Medial Elbow Pain: Diagnosing & Treating Throwing Overload
Introduction & Epidemiology
Medial elbow pain in the overhead athlete represents a spectrum of pathologies resulting from repetitive valgus stress and tensile loading across the medial compartment. This constellation of injuries, often termed "throwing elbow," predominantly affects baseball players but is also observed in javelin throwers, volleyball players, and other athletes engaged in overhead sports. The high-velocity, high-force demands of throwing impart extreme valgus moments on the elbow, particularly during the late cocking and early acceleration phases, placing the ulnar collateral ligament (UCL) complex under significant tensile stress and the flexor-pronator mass under contractile stress.
The incidence of medial elbow pathology in overhead athletes, particularly UCL injuries, has demonstrably risen over the past two decades. This increase is often attributed to several factors including increased participation in organized youth sports, year-round play, specialization at younger ages, and increased throwing velocity and pitch counts. UCL insufficiency, ranging from partial tears to complete ruptures, is a debilitating injury that often necessitates surgical intervention for return to competitive sport. Other common etiologies include medial epicondylar apophysitis (in skeletally immature athletes), flexor-pronator mass tendinopathy or strains, and ulnar nerve irritation or subluxation. Accurate and timely diagnosis is paramount for guiding appropriate management, which ranges from non-operative rehabilitation to complex surgical reconstruction.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy and biomechanics of the medial elbow is fundamental to both diagnosis and treatment of throwing injuries.
Ulnar Collateral Ligament Complex
The UCL is the primary static stabilizer against valgus stress at the elbow, providing approximately 54% of this resistance. It comprises three distinct bundles:
*
Anterior Bundle (AB)
: Originates from the anterior-inferior aspect of the medial epicondyle and inserts onto the sublime tubercle of the ulna. This is the strongest and most critical component, providing the primary restraint to valgus stress from 30° to 120° of flexion. It consists of anterior and posterior fascicles, which become taut at different degrees of flexion. The anterior fascicle is taut in extension, while the posterior fascicle is taut in flexion.
*
Posterior Bundle (PB)
: Originates from the posterior aspect of the medial epicondyle and inserts onto the medial olecranon. It is a fan-like thickening of the posterior capsule, becoming taut in extreme flexion and offering secondary valgus stability.
*
Transverse Bundle (TB) / Ligament of Cooper
: Connects the olecranon to the coronoid process. Its function is often considered negligible in valgus stability, primarily serving to deepen the trochlear notch.
Flexor-Pronator Mass
The flexor-pronator mass originates from the medial epicondyle and consists of five muscles: pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, and flexor carpi ulnaris. These muscles serve as dynamic stabilizers of the medial elbow, particularly under valgus load. They resist valgus stress by compressing the joint and providing a muscular counterforce to the tensile strain on the UCL. Overuse can lead to tendinopathy, strains, or partial avulsions from the medial epicondyle.
Ulnar Nerve
The ulnar nerve traverses the cubital tunnel, a fibro-osseous canal on the posteromedial aspect of the elbow. It passes posterior to the medial epicondyle and deep to the arcuate ligament (Osborne's ligament). Its superficial location makes it vulnerable to traction, compression, or friction injuries in the setting of valgus instability, osteophyte formation, or repetitive microtrauma, leading to cubital tunnel syndrome. Subluxation of the nerve over the medial epicondyle during elbow flexion can also occur.
Biomechanics of Throwing
The overhead throwing motion is a complex kinetic chain involving the entire body, but the elbow bears significant load. It is classically divided into six phases:
1.
Wind-up
: Minimal elbow stress.
2.
Early Cocking
: Shoulder abduction and external rotation begin.
3.
Late Cocking
: Peak valgus stress on the medial elbow, with the elbow typically at 90° of flexion and maximal shoulder external rotation. The UCL is maximally loaded in tension. The flexor-pronator mass activates eccentrically to decelerate pronation and wrist extension, and concentrically to provide dynamic stability.
4.
Acceleration
: Explosive internal rotation of the shoulder, elbow extension, and pronation. Shear forces are high across the olecranon and radial head.
5.
Deceleration
: High tensile forces across the posterior elbow (triceps, posterior capsule) and anterior shoulder.
6.
Follow-through
: Dissipation of energy.
Repetitive supraphysiologic valgus stress, particularly during the late cocking and acceleration phases, can overwhelm the static and dynamic stabilizers, leading to injury.

Indications & Contraindications
Management of medial elbow pain due to throwing overload necessitates a tailored approach based on the specific pathology, patient age, activity level, and response to initial non-operative treatment.
Non-Operative Indications
Non-operative management is the initial treatment for most medial elbow pathologies, especially in skeletally immature athletes or those with mild instability or tendinopathy.
*
Medial Epicondylar Apophysitis
: Rest, activity modification, anti-inflammatory medication, physical therapy focusing on stretching and strengthening.
*
Flexor-Pronator Tendinopathy/Strain
: Rest, activity modification, NSAIDs, eccentric strengthening programs, modalities (e.g., ultrasound, iontophoresis). Platelet-rich plasma (PRP) injections may be considered in refractory cases, though evidence remains mixed.
*
UCL Sprain (Grade I/II)
: Rest, bracing (hinged elbow brace to limit valgus stress), physical therapy focused on kinetic chain strengthening, scapular stabilization, and throwing mechanics analysis. Gradual return to throwing program.
*
Ulnar Nerve Neuropathy (mild)
: Activity modification, NSAIDs, night splinting in extension, nerve gliding exercises, physical therapy.
Operative Indications
Surgical intervention is generally reserved for patients who have failed a comprehensive non-operative rehabilitation program or those with specific pathologies demanding surgical repair or reconstruction.
*
UCL Reconstruction (UCLR) / "Tommy John Surgery"
:
*
Chronic UCL insufficiency
: Symptomatic valgus instability despite 6+ months of comprehensive non-operative management in a high-demand overhead athlete.
*
Acute complete UCL rupture
: In a professional or collegiate overhead athlete where prompt return to high-level play is critical.
*
Partial UCL tear with high-grade instability
: Documented by physical exam (positive valgus stress test, moving valgus stress test) and imaging (MRI arthrogram showing gapping).
*
UCL Repair (with or without internal brace augmentation)
:
*
Acute avulsion of the UCL
: From the medial epicondyle or sublime tubercle, particularly in athletes with excellent tissue quality.
*
Proximal or distal tears with adequate tissue for direct repair
: Especially effective when augmented with a suture tape internal brace, which allows for earlier and potentially faster return to sport compared to traditional reconstruction.
*
Medial Epicondylectomy/Debridement
: For recalcitrant flexor-pronator tendinopathy that has failed extensive non-operative management.
*
Ulnar Nerve Transposition
:
*
Recalcitrant cubital tunnel syndrome
: Failing non-operative management, especially with documented nerve compression or subluxation.
*
Prophylactic transposition
: Often performed concomitantly with UCLR to decompress the nerve and protect it during graft harvest and tunnel creation.
*
Removal of loose bodies/osteophytes
: For mechanical symptoms or ulnar nerve irritation.
| Indication Category | Non-Operative Management | Operative Management |
|---|---|---|
| UCL Injury | Grade I/II sprains; Partial tears with no valgus instability, responding to physical therapy, brace, activity modification. Skeletally immature athletes with apophysitis without true ligamentous injury. | Chronic symptomatic valgus instability (6+ months non-op failure) in overhead athlete. Acute complete rupture in high-level athlete. Partial tear with high-grade instability. Acute avulsion (repair/internal brace). |
| Flexor-Pronator | Tendinopathy/Strain: Rest, NSAIDs, eccentric strengthening, physical therapy, occasional PRP (controversial). | Refractory tendinopathy (6+ months non-op failure): Debridement, +/- medial epicondylectomy. Avulsion: Repair. |
| Ulnar Nerve | Mild neuropathy: Activity modification, NSAIDs, night splinting, nerve gliding. | Recalcitrant cubital tunnel syndrome (failed 3-6 months non-op), progressive motor deficits, nerve subluxation. Prophylactic transposition during UCLR. Loose body/osteophyte-induced neuropathy. |
| Other | Mild osteophyte formation without mechanical symptoms. | Symptomatic loose bodies, large osteophytes causing impingement or nerve irritation. |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is crucial for optimizing outcomes in medial elbow surgery.
Clinical Assessment
A comprehensive history should elucidate the mechanism of injury, chronicity of symptoms, precise location of pain, aggravating activities (e.g., specific phases of throwing), prior treatments, and return-to-play expectations.
Physical examination focuses on:
*
Inspection
: Swelling, ecchymosis, muscle atrophy.
*
Palpation
: Medial epicondyle, sublime tubercle, flexor-pronator mass, ulnar nerve (for tenderness, subluxation).
*
Range of Motion (ROM)
: Flexion, extension, pronation, supination. Note any deficits or pain arcs.
*
Valgus Instability Testing
:
*
Valgus Stress Test
: Performed at 30° of flexion to isolate the AB. Apply a valgus force while stabilizing the humerus. Excessive gapping or pain indicates UCL laxity.
*
Moving Valgus Stress Test
: Shoulder abducted to 90°, elbow fully flexed. Maintain valgus torque while rapidly extending the elbow to approximately 30°. A painful clunk or apprehension between 120° and 70° of flexion is highly specific for UCL injury.
*
Milking Maneuver
: Arm abducted 90°, elbow flexed 90°, forearm supinated. Examiner grasps thumb and pulls distally, applying a valgus stress. Pain on the medial elbow is indicative of UCL injury.
*
Ulnar Nerve Assessment
: Sensation in the small finger and ulnar half of the ring finger, motor strength of the intrinsic muscles (e.g., finger abduction/adduction, Froment's sign). Tinel's sign at the cubital tunnel.
Imaging Studies
- Radiographs : AP, lateral, and oblique views of the elbow are essential to rule out avulsion fractures, loose bodies, osteophytes, and physeal injuries (in adolescents). Stress radiographs (gravity or manual) can objectively quantify valgus gapping but require expertise to perform and interpret.
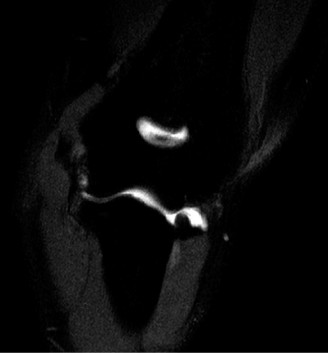
- Magnetic Resonance Imaging (MRI) : MRI, preferably with an arthrogram, is the gold standard for evaluating UCL integrity, flexor-pronator pathology, and associated intra-articular injuries (e.g., osteochondral lesions). A complete rupture will show discontinuity of the ligament, while a partial tear may show high signal intensity within the substance of the ligament. T2-weighted fat-saturated sequences are particularly useful.
- Dynamic Ultrasound : Increasingly used for real-time assessment of UCL laxity under valgus stress and to evaluate ulnar nerve dynamics during elbow flexion.
Graft Selection (for UCLR)
The most common autograft options include:
*
Palmaris Longus Tendon
: Preferred due to its low donor site morbidity, adequate length, and similar biomechanical properties to the UCL. It is absent in approximately 10-15% of individuals.
*
Gracilis Tendon
: A reliable alternative when palmaris longus is unavailable or insufficient. Requires a separate incision on the medial knee.
*
Semitendinosus Tendon
: Similar to gracilis, harvested from the medial knee.
*
Plantaris Tendon
: Less commonly used, harvested from the ankle.
Allografts are typically reserved for revision surgeries or when autograft harvest is contraindicated, but concerns exist regarding infection risk, immunogenicity, and slower incorporation.
Patient Positioning
The patient is typically positioned supine on the operating table.
* The arm is abducted to 90° on a specialized hand table, allowing full elbow flexion and extension.
* A tourniquet is applied to the proximal arm.
* The shoulder is internally rotated to present the medial aspect of the elbow clearly.
* Adequate padding is crucial at pressure points, especially the contralateral arm, head, and heels.
* The ulnar nerve path should be identified and marked to ensure it is not subjected to undue pressure or stretching.

Detailed Surgical Approach / Technique
This section will focus on Ulnar Collateral Ligament Reconstruction (UCLR) using the docking technique, which is a widely adopted and biomechanically sound procedure. Concomitant ulnar nerve management is typically performed.
1. Incision and Exposure
- Skin Incision : A curved longitudinal incision, approximately 6-8 cm in length, is made over the medial aspect of the elbow. It generally runs between the medial epicondyle and the olecranon, extending proximally towards the medial humeral epicondylar ridge and distally towards the sublime tubercle. This allows for excellent exposure of the medial epicondyle, UCL, and cubital tunnel.
- Superficial Dissection : Careful dissection through the subcutaneous tissue to identify and protect the medial antebrachial cutaneous nerve branches. These are often encountered and should be meticulously protected or localized and retracted to prevent iatrogenic injury and post-operative dysesthesia.
2. Ulnar Nerve Management
- Identification : The ulnar nerve is identified as it enters the cubital tunnel, posterior to the medial epicondyle. It is carefully mobilized from its surrounding fibrous attachments.
-
Decision for Transposition
: The decision to perform ulnar nerve transposition (subcutaneous vs. submuscular) is crucial.
- In-situ decompression (without transposition) : May be performed if there are no signs of nerve instability or severe compression, and sufficient space can be created by releasing the arcuate ligament.
- Subcutaneous Transposition : The nerve is mobilized anteriorly and left superficial to the flexor-pronator mass. This is simpler but carries a higher risk of direct nerve trauma or subluxation. It is typically secured with a fascial sling to prevent migration.
- Submuscular Transposition : The nerve is mobilized and placed deep to the flexor-pronator mass. This offers superior protection from direct trauma and often reduces recurrent subluxation. It requires detachment and reattachment of the flexor-pronator origin, which adds to surgical time and tissue dissection.
- Protection : Once mobilized, the ulnar nerve is gently retracted anteriorly or posteriorly with a vessel loop or Penrose drain, ensuring it is protected throughout the rest of the procedure.
3. Exposure of the UCL and Flexor-Pronator Mass
- Flexor-Pronator Split : The origin of the flexor-pronator mass (specifically between the pronator teres and flexor carpi radialis or between the flexor carpi radialis and palmaris longus) is identified. The fascia is incised, and the muscle belly is carefully split longitudinally and elevated off the medial epicondyle. This provides access to the underlying UCL.
- UCL Identification and Debridement : The remnants of the native UCL's anterior bundle are identified. Often, the ligament is attenuated, scarred, or frankly ruptured. Non-viable tissue is debrided to prepare a healthy bleeding bed for graft incorporation. The insertion of the anterior bundle onto the sublime tubercle is carefully identified.
4. Graft Harvest
- Palmaris Longus : If selected, a separate curvilinear incision (2-3 cm) is made on the volar aspect of the distal forearm, proximal to the wrist crease. The palmaris longus tendon is identified (superficial to the flexor digitorum superficialis and deep to the palmaris longus fascia). It is harvested by ligating and cutting proximally and distally, leaving a sufficient length (typically 15-18 cm) with sutures on each end.
- Gracilis/Semitendinosus : Harvested through a small longitudinal incision over the anteromedial aspect of the proximal tibia, distal to the knee joint. The tendons are identified and harvested with a tendon stripper.
5. Tunnel Creation (Docking Technique)
The docking technique aims to recreate the anatomical footprint of the anterior bundle.
*
Humeral Tunnel
:
* A guidewire is placed from the anterior cortex of the medial epicondyle, aiming towards the center of the native UCL origin, approximately 2-3 mm proximal and posterior to the medial epicondyle's articular edge. The wire should exit on the posterior cortex, forming an "over-the-top" or "figure-of-eight" position. This ensures the graft is placed anatomically and prevents impingement.
* Drill a 3.5 mm tunnel over the guidewire from anterior to posterior.
* A second 3.5 mm tunnel is drilled parallel to the first, approximately 1 cm distal, from anterior to posterior. These are the "docking" tunnels.
* A larger central "docking socket" (e.g., 6 mm) is drilled between the two parallel tunnels, penetrating only the superficial cortex of the medial epicondyle. This socket will receive the graft loop.
* Careful use of a nerve hook or blunt dissector is essential to protect the ulnar nerve and surrounding soft tissues during drilling.
*
Ulnar Tunnels
:
* The isometric point for the ulnar insertion is identified on the sublime tubercle, approximately 18 mm distal to the coronoid tip and 4 mm distal to the joint line. This is typically the most prominent point on the sublime tubercle.
* A guidewire is drilled from this point on the sublime tubercle, exiting on the posterior-ulnar cortex of the ulna.
* A 3.5 mm tunnel is drilled over this guidewire.
* A second 3.5 mm tunnel is drilled parallel, approximately 1 cm proximal, also exiting on the posterior-ulnar cortex. These are the "docking" tunnels on the ulna.
* A larger central "docking socket" (e.g., 6 mm) is drilled between the two parallel tunnels on the ulna, penetrating only the superficial cortex.
6. Graft Passage and Fixation
- Graft Preparation : The harvested graft is folded in half, creating a loop. Strong non-absorbable sutures are placed in the free ends.
- Passage : The looped portion of the graft is passed into the central humeral docking socket and then through the two humeral tunnels, exiting on the posterior side of the humerus.
- Ulnar Passage : The free ends of the graft are then passed from the posterior-ulnar cortex through the two ulnar tunnels and out into the central ulnar docking socket.
-
Tensioning and Fixation
:
- The elbow is brought into approximately 30-45° of flexion (the position of maximal isometricity for the anterior bundle).
- The free ends of the graft are firmly tensioned.
- While maintaining tension, the free ends are tied over the humeral and ulnar docking sockets using a strong non-absorbable suture, creating a tensioned figure-of-eight construct. The goal is to achieve firm, isometric tension without overtightening, which could lead to stiffness.
- Alternatively, interference screws or suture anchors can be used for direct fixation within the tunnels. The "internal brace" technique involves augmenting a UCL repair or reconstruction with a strong suture tape (FiberTape®) fixed with anchors, providing immediate stability and allowing faster rehabilitation.
7. Flexor-Pronator Repair & Closure
- Flexor-Pronator Reattachment : The elevated flexor-pronator mass is meticulously repaired and reapproximated over the reconstructed UCL. This provides an additional layer of protection and restores its dynamic stabilizing function.
- Ulnar Nerve Redraping : The ulnar nerve is carefully placed back into its transposed position (if performed) and ensured to be free of compression or tension.
- Layered Closure : The deep fascia, subcutaneous tissue, and skin are closed in layers. A sterile dressing and a hinged elbow brace are applied, typically locked in 90° of flexion initially to protect the repair.

Complications & Management
Despite high success rates, surgical intervention for medial elbow pathologies is not without potential complications. Anticipation and prompt management are crucial for optimal outcomes.
| Complication | Incidence | Management Strategy |
|---|---|---|
| Ulnar Nerve Neuropathy | 10-25% (transient), 1-5% (permanent) | Transient : Observation, physical therapy, NSAIDs, nerve gliding exercises. Persistent/Progressive : Nerve conduction studies/EMG. If severe or persistent, consider surgical neurolysis, potentially revision transposition. |
| Elbow Stiffness/Loss of ROM | 5-15% | Early and aggressive physical therapy, dynamic splinting. If severe and recalcitrant, consider manipulation under anesthesia or arthroscopic capsular release (anterior and/or posterior) after graft healing is secure (typically >6 months). |
| Graft Failure/Re-rupture | 2-10% | Early (<6 months) : Often due to technical error or premature return to activity. Late : Often due to recurrent high valgus stress or inadequate rehabilitation. Management involves revision UCLR, often with an allograft or a different autograft. |
| Infection | 0.5-2% | Superficial: Oral antibiotics, local wound care. Deep: Surgical debridement, intravenous antibiotics. If prosthesis involved (interference screw), consider hardware removal if infection persists. |
| Donor Site Morbidity | 5-10% | Palmaris Longus : Nerve injury (medial antebrachial cutaneous nerve leading to dysesthesia/neuroma), scar tenderness. Gracilis/Semitendinosus : Saphenous nerve injury, quadriceps weakness (rarely symptomatic), anterior knee pain. Management: Physical therapy, NSAIDs, nerve blocks/neurolysis for neuromas. |
| Hardware Irritation | 1-3% | Pain or palpable prominence over screw/suture anchor. If symptomatic after graft healing, consider elective hardware removal (typically >1 year post-op). |
| Heterotopic Ossification (HO) | Rare, but possible | Prophylaxis (NSAIDs/radiation) for high-risk patients (e.g., severe trauma, head injury). Management of symptomatic HO: Surgical excision after maturation of ossification, with continued HO prophylaxis. |
| Complex Regional Pain Syndrome (CRPS) | Rare | Aggressive multidisciplinary management: Physical therapy, pain management (nerve blocks, medication), psychological support. Early recognition is key. |
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation following UCLR is a lengthy, structured, and critically important process, typically spanning 9-12 months for return to competitive throwing. The goals are to protect the healing graft, restore ROM and strength, and gradually return to sport-specific activities.
Phase I: Maximum Protection (Weeks 0-6)
- Goals : Protect the graft, minimize pain and swelling, initiate gentle ROM.
- Bracing : Hinged elbow brace locked at 90° flexion for 1 week, then gradually extended to 30° flexion by week 2, and 0° extension by week 4-6. Valgus stress is strictly avoided.
- ROM : Passive elbow flexion/extension (within brace limits), active wrist and hand ROM. Forearm pronation/supination can begin gently.
- Strengthening : Isometric wrist flexion/extension, grip strengthening.
- Activity : No lifting >1 lb. No active elbow flexion against resistance.
Phase II: Moderate Protection (Weeks 6-12)
- Goals : Full active ROM, restore basic strength, begin kinetic chain exercises.
- Bracing : Brace removed for hygiene and exercises, but worn for protection. Discontinued by week 10-12 if appropriate.
- ROM : Progress to full active elbow flexion/extension and forearm rotation.
-
Strengthening
:
- Elbow : Gentle active-assisted and active elbow flexion/extension without resistance, then light resistance (e.g., Theraband).
- Wrist/Forearm : Progressive strengthening.
- Shoulder/Scapula : Essential for kinetic chain stability. Rotator cuff strengthening (isometrics to light resistance), scapular stabilization exercises.
- Core : Core strengthening.
- Activities : Light cardio. Avoid valgus stress. No throwing.
Phase III: Intermediate Strengthening (Months 3-5)
- Goals : Restore full strength and endurance, prepare for sport-specific training.
- Bracing : Typically discontinued.
-
Strengthening
:
- Elbow : Progressive resistance exercises for elbow flexors/extensors, pronators/supinators.
- Full Kinetic Chain : Emphasis on power and endurance for the shoulder, scapula, core, and lower extremities. Plyometric exercises (e.g., medicine ball throws).
- Proprioception : Balance and agility exercises.
- Activity : Continued cardio. Initiation of light sport-specific drills that do not involve throwing mechanics.
Phase IV: Return to Throwing (Months 5-9)
- Goals : Gradual, progressive return to throwing mechanics and sport-specific loads.
- Criteria for entry : Full pain-free ROM, symmetrical strength (isokinetic testing often used), no residual tenderness.
-
Interval Throwing Program (ITP)
: A highly structured, progressive program that gradually increases throwing distance, velocity, and intensity.
- Phase 1 (Flat Ground) : Focus on mechanics, short distances, light effort.
- Phase 2 (Mound/Increased Velocity) : Gradually increase intensity and introduce breaking pitches (later).
- Monitoring : Close monitoring for pain, fatigue, and mechanical flaws. Biomechanical analysis may be performed.
- Pitch Count Guidelines : Strict adherence to age-appropriate and post-surgical pitch count and rest guidelines.
Phase V: Return to Competition (Months 9-12+)
- Goals : Full return to competitive sport.
- Criteria for entry : Completion of ITP without symptoms, sustained pain-free throwing at competitive velocities, psychological readiness.
- Transition : Gradual integration into team practice and competitive games. Continued monitoring of arm health.
- Maintenance : Lifelong emphasis on proper throwing mechanics, strength and conditioning, and appropriate rest.
Summary of Key Literature / Guidelines
The landscape of medial elbow injury management in overhead athletes has evolved considerably, driven by extensive research and clinical experience. Key insights and guidelines include:
- UCLR Success Rates : Modern UCLR techniques consistently report return-to-sport rates in high-level athletes ranging from 75% to 90%, with excellent or good outcomes in over 85% of cases. Professional baseball pitchers typically demonstrate high rates of return to previous or higher levels of competition.
- Factors Influencing Outcomes : Several factors correlate with successful outcomes, including younger age at surgery, higher pre-injury level of competition, compliance with rehabilitation, and absence of prior revision surgery. Concomitant intra-articular pathology (e.g., osteochondral lesions, posterior impingement) can negatively impact recovery.
- Internal Brace Augmentation : The internal brace technique, which uses a high-strength suture tape augmentation for UCL repair or reconstruction, has gained significant traction. Preliminary studies suggest it may allow for an accelerated rehabilitation protocol and potentially earlier return to sport, particularly for acute avulsion injuries, by providing immediate robust stabilization. Long-term comparative data with traditional reconstruction are still accumulating.
- Biomechanical Analysis : The importance of detailed biomechanical analysis of the throwing motion is increasingly recognized. Identifying and correcting faulty mechanics (e.g., increased valgus moment, excessive shoulder external rotation, delayed trunk rotation) can reduce stress on the elbow and prevent re-injury.
- Ulnar Nerve Transposition : While often performed prophylactically or therapeutically, studies indicate a non-negligible incidence of post-operative ulnar nerve morbidity (neuropathy, dysesthesia) even after successful transposition. Careful dissection and tension-free placement are paramount.
- Youth Athlete Considerations : The management of medial elbow pain in skeletally immature athletes differs, with a strong emphasis on non-operative management for medial epicondylar apophysitis. However, significant apophyseal avulsion fractures may require surgical fixation. The presence of chronic UCL insufficiency in a young athlete should prompt careful consideration, as early surgical intervention may be appropriate in high-level throwers to preserve their athletic careers.
-
Prevention Strategies
: Emphasis on prevention includes:
- Pitch Count and Rest Guidelines : Adherence to guidelines from organizations like USA Baseball and Little League regarding maximum pitches per game/week and mandatory rest periods.
- Avoiding Specialization : Encouraging participation in multiple sports and delaying single-sport specialization until late adolescence.
- Proper Mechanics : Early instruction in efficient and safe throwing mechanics.
- Strength and Conditioning : Comprehensive full-body conditioning, including core stability, shoulder strength, and hip drive, to optimize the kinetic chain.
- Future Directions : Ongoing research focuses on biologic augmentation (e.g., PRP, bone marrow aspirate concentrate) for UCL tears and repairs, further refinement of surgical techniques, and development of predictive models for injury risk and return to sport. The role of dynamic ultrasound in both diagnosis and post-operative assessment is also expanding.
