Collateral Ligament (MCL) Repair/Reconstruction:
- With the coronoid buttress restored, the MCL complex was addressed.
- The anterior bundle of the MCL, found to be avulsed from the humeral origin (or proximal to the coronoid fracture site), was directly repaired . Heavy non-absorbable sutures were passed through the avulsed ligament substance and then secured back to its anatomical footprint on the medial epicondyle via suture anchors placed in the humerus.
- The integrity of the repair was tested intraoperatively by applying valgus stress through a full arc of motion (0-130 degrees). The elbow demonstrated significantly improved stability, but some residual laxity was noted at terminal extension and supination.
- Given the significant disruption and the high demand of the patient's activity level, an internal brace augmentation using a strong non-absorbable suture tape (e.g., FiberTape) was performed to reinforce the MCL repair. This tape was passed from the medial epicondyle (through the suture anchor) to a trans-osseous tunnel in the ulna, replicating the course of the native anterior bundle of the MCL, providing immediate robust stability.
- Lateral Collateral Ligament (LCL) Assessment: The lateral aspect of the elbow was not exposed unless persistent posterolateral instability was noted. In this case, intraoperative stress testing in flexion and pronation did not reveal any LCL insufficiency, consistent with the pre-operative imaging findings. Therefore, no lateral repair was performed.
- Capsular and Soft Tissue Closure: The remaining joint capsule was closed. The flexor-pronator mass was reapproximated. The ulnar nerve was secured in its anterior transposition pocket. Subcutaneous tissues and skin were closed in layers.
- Post-Fixation Stability Assessment: After closure, the elbow's stability was re-assessed through a full range of motion. The elbow was stable from 30 to 130 degrees of flexion with no signs of re-dislocation or subluxation under valgus or varus stress, or with pronation/supination.
Post-Operative Protocol & Rehabilitation
The post-operative protocol was designed to protect the repaired structures while encouraging early, controlled motion to prevent stiffness and heterotopic ossification.
-
Immediate Post-Operative (Day 0-7):
- The elbow was immobilized in a posterior plaster splint in approximately 90 degrees of flexion with the forearm in neutral rotation for 5-7 days to allow for initial soft tissue healing.
- Ice and elevation were initiated to manage swelling.
- Pain management protocol was initiated.
-
Early Mobilization (Week 1-6):
- At the first post-operative visit, the splint was removed, and a custom or off-the-shelf hinged elbow brace was fitted.
- The brace was initially locked from 30 degrees of flexion to 90 degrees of flexion to protect the coronoid repair and MCL. The forearm was kept in neutral or slight pronation to minimize stress on the MCL.
- Passive range of motion (PROM) exercises were initiated under the supervision of a hand therapist, focusing on flexion and extension within the brace's allowed range.
- Active-assisted range of motion (AAROM) and gravity-assisted ROM were gradually introduced.
- Gentle forearm supination/pronation within pain limits.
- Active hand, wrist, and shoulder exercises were encouraged.
- Crucially, no active resisted elbow flexion, valgus stress, or aggressive supination was permitted.
- Wound care and removal of sutures/staples.
-
Progressive Rehabilitation (Week 6-12):
- The flexion-extension arc of the brace was gradually increased, typically by 10-15 degrees per week, aiming for full extension and flexion by 10-12 weeks.
- Forearm rotation was progressively increased.
- Gentle isometric exercises for elbow flexors and extensors were introduced.
- Light resistance exercises were initiated for wrist and shoulder.
- Manual therapy by the therapist to address joint mobility and soft tissue restrictions.
- No lifting restrictions above 1-2 pounds.
-
Strength and Functional Return (Week 12-6 Months):
- Brace weaning typically began around 12 weeks, depending on clinical stability and patient progress.
- Progressive strengthening exercises for the entire upper extremity, including eccentric and concentric loading.
- Introduction of sport-specific or activity-specific drills with low impact.
- Emphasis on gradual progression of weight-bearing and lifting.
- Close monitoring for signs of heterotopic ossification or contracture.
- Full return to unrestricted activities, including sports, was typically anticipated around 6 months, contingent on full restoration of strength, stability, and range of motion.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
- High Index of Suspicion for PMRRI: Any elbow dislocation, especially one with a subtle coronoid fracture or persistent instability after reduction, warrants thorough investigation for PMRRI. The mechanism of valgus + supination + axial load is highly suggestive.
- Meticulous Imaging Review: Don't rely solely on initial plain films. A CT scan is mandatory for precise characterization of coronoid fracture morphology (especially anteromedial facet involvement), size, and displacement. This dictates the surgical approach and fixation strategy.
- Anatomical Reduction of Coronoid Fragment: The coronoid process, particularly the anteromedial facet, is a critical bony buttress for elbow stability. Failure to anatomically reduce and stably fix the coronoid will inevitably lead to persistent instability, regardless of ligament repair.
-
Sequencing of Repair:
The common sequence for PMRRI (and other complex elbow dislocations) is:
- Bony stabilization first: Radial head, then coronoid.
- Medial ligamentous structures: MCL complex repair/reconstruction.
- Lateral ligamentous structures: LCL complex repair/reconstruction (if indicated).
- This "inside-out" or "outside-in" (depending on approach) and "bone-before-soft-tissue" approach helps restore the primary stabilizers sequentially, allowing each repair to be tested for residual instability.
- Robust MCL Repair/Augmentation: The MCL, specifically its anterior bundle, is the primary static stabilizer against valgus stress and plays a crucial role in PMRRI. A strong repair, often augmented with an internal brace, is essential for stability.
- Intraoperative Stability Assessment: After each step of fixation and repair, dynamically assess elbow stability through a full range of motion (0-130 degrees) under fluoroscopy. Ensure stability in various positions (pronation, supination, valgus, varus stress). This guides the need for further intervention.
- Ulnar Nerve Protection: The ulnar nerve is highly vulnerable during medial approaches to the elbow. Routine identification, neurolysis, and anterior transposition are often prudent to prevent iatrogenic injury.
- Early Controlled Motion: Initiate passive and active-assisted ROM within a protected arc as early as tolerated to prevent stiffness, contractures, and heterotopic ossification, while respecting the stability of the repairs. The arc of motion must be carefully defined to protect the healing structures.
Pitfalls:
- Missed Diagnosis/Underestimation of Instability: Treating a PMRRI as a "simple" dislocation or failing to identify the significant coronoid fracture leads to inadequate management and poor outcomes.
- Inadequate Coronoid Fixation: Using insufficient fixation (e.g., small screws only, non-anatomical reduction) for a large or comminuted coronoid fracture can lead to malunion, nonunion, or persistent instability.
- Failure to Address the MCL: While coronoid fixation restores the bony buttress, the MCL is paramount for valgus stability. Failure to repair or adequately augment a disrupted MCL will result in recurrent valgus/posteromedial instability.
- Overly Aggressive Early Rehabilitation: Pushing ROM too aggressively or allowing unprotected valgus stress or supination can lead to failure of the repairs, re-dislocation, or iatrogenic instability. Strict adherence to a progressive, protected protocol is essential.
- Heterotopic Ossification (HO): Complex elbow trauma, especially with extensive soft tissue dissection and open surgery, carries a high risk of HO. Prophylaxis with NSAIDs (e.g., indomethacin) or low-dose radiation post-operatively should be considered, particularly in high-risk patients.
- Stiffness and Contracture: Despite early motion, elbow stiffness is a common complication. Vigilant physical therapy and sometimes dynamic bracing or even manipulation under anesthesia may be required.
- Iatrogenic Ulnar Nerve Injury: Failure to identify and protect or transpose the ulnar nerve during a medial approach can lead to significant morbidity.
- Post-Traumatic Arthritis: Long-term follow-up is necessary due to the inherent risk of post-traumatic arthritis in complex elbow injuries, even with optimal surgical management.
