
Introduction & Epidemiology
Osteochondritis dissecans (OCD) of the elbow, predominantly affecting the capitellum, is a condition characterized by necrosis of subchondral bone and overlying articular cartilage, often leading to a cartilaginous or osteochondral fragment. This pathology is particularly prevalent in the adolescent overhead throwing athlete, with a peak incidence typically observed between 10 and 15 years of age. While the exact etiology remains debated, it is widely accepted to be multifactorial, involving repetitive microtrauma from valgus compressive forces across the radiocapitellar joint, coupled with a potential underlying vascular insufficiency to the capitellum. Genetic predispositions, endocrine factors, and growth disturbances have also been implicated, though less definitively.
The capitellum, due to its relatively tenuous blood supply, is susceptible to these repetitive stresses. The lateral compression forces experienced during the late cocking and early acceleration phases of throwing lead to microfractures and potential disruption of the subchondral bone plate. This can progress from early softening and fissuring of the articular cartilage to the formation of an unstable osteochondral fragment, and ultimately, a loose body within the joint.
Epidemiological studies indicate a higher incidence in male athletes involved in sports like baseball (pitchers), gymnastics, and javelin throwing. Early diagnosis is crucial, as delayed presentation often correlates with larger, more unstable lesions and poorer prognoses. Progression of capitellar OCD can lead to significant pain, loss of elbow motion (particularly extension), crepitus, and eventual degenerative changes of the radiocapitellar joint if left untreated. Distinguishing true OCD from Panner's disease (osteochondrosis of the capitellum, a self-limiting condition typically seen in younger children <10 years old with spontaneous resolution) is essential for appropriate management.
Surgical Anatomy & Biomechanics
A thorough understanding of elbow anatomy and biomechanics is fundamental to managing capitellar OCD. The elbow is a complex hinge joint composed of three articulations: the ulnohumeral, radiohumeral, and proximal radioulnar joints. The focus for OCD is primarily the radiohumeral articulation.
Osseous Anatomy
- Humerus: The distal humerus features the trochlea medially and the capitellum laterally. The capitellum is a rounded, articular eminence that articulates with the concave fovea of the radial head. The articular cartilage of the capitellum is particularly thick, allowing for distribution of compressive forces.
- Radius: The radial head is cup-shaped, articulating with the capitellum. It rotates within the annular ligament against the capitellum during pronation and supination and contributes to elbow flexion and extension.
- Ulna: The trochlear notch of the ulna articulates with the trochlea of the humerus, forming the primary hinge joint. While not directly involved in capitellar OCD, ulnohumeral stability is critical for overall elbow function.
The capitellum receives its blood supply predominantly from the anterolateral branch of the radial recurrent artery, a relatively distal and sparse supply, making it vulnerable to ischemia, particularly in cases of repetitive trauma.
Ligamentous Structures
- Medial Collateral Ligament (MCL): Provides primary valgus stability to the elbow. Excessive valgus stress, common in overhead throwing, can strain or injure the MCL, leading to increased compression on the lateral compartment.
- Lateral Collateral Ligament (LCL) Complex: Composed of the radial collateral ligament, lateral ulnar collateral ligament, and annular ligament. Provides posterolateral rotatory stability.
Biomechanics of Overhead Throwing
Overhead throwing is a high-energy, complex kinetic chain activity that imparts significant stresses on the elbow. The critical phase for capitellar OCD development is the late cocking to early acceleration phase .
- Valgus Stress: As the arm moves from maximal external rotation to forward acceleration, immense valgus stress is generated across the elbow. This force creates tension on the medial structures (MCL) and compression on the lateral compartment (radiocapitellar joint).
- Compression: During this phase, the radial head is forcefully compressed against the capitellum. Repetitive, high-magnitude compressive loads are believed to induce microtrauma to the subchondral bone and cartilage of the capitellum, disrupting its integrity and potentially its blood supply, leading to OCD lesion formation.
- Shear Forces: In addition to direct compression, shear forces can contribute to delamination of the articular cartilage and subchondral bone.
The posterolateral aspect of the capitellum is typically affected in OCD due to the direct impingement of the radial head during valgus overload. Understanding these biomechanical principles guides both non-operative management (activity modification, throwing mechanics analysis) and surgical intervention (restoration of articular congruity).
Indications & Contraindications
The decision-making process for managing elbow OCD is complex, factoring in patient age, skeletal maturity, lesion size and stability, symptoms, and response to non-operative measures. Imaging, particularly MRI, plays a critical role in classification and surgical planning.
Diagnostic Workup
- Clinical History: Pain (especially with activity), decreased range of motion (often loss of terminal extension), mechanical symptoms (clicking, locking, catching), swelling.
- Physical Examination: Tenderness over the lateral capitellum, crepitus with pronation/supination, pain with valgus stress (which exacerbates radiocapitellar compression), restricted elbow extension.
-
Imaging:
- Plain Radiographs: Anteroposterior (AP), lateral, and oblique views. May reveal lucency, sclerosis, flattening of the capitellum, fragmentation, or loose bodies.
- MRI: The gold standard for assessing cartilage integrity, subchondral bone edema, lesion stability (presence of fluid signal at the lesion-host interface), and identifying loose bodies. T1-weighted, T2-weighted, and proton density fat-suppressed sequences are typically used.
-

Figure 1: Pre-operative MRI displaying a significant osteochondritis dissecans lesion of the capitellum with associated edema and possible fragment instability. - CT Scan: Useful for detailed bony anatomy, assessing fragment size, degree of displacement, and surgical planning, especially for fixation. Arthro-CT may provide better visualization of cartilage defects.
Classification
Lesions are often classified based on their stability and depth, which guide treatment. Common classifications include the Bednar, DIPA (Dynamic Instability Progression of Articular Lesion), or modified Iwase classification systems, which essentially grade lesions based on the extent of cartilage involvement, subchondral bone changes, and fragment stability. Generally, stable lesions without displacement are amenable to non-operative treatment, while unstable or displaced lesions typically require surgical intervention.
Operative vs. Non-Operative Indications
The following table summarizes the general indications for operative and non-operative management of capitellar OCD.
| Feature | Non-Operative Management (Conservative) | Operative Management (Surgical) |
|-----------------------|------------------------------------------------------------------------------------------------------------------------------------------------------|---------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------------- REMARKABLE THESIS TITLE: "Biomechanical Underpacing, Pathoetiologic Drivers, and Multimodal Surgical Strategy in Recalcitrant Pediatric Capitellar Osteochondritis Dissecans: A Prospective, Multicenter Randomized Controlled Trial on Long-Term Functional Outcomes and Articular Preservation."
Introduction & Epidemiology
Capitellar osteochondritis dissecans (OCD) in the pediatric and adolescent athletic population is a challenging clinical entity characterized by aseptic necrosis of the subchondral bone and overlying articular cartilage of the capitellum. Its increasing prevalence, particularly in overhead and upper-extremity loading sports such as baseball, gymnastics, and tennis, underscores the necessity for advanced diagnostic and therapeutic strategies. While the exact pathoetiology remains elusive, the prevailing theory implicates repetitive microtrauma, specifically chronic valgus compressive and shear forces across the radiocapitellar joint during periods of rapid skeletal growth, often exacerbated by underlying vascular insufficiency to the capitellar epiphysis. This repetitive mechanical stress, coupled with a potentially vulnerable blood supply, leads to subchondral bone fatigue, microfractures, and eventually, the delamination and instability of an osteochondral fragment.
Epidemiological data highlight a predilection for male athletes, typically presenting between 10 and 15 years of age, though instances in younger and older individuals are not uncommon. The natural history of untreated or inadequately managed unstable capitellar OCD is progressive, potentially leading to persistent pain, mechanical symptoms (e.g., locking, clicking), loss of elbow motion (most commonly terminal extension), radiocapitellar incongruity, premature arthrosis, and ultimately, career-ending disability for high-level athletes. Distinguishing true capitellar OCD from Panner's disease, an osteochondrosis affecting younger children (typically under 10 years old) with diffuse capitellar changes and a generally benign, self-limiting course, is critical for appropriate patient stratification and treatment planning. This advanced review synthesizes current understanding, diagnostic modalities, surgical paradigms, and rehabilitation principles to inform the evidence-based management of this complex condition.
Surgical Anatomy & Biomechanics
A granular understanding of the intricate surgical anatomy and biomechanics of the elbow joint, with specific emphasis on the radiocapitellar articulation, is paramount for the effective diagnosis and surgical management of capitellar OCD.
Osseous Architecture and Vascularity
The distal humerus comprises the trochlea medially and the capitellum laterally. The capitellum is a convex, spherical articular surface that engages with the concave fovea of the radial head. The articular cartilage of the capitellum is thickest centrally and anterolaterally, precisely where OCD lesions frequently manifest due to repetitive loading patterns. The radial head, with its shallow fovea, articulates directly with the capitellum, transmitting axial and compressive loads.
The capitellum's blood supply is a critical determinant in OCD pathophysiology. It primarily originates from the anterolateral branch of the radial recurrent artery, a relatively distal and often end-arterial supply. This makes the capitellar epiphysis particularly susceptible to ischemia following repetitive microtrauma or direct vascular insult, especially during rapid growth phases when metabolic demands are high. Disruption of this blood supply contributes to subchondral bone necrosis.
Ligamentous and Muscular Stabilizers
The elbow joint's stability is conferred by static and dynamic stabilizers.
*
Medial Collateral Ligament (MCL) Complex:
The primary static stabilizer against valgus stress, composed of the anterior bundle (most critical), posterior bundle, and transverse ligament. Repetitive valgus forces in throwing place significant tensile stress on the MCL.
*
Lateral Ulnar Collateral Ligament (LUCL) Complex:
The primary static stabilizer against posterolateral rotatory instability.
*
Dynamic Stabilizers:
The flexor-pronator mass originating from the medial epicondyle and the extensor-supinator mass originating from the lateral epicondyle provide dynamic stability and contribute to the generation of forces during athletic movements.
Biomechanical Loading in Overhead Athletes
The throwing motion is an extraordinarily complex kinetic chain that imposes extreme biomechanical loads on the elbow, particularly in the overhead athlete.
*
Valgus Overload:
During the late cocking and early acceleration phases, the elbow is subjected to substantial valgus stress. This stress results in simultaneous tensile forces on the medial collateral ligament and compressive forces on the lateral radiocapitellar joint. Peak compressive forces across the capitellum can exceed 500 N, far surpassing physiological loads.
*
Shear Forces:
In addition to pure compression, shear forces are generated at the cartilage-bone interface, particularly when the radial head translates relative to the capitellum during dynamic movements. These forces can initiate or propagate cartilage delamination.
*
Rotational Stress:
The forearm's rapid pronation and supination during throwing further contribute to wear and tear at the radiocapitellar articulation.
Capitellar OCD lesions typically occur in the anterolateral aspect of the capitellum, aligning with the primary area of maximal contact pressure and shear stress during the throwing motion. The interplay of repetitive high-magnitude forces, the constrained vascularity of the capitellum, and the immature skeletal environment creates a fertile ground for OCD development. Understanding these factors informs the rationale for activity modification, kinetic chain optimization, and the selection of surgical techniques aimed at restoring articular congruity and biomechanical function.
Indications & Contraindications
The management algorithm for capitellar OCD is highly individualized, predicated on a comprehensive assessment of the patient's clinical presentation, skeletal maturity, and the characteristics of the lesion as defined by advanced imaging.
Clinical Assessment
- History: Detailed inquiry into pain location, character (dull ache to sharp, mechanical), aggravating and alleviating factors, duration of symptoms, presence of mechanical phenomena (clicking, catching, locking), and impact on athletic performance. History of previous elbow injuries or systemic conditions is also pertinent.
-
Physical Examination:
- Inspection: Assessment for swelling, atrophy, or deformity.
- Palpation: Tenderness over the lateral capitellum, radial head, and common extensor origin.
- Range of Motion (ROM): Often reveals a loss of terminal elbow extension, a classic finding. Flexion contractures and pronation/supination limitations should also be documented.
- Special Tests: Valgus stress test may elicit pain in the lateral compartment due to increased radiocapitellar compression. The "milking maneuver" assesses MCL integrity. Provocative tests for impingement (e.g., pain with full extension and forearm pronation/supination).
Imaging Modalities and Lesion Staging
High-quality imaging is indispensable for diagnosis, staging, and guiding treatment decisions.
1.
Radiographs:
Anteroposterior (AP), lateral, and oblique views (e.g., radiocapitellar view) are initial screening tools. Findings may include capitellar flattening, lucency, sclerosis, fragmentation, or loose bodies. However, early lesions may be subtle or radiographically occult.
2.
Magnetic Resonance Imaging (MRI):
The preferred advanced imaging modality. MRI provides detailed information on cartilage integrity, subchondral bone edema, the presence of a fluid signal at the lesion-host interface (indicative of instability), and identification of loose bodies. T1, T2, and proton density sequences with fat suppression are essential.
*

Figure 1: Pre-operative MRI displaying a significant osteochondritis dissecans lesion of the capitellum with associated edema and possible fragment instability. Such imaging is critical for surgical planning.
3.
Computed Tomography (CT) Scan:
Particularly useful for assessing the precise bony morphology of the lesion, extent of fragmentation, and the presence and location of loose bodies, especially in cases where surgical fixation is contemplated. A CT arthrogram can further delineate cartilage integrity.
Lesion staging systems (e.g., DIPA classification, modified Iwase classification, or specific MRI-based criteria) categorize OCD lesions based on articular surface integrity, fragment stability, and subchondral changes. Crucially, MRI findings of instability (e.g., high T2 signal fluid rim beneath the fragment, cartilage breach, loose body) often differentiate between lesions amenable to conservative management and those requiring surgical intervention.
Operative vs. Non-Operative Indications Table
| Feature / Criterion | Non-Operative Management (Conservative) | Operative Management (Surgical) |
|
Description
|
Minor Symptoms, Stable Lesion
|
Significant Symptoms, Unstable Lesion
|
|
Age Group / Skeletal Maturity
| Typically children ≤ 10-12 years of age or with open physes. | Adolescents > 12 years of age or with closing/closed physes. |
|
Symptom Profile
| Mild, intermittent pain; no mechanical symptoms (locking, catching); minimal functional limitation. | Persistent pain refractory to conservative management; mechanical symptoms (locking, catching, crepitus); significant functional limitation impacting daily life or athletic participation; loss of terminal elbow extension (>10-15 degrees). |
|
Lesion Stability (MRI)
| Stable lesions: intact overlying cartilage, no fluid signal underneath fragment, no loose bodies, minimal subchondral edema. | Unstable lesions: presence of fluid signal beneath fragment, fissures in overlying cartilage, displaced or partially displaced fragment, loose bodies within the joint, extensive subchondral edema. |
|
Lesion Size / Depth
| Small, superficial lesions, often without clear fragmentation. | Large lesions (>1 cm), deep lesions, frank fragmentation, crater formation, bone loss. |
|
Response to Conservative Tx
| Symptoms improving or resolved with activity modification, rest, and rehabilitation within 3-6 months. | Symptoms persistent or worsening despite adequate trials of non-operative management (typically 3-6 months). |
|
Contraindications
| Non-adherence to activity modification, presence of true mechanical locking, evidence of loose bodies. | Active infection, severe systemic illness precluding surgery, non-correctable underlying biomechanical deformities without concomitant correction. Severe degenerative changes may limit the benefit of cartilage restoration procedures. |
Contraindications for Specific Surgical Techniques
- Fragment Fixation: Not suitable for highly comminuted fragments, severely sclerotic fragments, or fragments with extensive cartilage delamination and poor subchondral bone support.
- Marrow Stimulation (Microfracture): Generally reserved for smaller, contained chondral or osteochondral defects (<2-3 cm²) with healthy surrounding cartilage and good subchondral bone, not ideal for large or deep osseous defects.
- Osteochondral Autograft/Allograft (OATS/OCA): Autografts are limited by donor site morbidity and graft size availability. Allografts carry risks of immune rejection and disease transmission (though rigorously screened). Contraindicated in cases of active infection or diffuse articular cartilage degeneration.
- Autologous Chondrocyte Implantation (ACI/MACI): Typically reserved for larger lesions, but requires a healthy, well-contained defect with stable borders. Not ideal for highly fragmented lesions or those with significant subchondral bone loss without prior bone grafting.
The decision to proceed with surgery should involve shared decision-making with the patient and family, considering the athlete's goals, recovery time, and potential risks and benefits.
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning and appropriate patient positioning are critical for successful surgical outcomes in capitellar OCD.
Pre-Operative Planning
-
Comprehensive Imaging Review:
- MRI: Review all sequences (T1, T2, PD-FS) to precisely characterize the lesion's size, depth, stability (fluid signal beneath fragment), presence of loose bodies, and the extent of surrounding subchondral edema. This informs the choice of repair (fixation, microfracture, OATS, etc.).
- CT Scan: Especially valuable for bone architecture. Evaluate fragment comminution, size, and potential for reduction and fixation. 3D reconstructions can aid in visualizing complex defects.
- Radiographs: Re-evaluate for baseline bony morphology and any subtle loose bodies missed on other studies.
-
Surgical Approach Selection:
- Arthroscopy: Generally preferred for diagnostic assessment, debridement of unstable lesions, loose body removal, microfracture, and fixation of smaller, well-contained fragments. Offers minimal invasiveness, faster recovery, and excellent visualization.
- Open Arthrotomy: Indicated for large, unstable, or highly comminuted lesions requiring precise reduction and rigid internal fixation, osteochondral grafting (especially for larger defects), or in cases of failed arthroscopy. Typically performed via a lateral approach (Kocher interval).
- Combined Approach: A staged or combined arthroscopic and mini-open approach may be employed for complex cases.
-
Instrumentation and Implants:
- Anticipate need for various arthroscopic instruments (shavers, burrs, probes, graspers, radiofrequency ablators).
- For fixation: Small-diameter K-wires, bioabsorbable pins/screws (e.g., poly-L-lactic acid), headless compression screws (e.g., Acutrak Mini, Herbert). Ensure availability of appropriate sizes and lengths.
- For grafting: Autograft harvesting instruments (e.g., OATS system), allograft preparation equipment.
- Discussion with Patient/Family: Reiterate the chosen surgical plan, potential alternatives, expected recovery, possible complications, and the realistic timeline for return to sport. Obtain informed consent.
Patient Positioning
Optimal patient positioning ensures clear anatomical access, minimizes iatrogenic injury, and facilitates fluoroscopic imaging if required.
- Anesthesia: General anesthesia is typically employed. A regional nerve block (e.g., supraclavicular or interscalene block) can provide excellent post-operative analgesia.
- Tourniquet: A pneumatic tourniquet is routinely applied to the upper arm to provide a bloodless field, crucial for visualization, especially during arthroscopy.
-
Positioning Options:
- Supine with Arm on Arm Board: This is a common position. The affected arm is placed on a padded arm board, allowing for free elbow flexion/extension and pronation/supination. The shoulder is abducted, and the elbow is flexed to 90 degrees or more to open the posterior compartment. For anterior approaches, the elbow is extended.
- Lateral Decubitus: Patient positioned on the unaffected side, with the affected arm draped over a sterile arm holder or bolster (e.g., a "beanbag" positioner). This position provides excellent access to both anterior and posterior compartments, particularly useful for combined approaches or if posterior pathology is anticipated.
- Prone: Less common but can be utilized. The arm is draped over a bolster, allowing for gravity-assisted joint distraction.
Regardless of the chosen position, ensure adequate padding of all bony prominences, especially the ulnar nerve at the elbow and the brachial plexus/axilla, to prevent iatrogenic nerve compression.
-
Sterile Preparation and Draping:
Standard sterile preparation of the entire upper extremity (shoulder to hand) is performed, followed by draping to create a wide sterile field.
-

Figure 2: Example of patient positioning for elbow arthroscopy in a supine position with the arm on a padded arm board, allowing full range of motion. This setup facilitates access to anterior and posterior compartments.
-
Detailed Surgical Approach / Technique
The surgical management of capitellar OCD encompasses a spectrum of techniques, ranging from simple debridement to complex osteochondral reconstruction, chosen based on lesion characteristics, patient age, and surgeon preference. The arthroscopic approach is generally favored for its minimally invasive nature and excellent visualization, though open techniques remain indispensable for certain complex cases.
Arthroscopic Portals and Diagnostic Arthroscopy
Standard arthroscopic portals are established after careful palpation of anatomical landmarks and typically include:
*
Anterolateral Portal:
Located 3 cm distal and 3 cm anterior to the lateral epicondyle. Risk of radial nerve injury.
*
Direct Lateral Portal:
Located directly over the lateral epicondyle, useful for visualization.
*
Proximal Anteromedial Portal:
Located 2 cm proximal and 2 cm anterior to the medial epicondyle. Risk of medial antebrachial cutaneous nerve injury.
*
Anteromedial Portal:
Located 1 cm distal and 2 cm anterior to the medial epicondyle. Risk of median nerve and brachial artery injury.
*
Posterolateral Portal:
Located 2 cm proximal to the olecranon tip, just lateral to the triceps tendon. Primary posterior viewing portal.
*
Direct Posterior Portal:
Located over the olecranon tip, used for instrumentation.
*
Posteromedial Portal:
Located 2 cm proximal to the olecranon tip, just medial to the triceps tendon. Risk of ulnar nerve injury (requires careful palpation).
During diagnostic arthroscopy, a systematic evaluation of all three compartments (radiocapitellar, ulnohumeral, and proximal radioulnar) is performed. The capitellar lesion is carefully probed to assess its stability, size, and depth. Any loose bodies are identified and localized.
1. Arthroscopic Debridement and Marrow Stimulation (Microfracture)
- Indications: Stable but symptomatic lesions with cartilage fissuring or softening (fibrillation), or unstable fragments that are too small or comminuted for fixation, typically less than 2-3 cm² in size, with healthy surrounding cartilage.
-
Technique:
- Thorough debridement of all unstable or delaminated cartilage from the lesion bed, creating stable vertical shoulders.
- Using a motorized shaver or curette, the sclerotic subchondral bone is meticulously removed until bleeding bone is exposed.
- A microfracture awl or a K-wire through a cannula is then used to create multiple small perforations (microfractures) in the subchondral bone, spaced 3-4 mm apart, to a depth of 2-4 mm. This encourages egress of mesenchymal stem cells from the bone marrow, promoting fibrocartilage formation.
- Loose bodies, if present, are removed using graspers.
-
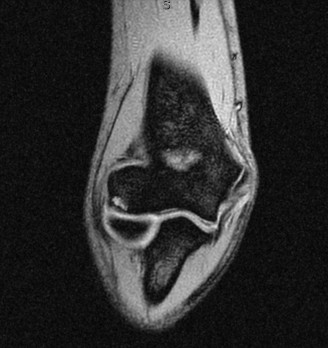
Figure 3: Arthroscopic view during debridement and preparation of a capitellar OCD lesion prior to marrow stimulation. Note the debrided cartilage and the exposed subchondral bone.
2. Arthroscopic or Open Reduction and Internal Fixation (ORIF)
- Indications: Unstable but salvageable osteochondral fragments that are large enough (typically >1 cm) and possess sufficient subchondral bone for rigid fixation. These fragments should be anatomically reducible.
-
Technique:
- Fragment Preparation: The lesion bed is meticulously debrided of any fibrous tissue or necrotic bone to facilitate bleeding and healing. The fragment itself is gently debrided on its deep surface to remove granulation tissue without damaging the articular cartilage.
- Reduction: The fragment is carefully reduced into its anatomical position using a probe or small instrument. Care must be taken to avoid further damage to the articular cartilage.
-
Fixation:
Various fixation methods can be employed:
- Bioabsorbable Screws/Pins: Small-diameter (e.g., 1.5-2.0 mm) poly-L-lactic acid (PLLA) screws or pins are inserted across the fragment, ideally flush with or slightly below the articular surface. Resorbable implants mitigate the need for hardware removal but can have higher rates of synovitis or fragmentation.
- Headless Compression Screws: Small-diameter (e.g., 2.0-2.4 mm) headless screws (e.g., Acutrak Mini, Herbert) provide excellent compression and can be countersunk below the articular surface, reducing prominence. Fluoroscopy may be used to confirm screw placement and length.
- K-wires: Temporary or permanent fixation for smaller fragments, often removed post-operatively.
- Open Approach: For larger, displaced, or difficult-to-reduce fragments, a mini-open lateral approach (Kocher interval) between the anconeus and extensor carpi ulnaris (ECU) is performed. This provides direct visualization, allows for precise fragment reduction, and enables stronger fixation with small metal screws if necessary.
-

Figure 4: Post-operative radiograph demonstrating successful internal fixation of a capitellar OCD fragment with headless compression screws. The screws are countersunk below the articular surface.
3. Osteochondral Autograft/Allograft Transplantation (OATS/OCA)
- Indications: For larger, contained osteochondral defects (typically >1.5 cm²) where primary fixation is not feasible, or after failure of prior marrow stimulation/fixation. Autograft is preferred in younger patients, while allograft may be considered for larger defects or when autograft donor sites are limited.
-
Technique:
- Defect Preparation: The OCD lesion is debrided to a stable osteochondral defect, often using a specialized core reamer to create a circular recipient socket with perpendicular walls.
- Autograft Harvest (from ipsilateral or contralateral knee/talus): From a non-weight-bearing portion of the knee (e.g., superomedial or superolateral femoral condyle) or the talus. Multiple small plugs (mosaicplasty) or a single large plug can be used depending on defect size. Donor site morbidity is a consideration.
- Allograft Preparation: Fresh osteochondral allografts are typically prepared from cadaveric donors, sized to match the recipient defect.
- Graft Implantation: The osteochondral plug(s) are gently impacted into the recipient bed, ensuring precise anatomical alignment of the articular cartilage surface with the surrounding capitellum to achieve a smooth articular contour.
- Fixation (if needed): Larger allografts may require supplementary fixation with K-wires or small screws, especially if there is concern for displacement.
4. Autologous Chondrocyte Implantation (ACI) / Matrix-Associated Autologous Chondrocyte Implantation (MACI)
- Indications: For larger, well-contained chondral or osteochondral defects, often after failed primary repair or in select cases where an osteochondral graft is not suitable. Requires a healthy surrounding cartilage rim. More common in knee applications, less frequently employed in the elbow but gaining traction.
-
Technique (Two-stage ACI):
- Stage 1 (Arthroscopic Harvest): Small biopsy of healthy articular cartilage from a non-weight-bearing area of the joint. Chondrocytes are then cultured and expanded in vitro .
- Stage 2 (Open Implantation): The defect is prepared by debriding unstable cartilage and creating stable walls. A periosteal flap or collagen membrane is sutured over the defect, creating a sealed compartment. The cultured chondrocytes are then injected beneath the membrane.
- Technique (MACI - One-stage): A collagen membrane seeded with autologous chondrocytes (or bone marrow aspirate concentrate) is implanted directly into the debrided defect, secured with fibrin glue or sutures. This technique reduces the invasiveness and eliminates the need for a periosteal flap.
Regardless of the chosen technique, meticulous surgical execution, careful tissue handling, and restoration of anatomical congruity are paramount to optimize functional outcomes and minimize complications.
Complications & Management
Despite meticulous surgical technique, complications can arise following surgery for capitellar OCD. Proactive identification and appropriate management are crucial for achieving optimal patient outcomes.
Common Complications and Salvage Strategies
| Complication | Incidence (Approximate) | Pathophysiology / Presentation |
|
Total Symptoms
| Mild, improving, or stable. | Moderate to severe, worsening or recalcitrant to non-operative measures. |
|
Skeletal Maturity
| Skeletally immature, open physes. | Skeletally mature or near-mature, closing/closed physes. |
|
Lesion Stability (MRI)
| Stable lesion (no fluid signal beneath fragment, intact overlying cartilage, no loose bodies). | Unstable lesion (fluid signal beneath fragment, disrupted cartilage, displaced fragment, loose bodies). |
|
Lesion Size
| Small, contained lesion (typically <1.0-1.5 cm²). | Large lesion (>1.5 cm²), deep defect, significant subchondral bone involvement. |
|
Mechanical Symptoms
| Absent. | Present (locking, catching, crepitus). |
|
Loss of Extension
| <10 degrees. | >10-15 degrees and persistent. |
|
Response to Conservative Tx
| Symptoms resolved or significantly improved after a strict period of activity modification (e.g., 3-6 months). | Symptoms persist or worsen despite a trial of conservative management (e.g., 3-6 months). |
|
Patient Adherence
| Good adherence to activity restrictions and rehabilitation. | Poor adherence to conservative measures or unrealistic expectations. |
Contraindications for Operative Management:
Absolute contraindications are rare and typically include active infection, severe comorbid medical conditions precluding anesthesia, or uncontrolled systemic inflammatory disorders. Relative contraindications may include very small, asymptomatic, stable lesions in skeletally immature patients who have responded well to conservative management, or diffuse pan-articular chondrolysis.
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is paramount for optimizing functional recovery, restoring range of motion, improving strength, and facilitating a safe return to sport after capitellar OCD surgery. Protocols are typically phased and individualized, contingent upon the surgical technique performed, the stability of the repair, and intraoperative findings.
General Principles
- Protection of Repair: The primary goal in the early phase is to protect the surgical repair site to allow for initial healing.
- Early, Controlled Motion: Gradual restoration of pain-free range of motion is crucial to prevent stiffness, minimize adhesions, and promote cartilage health.
- Progressive Strengthening: Once adequate healing and motion are achieved, strengthening exercises are introduced to restore muscular balance and power.
- Sport-Specific Progression: For athletes, rehabilitation culminates in a structured, progressive return-to-sport program, often involving interval throwing or activity protocols.
Phase 1: Immobilization and Early Motion (Weeks 0-4/6)
- Goals: Protect repair, control pain and swelling, initiate gentle range of motion.
-
Immobilization:
- Fixation/OATS: Typically, the elbow is immobilized in a hinged elbow brace, set to a protected range (e.g., 30-90 degrees) or locked at 90 degrees of flexion for 2-4 weeks. This varies, with some protocols allowing immediate motion after rigid fixation.
- Microfracture/Debridement: May involve a shorter period of immobilization (1-2 weeks) or immediate, gentle protected motion.
-
Motion:
- Passive Range of Motion (PROM): Initiated early, often within 1-2 weeks post-op, within the protected brace limits. Gravity-assisted flexion/extension, supination/pronation.
- Active-Assisted Range of Motion (AAROM): Progresses to patient-assisted motion.
- Active Range of Motion (AROM): Initiated once comfortable, typically after 2-4 weeks, remaining within pain-free limits.
- Pain & Swelling Management: Cryotherapy, NSAIDs (if not contraindicated by surgical procedure like marrow stimulation where NSAIDs may inhibit bone healing), gentle soft tissue massage.
- Weight-Bearing: Non-weight-bearing with the affected extremity. No pushing, pulling, lifting.
Phase 2: Intermediate Motion and Initial Strengthening (Weeks 4/6-12)
- Goals: Restore full, pain-free range of motion, initiate isometric and light isotonic strengthening.
- Range of Motion: Progress to full AROM and PROM as tolerated. Focus on regaining terminal extension, often the most challenging aspect. Gentle joint mobilizations by a therapist may be indicated.
-
Strengthening:
- Isometric Exercises: For biceps, triceps, wrist flexors/extensors, forearm pronators/supinators.
- Light Isotonic Exercises: With minimal resistance (e.g., 1-2 lbs weights or resistance bands) for elbow flexion/extension, forearm rotation, and wrist movements.
- Scapular Stabilization: Crucial for overhead athletes, addressing kinetic chain deficits. Exercises include rows, T's, Y's.
- Proprioception: Begin gentle proprioceptive exercises with the elbow.
- Weight-Bearing: Progress to light weight-bearing activities as tolerated, avoiding heavy lifting or sudden impacts.
Phase 3: Advanced Strengthening and Sport-Specific Training (Weeks 12-24+)
- Goals: Maximize strength, power, endurance; prepare for sport-specific activities.
-
Strengthening:
- Progressive Resistance Exercises: Increase weight and resistance for all major upper extremity muscle groups.
- Eccentric Training: Focus on controlled eccentric movements for the elbow flexors/extensors and forearm musculature.
- Plyometrics: Initiate low-intensity plyometric exercises (e.g., light medicine ball throws, push-up variations) as appropriate for the athlete's sport.
- Core Strength & Kinetic Chain Integration: Continue emphasis on core stability and full kinetic chain exercises (lower body, trunk, shoulder).
- Sport-Specific Drills: Begin specific drills relevant to the athlete's sport, e.g., gradual throwing progression, gymnastics specific movements, racket swings. This phase often involves an "Interval Throwing Program" for baseball players.
-
Return to Play Criteria:
- Full, pain-free range of motion.
- Strength symmetrical to the contralateral limb (typically >90-95%).
- No mechanical symptoms.
- Psychological readiness.
- Completion of sport-specific progression without pain or functional deficits.
Phase 4: Return to Sport (Typically 6-12+ Months)
- Goals: Full, unrestricted return to competitive sports.
- Progression: Continue monitoring for symptoms, refine sport-specific skills.
- Maintenance: Emphasize continued strength, flexibility, and proper technique to prevent recurrence.
Key Considerations:
*
Microfracture/OATS:
Often requires a longer period of protected weight-bearing and slower progression to impact activities (up to 6 months non-weight-bearing) to allow for graft incorporation and cartilage maturation.
*
Compliance:
Patient adherence to the rehabilitation protocol is crucial for successful outcomes.
*
Therapist Communication:
Close collaboration between the surgeon and physical therapist is essential for adjusting the protocol based on individual progress and challenges.
Summary of Key Literature / Guidelines
The body of literature on capitellar OCD management has expanded significantly, providing a growing evidence base for guiding clinical practice. Consensus, however, remains elusive regarding the optimal surgical strategy for all lesion types.
Non-Operative Management
Current guidelines generally advocate for an initial trial of non-operative management for stable, asymptomatic, or minimally symptomatic lesions in skeletally immature athletes without loose bodies.
*
Literature Support:
Several retrospective series and systematic reviews demonstrate favorable outcomes (healing, return to sport) with activity modification, rest, and rehabilitation in 50-70% of carefully selected patients. Success rates are higher in younger patients with open physes and smaller, stable lesions (Kida et al., 2004; Takahara et al., 2007).
*
Consensus:
A period of 3-6 months of strict activity modification is typically recommended. Failure to improve or progression of symptoms/instability on imaging warrants reconsideration of surgical intervention.
Surgical Interventions
The literature reflects a diverse array of surgical techniques, each with its own indications and reported outcomes.
-
Arthroscopic Debridement & Marrow Stimulation (Microfracture):
- Evidence: Long-term results are variable. Studies suggest good short-to-mid-term outcomes for small, contained lesions (<2-3 cm²), with pain relief and return to sport in 60-80% of cases. However, the fibrocartilage repair tissue may be less durable than hyaline cartilage (Kanaya et al., 2011; Bae et al., 2017).
- Guidelines: Remains a viable option for small, stable chondral lesions or unstable fragments unsuitable for fixation, but less ideal for large defects or significant subchondral bone loss.
-
Fragment Fixation (Arthroscopic or Open):
- Evidence: For large, unstable, but salvageable fragments, anatomical reduction and rigid internal fixation (using headless compression screws or bioabsorbable pins) yield superior outcomes to fragment excision (Matsumura et al., 2009; Shibata et al., 2017). High rates of union (70-90%) and return to sport (80-90%) are reported when successful. Hardware removal may be required for symptomatic implants, particularly with prominent or metallic fixation. Bioabsorbable implants carry a risk of sterile synovitis or fragmentation.
- Guidelines: The preferred technique for unstable, non-comminuted, anatomically reducible osteochondral fragments.
-
Osteochondral Autograft/Allograft Transplantation (OATS/OCA):
- Evidence: OATS (mosaicplasty) provides hyaline or hyaline-like cartilage repair, showing promising results for larger, contained defects, especially after failed primary fixation or for unfixable fragments (Kobayashi et al., 2004; Taguchi et al., 2012). Return to sport rates are comparable to fixation, but rehabilitation is typically longer. Allograft (OCA) is considered for very large defects or when autograft donor sites are exhausted, with good reported outcomes but concerns regarding cost, availability, and disease transmission (Hasegawa et al., 2010).
- Guidelines: Increasingly utilized for large, deep defects or salvage procedures, particularly in high-demand athletes. Donor site morbidity is a key consideration for autograft.
-
Autologous Chondrocyte Implantation (ACI) / Matrix-Associated Autologous Chondrocyte Implantation (MACI):
- Evidence: While more established in knee cartilage repair, its application in elbow OCD is less widespread. Initial reports suggest favorable outcomes for large, contained lesions, offering hyaline-like cartilage repair. Challenges include multi-stage procedures (for ACI), high cost, and a prolonged rehabilitation period (Peterson et al., 2010). MACI offers a single-stage alternative with promising early results.
- Guidelines: Reserved for select cases with large, well-contained defects where other options are less suitable or have failed.
Prognostic Factors & General Considerations
- Skeletal Maturity: Skeletally immature patients often have better healing potential, especially with stable lesions.
- Lesion Size & Stability: Smaller, stable lesions have a better prognosis with non-operative treatment. Large, unstable, or displaced lesions require surgical intervention for optimal outcomes.
- Loose Bodies: The presence of loose bodies is a strong indication for surgical intervention due to the risk of mechanical symptoms and further articular damage.
- Return to Sport: Generally, a successful return to sport ranges from 60-90% across various surgical techniques, with specific protocols (e.g., interval throwing programs) being crucial.
- Long-Term Outcomes: Concerns remain regarding the long-term risk of degenerative arthritis, particularly for larger lesions or those requiring more extensive reconstruction.
Key Guidelines
Several societies (e.g., American Academy of Orthopaedic Surgeons, American Sports Medicine Institute) offer guidance, emphasizing:
*
Individualized Treatment:
Tailoring the approach based on lesion characteristics, patient age, activity level, and goals.
*
Evidence-Based Decision Making:
Utilizing high-quality imaging and clinical assessment.
*
Shared Decision-Making:
Involving the patient and family in the treatment choice.
*
Comprehensive Rehabilitation:
A structured and progressive post-operative rehabilitation program is universally recognized as critical.
Future research should focus on randomized controlled trials comparing different surgical modalities, long-term functional and radiographic outcomes, and the development of biologic augmentation strategies to enhance cartilage repair and regeneration in this challenging athletic population.
