Introduction & Epidemiology
Distal biceps tendon rupture is a relatively uncommon but functionally devastating injury, predominantly affecting active, middle-aged males. It typically results from an eccentric load applied to a flexed elbow in a supinated forearm, such as lifting a heavy object or resisting an unexpected extension force. While the overall incidence is low, estimated at 1.2 per 100,000 person-years, its prevalence appears to be increasing, likely due to an aging yet active population.
The biceps brachii muscle is a powerful supinator and elbow flexor. A complete rupture of its distal attachment to the radial tuberosity leads to significant loss of supination strength (often 40-50%) and elbow flexion strength (approximately 30-40%), severely impairing activities of daily living and occupational performance. Partial tears, though less common and often more challenging to diagnose, can also result in persistent pain and functional limitation.
Timely and accurate diagnosis is crucial for optimal outcomes, as delayed presentation can complicate surgical repair due to tendon retraction, scarring, and muscle atrophy. The primary goal of treatment is to restore the anatomical insertion and biomechanical function of the biceps tendon, thereby maximizing strength and endurance in both supination and elbow flexion.
Surgical Anatomy & Biomechanics
A thorough understanding of the intricate anatomy surrounding the distal biceps tendon is paramount for successful surgical repair and minimization of iatrogenic complications.
The biceps brachii muscle originates from two heads: the short head from the coracoid process and the long head from the supraglenoid tubercle of the scapula. The muscle belly transitions into a robust, flattened tendon in the distal third of the arm, which then twists approximately 90 degrees as it crosses the elbow joint. This twist results in the short head fibers inserting more distally and anteriorly on the radial tuberosity, and the long head fibers inserting more proximally and posteriorly. This unique helical arrangement facilitates efficient supination.
The distal biceps tendon inserts onto the roughened, ulnar-sided aspect of the radial tuberosity. This insertion is critical, as it is the primary attachment point for the muscle's powerful supinating and elbow-flexing actions.
Key anatomical structures in close proximity and at risk during surgical approaches include:
- Radial Nerve: The main trunk of the radial nerve lies lateral to the distal humerus, giving off the posterior interosseous nerve (PIN) branch approximately 2-3 cm distal to the elbow joint, often beneath the supinator muscle or within the arcade of Frohse. The PIN is particularly vulnerable during posterior approaches or aggressive anterior dissection.
- Lateral Antebrachial Cutaneous Nerve (LACN): A terminal branch of the musculocutaneous nerve, the LACN provides sensation to the radial forearm and typically pierces the deep fascia between the biceps and brachialis muscles. It lies superficially and is susceptible to injury during skin incision and subcutaneous dissection.
- Brachial Artery and Median Nerve: These vital neurovascular structures lie medial to the biceps tendon in the cubital fossa, deeper than the lacertus fibrosus. They are generally protected by careful anterior dissection but can be at risk with aggressive medial retraction or deep penetration during tunnel drilling.
- Lacertus Fibrosus (Bicipital Aponeurosis): This fascial band extends from the medial aspect of the distal biceps tendon, crossing obliquely to insert into the deep fascia of the forearm, continuous with the flexor-pronator mass. It provides stability to the distal tendon and can act as a secondary attachment point, potentially maintaining some supination function in partial tears or even complete ruptures with significant retraction. Its release is often necessary during surgical repair to mobilize the retracted tendon.
Biomechanically, the distal biceps tendon is the primary supinator of the forearm, contributing approximately 80% of supination power, particularly against resistance. It also contributes significantly to elbow flexion (approximately 30-40%). Loss of this insertion leads to substantial functional deficits, especially for activities requiring powerful supination, such as using a screwdriver, turning a doorknob, or lifting heavy objects with the palm up. The integrity of the lacertus fibrosus can mitigate some of these losses in partial injuries, but rarely provides sufficient compensation in complete ruptures.
Indications & Contraindications
The decision for operative versus non-operative management of a distal biceps tendon injury hinges on several factors, including patient demographics, activity level, medical comorbidities, timing of injury, and the extent of the tear. For active patients with complete ruptures, surgical repair is generally indicated to restore optimal function.
Indications for Operative Management
- Complete Distal Biceps Tendon Rupture: This is the primary indication, especially in acute presentations.
- Active Patients: Individuals desiring to return to activities requiring full supination and flexion strength (e.g., athletes, manual laborers).
- Acute Injuries: Optimal surgical window is typically within 2-3 weeks of injury. Repair within this timeframe allows for easier tendon identification, less retraction, and lower complication rates.
- Significant Functional Deficit: Patients experiencing considerable weakness in supination or flexion, impacting daily activities or occupational demands.
- Partial Tears with Persistent Symptoms: If a partial tear causes chronic pain, weakness, or fails to respond to conservative management, surgical debridement and/or repair may be considered. Imaging (MRI) is crucial to assess the extent of the tear.
Indications for Non-Operative Management
- Low-Demand Patients: Sedentary individuals who do not require maximal supination or flexion strength for their daily activities.
- Significant Medical Comorbidities: Patients with severe systemic illnesses that preclude safe surgical intervention (e.g., uncontrolled diabetes, severe cardiovascular or pulmonary disease).
- Chronic Ruptures with Extensive Retraction and Scarring: While delayed repairs are possible, particularly with graft augmentation, the technical difficulty increases significantly beyond 4-6 weeks post-injury, and outcomes may be less predictable. Non-operative management might be considered if the risks of surgery outweigh potential benefits, or if the patient prefers it after informed consent.
- Select Partial Tears: Minor partial tears (<50% tendon involvement) that are asymptomatic or respond well to conservative treatment (rest, NSAIDs, physical therapy).
Contraindications for Surgical Repair
- Active Infection: Any local or systemic infection should be controlled prior to elective surgery.
- Severe Comorbidities: Unstable medical conditions posing an unacceptable anesthetic or surgical risk.
- Extremely Delayed Presentation (Relative Contraindication): While not an absolute contraindication, chronic ruptures (e.g., >3-6 months) with significant tendon retraction and muscle atrophy may necessitate complex reconstruction with allograft or autograft, making non-operative management an acceptable alternative for some patients.
- Non-Ambulatory or Non-Functional Limb: If the overall function of the limb is severely compromised by other conditions, the benefit of distal biceps repair may be limited.
Operative vs. Non-Operative Indications
| Feature | Operative Management | Non-Operative Management |
|---|---|---|
| Tear Type | Complete rupture (acute) | Select partial tears (asymptomatic, <50%) |
| Patient Activity | Active, high-demand, athletes, manual laborers | Sedentary, low-demand |
| Functional Goal | Restore full supination/flexion strength and endurance | Accept mild-moderate strength deficit, pain control |
| Timing | Acute (within 2-3 weeks post-injury) | Chronic (>4-6 weeks) with extensive retraction (consider for high risk pts) |
| Comorbidities | Minimal to moderate medical risks | Significant medical comorbidities precluding surgery |
| Symptoms | Significant weakness, cosmetic deformity | Minimal pain, acceptable functional deficit |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential to optimize surgical outcomes and mitigate potential complications.
Pre-Operative Assessment
- Clinical Diagnosis: Confirm diagnosis with a thorough history and physical examination. Key physical exam findings include a palpable defect in the distal arm, ecchymosis, tenderness in the cubital fossa, and weakness with resisted elbow flexion and supination. The "Hook Test" is highly sensitive and specific: inability to hook a finger under the intact distal biceps tendon from the lateral side of the cubital fossa is indicative of a complete rupture. Dynamic supination-pronation testing can also reveal loss of normal biceps muscle bulk excursion.
-
Imaging:
- Plain Radiographs: Obtain AP and lateral views of the elbow to rule out avulsion fractures of the radial tuberosity, which can sometimes occur with biceps ruptures.
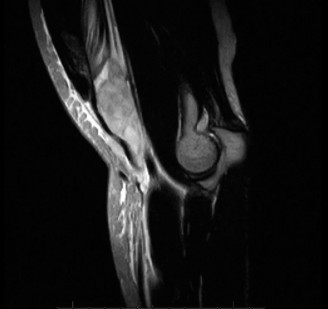
- Magnetic Resonance Imaging (MRI): While often not strictly necessary for acute, clinically obvious complete ruptures, MRI is the gold standard for confirming the diagnosis, assessing the extent of tendon retraction, identifying partial tears, and evaluating for associated injuries. It is particularly useful in chronic cases to estimate the gap and determine the feasibility of direct repair versus reconstruction.
- Timing of Surgery: Acute repair, ideally within 2-3 weeks of injury, is strongly recommended. Beyond this window, the tendon retracts, scars down, and muscle atrophy occurs, increasing surgical complexity and the potential need for tendon lengthening or graft augmentation.
- Patient Counseling: Discuss the procedure, expected outcomes, and potential complications, including nerve injury (radial nerve/PIN, LACN), heterotopic ossification, re-rupture, infection, and stiffness. Provide realistic expectations regarding rehabilitation and return to activities.
- Antibiotic Prophylaxis: Administer intravenous antibiotics (e.g., Cefazolin) within 60 minutes prior to incision.
Anesthesia
General anesthesia is typically employed. A regional nerve block (e.g., supraclavicular or interscalene brachial plexus block) can be a valuable adjunct for post-operative pain control, but should be used cautiously given the proximity of the distal biceps tendon to the radial nerve.
Patient Positioning
The patient is typically positioned supine on the operating table.
- Arm Table: The affected arm is placed on a hand table, ensuring adequate access to the anterior aspect of the elbow.
- Tourniquet: A pneumatic tourniquet is applied to the upper arm. This provides a bloodless field, which is critical for identifying and protecting neurovascular structures. The arm should be prepped and draped to allow full range of motion, particularly pronation and supination, which will be necessary intraoperatively for radial nerve protection and exposure of the tuberosity.
- Protection of Neurovascular Structures: Ensure appropriate padding for the contralateral arm and all pressure points. The forearm should be in a neutral position or slight pronation to help protect the radial nerve during anterior approaches.

Detailed Surgical Approach / Technique
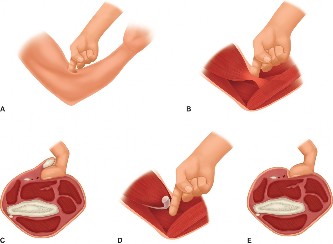
The goal of surgical repair is to re-establish the anatomical insertion of the distal biceps tendon to the radial tuberosity, thereby restoring biomechanical efficiency. Several techniques have evolved, but the most common approaches include the single-incision anterior approach and the two-incision (Boyes-O'Brien) approach. The single-incision anterior approach has gained favor due to its reduced soft tissue dissection and lower incidence of heterotopic ossification, provided careful attention is paid to radial nerve protection.
Single-Incision Anterior Approach (Preferred Technique)
This technique offers direct visualization of the distal biceps tendon and radial tuberosity while minimizing disruption to the posterior soft tissues.
-
Incision:
- A transverse or curvilinear incision, approximately 4-6 cm in length, is made in the antecubital fossa, following the natural skin crease. Alternatively, a longitudinal incision can be used, centered over the cubital fossa. The transverse incision generally offers a more aesthetic scar and better access to the neurovascular structures superficially, while the longitudinal incision allows for greater proximal and distal exposure.
- Care should be taken to avoid injury to the superficial branches of the lateral antebrachial cutaneous nerve (LACN), which typically lies subcutaneously, often anterior to the cephalic vein. Identify and gently retract these nerves.
-
Dissection:
- The incision is deepened through the subcutaneous tissue. The cephalic vein, if encountered, is retracted laterally.
- The bicipital aponeurosis (lacertus fibrosus) is identified. In a complete rupture, the aponeurosis may remain intact and prevent proximal retraction of the muscle belly, or it may also be torn. If intact, it is sharply incised and released along its medial border to facilitate tendon retrieval and mobilization.
- The interval between the brachioradialis laterally and the pronator teres medially is developed. This is the internervous plane.
-
Tendon Retrieval:
- The retracted distal biceps tendon stump is identified. It may be significantly retracted, sometimes into the mid-arm. Gentle traction on the muscle belly can help bring it into view.
- Often, a "fishing" suture (e.g., a heavy non-absorbable suture) is placed through the tendon stump using a long clamp or Kocher to prevent further retraction and to facilitate manipulation. Any devitalized tissue on the tendon end is debrided.
-
Protection of the Radial Nerve (PIN): This is the most critical step for avoiding neurological complications.
- With the forearm in full pronation , the posterior interosseous nerve (PIN), a deep branch of the radial nerve, moves away from the surgical field, typically posterior to the radial tuberosity and deep to the supinator muscle. This maneuver increases the distance between the PIN and the radial tuberosity.
- A deep, blunt Hohmann or cobra retractor is placed beneath the brachioradialis and supinator, hugging the anterior surface of the radius, retracting the muscle belly laterally to expose the radial tuberosity. This retractor acts as a physical barrier, protecting the PIN from drilling and reaming.
- Avoid aggressive deep medial retraction, which could endanger the brachial artery and median nerve.
-
Radial Tuberosity Preparation:
- With the forearm fully pronated, the radial tuberosity is visualized. Any remaining tendinous tissue or granulation tissue on the tuberosity is debrided using a burr or curette to create a bleeding, raw bone surface for optimal tendon-to-bone healing.
- A drill hole or series of holes is created in the tuberosity for tendon reinsertion. The technique for creating these tunnels depends on the chosen fixation method (e.g., cortical button, suture anchor, interference screw).
-
Fixation Methods:
-
Cortical Button (EndoButton®) Technique (Common and Robust):
- A single monocortical drill hole, typically 2.5 mm, is made from the anterior aspect of the radial tuberosity, traversing anterior to posterior.
- A second bicortical drill hole, 3.5-4.0 mm, is then created through this monocortical hole, exiting the posterior cortex of the radius. A specialized drill guide ensures proper trajectory and protects posterior structures.
- A long passing suture is advanced through this bicortical tunnel, and the cortical button, preloaded with sutures (e.g., FiberWire®), is passed through the anterior hole and out the posterior cortex.
- The button is then flipped to lie flat on the posterior cortex of the radius. The tendon stump is prepared with strong whipstitches (e.g., Krackow or Modified Kessler) using the same sutures as the cortical button.
- The sutures are then tensioned, drawing the tendon stump firmly into the prepared tunnel on the radial tuberosity. The tendon is typically placed into the tunnel in a slightly supinated position (approx 30-45 degrees) to optimize biomechanics.
- The sutures are tied over the cortical button, or a separate screw post system can be used to tension and secure the sutures.
-
Suture Anchor Technique:
- Multiple suture anchors (e.g., 2-4 anchors) are placed into the radial tuberosity. This may involve creating divergent drill holes for each anchor.
- The tendon is then sutured directly to the bone using the sutures from the anchors. This technique avoids the need for a posterior cortical exit, potentially reducing radial nerve risk, but may be biomechanically less robust than cortical button fixation.
-
Interference Screw Technique:
- A bone tunnel is reamed into the radial tuberosity, matching the size of the tendon stump.
- The tendon is prepared with sutures, pulled into the tunnel, and then an interference screw (bioabsorbable or titanium) is advanced alongside the tendon within the tunnel to compress it against the bone.
- This method requires a precise tunnel diameter and tendon size match and may not be suitable for all tendon morphologies.
-
Hybrid Techniques: Combinations, such as a cortical button for primary fixation and a supplementary suture anchor for rotational stability.
-
-
Tensioning and Assessment:
- Once the tendon is securely attached, the elbow is taken through a full range of motion (flexion, extension, pronation, supination) to ensure stable fixation and absence of impingement.
- The forearm is usually placed in a neutral or slightly supinated position at the time of final tensioning.
-
Wound Closure:
- Copious irrigation.
- The deep fascia is closed with absorbable sutures to cover the repair and prevent tendon bowstringing.
- Subcutaneous tissue and skin are closed in layers. A sterile dressing is applied, and the arm is placed in a hinged elbow brace or sling with the elbow flexed to 90 degrees and the forearm in neutral rotation.
Two-Incision (Boyes-O'Brien) Approach (Briefly)
This approach involves two separate incisions to minimize radial nerve risk by creating a distinct posterior exposure of the radial tuberosity.
- Anterior Incision: A transverse incision in the antecubital fossa is used to identify and retrieve the retracted biceps tendon. The tendon is whipstitched.
- Posterior Incision: A separate longitudinal incision is made over the proximal ulna, posterior to the mobile wad. Subperiosteal dissection of the supinator and brachioradialis exposes the posterior aspect of the radial tuberosity. This allows for direct visualization of the tuberosity for tunnel creation without risking the PIN.
- The whipstitches from the anterior incision are passed through the posterior incision, and the tendon is pulled through to the radial tuberosity and secured, typically with screw and washer or suture anchor fixation.
- Disadvantage: Higher risk of heterotopic ossification due to more extensive soft tissue disruption.
Complications & Management
Despite meticulous surgical technique, complications can occur following distal biceps tendon repair. Understanding these risks and their management is crucial for optimal patient care.
Common Complications
| Complication | Incidence (%) | Management Strategy |
|---|---|---|
| Neurological Injury | ||
| - Posterior Interosseous Nerve (PIN) | 0.5 - 10 | Prevention: Full pronation during drilling/reaming, deep retractor protecting PIN. Management: Often neuropraxia, managed with observation, bracing. If persistent deficit >3-6 months, consider nerve conduction studies/EMG. Exploration, neurolysis, or tendon transfers may be required in severe cases. |
| - Lateral Antebrachial Cutaneous Nerve (LACN) | 10 - 30 | Prevention: Careful subcutaneous dissection, identification, and retraction. Management: Usually neuropraxia/neuroma, leading to numbness/dysesthesia in radial forearm. Often self-resolving. Symptomatic neuromas may require local injection, desensitization, or surgical excision/transposition in rare, debilitating cases. |
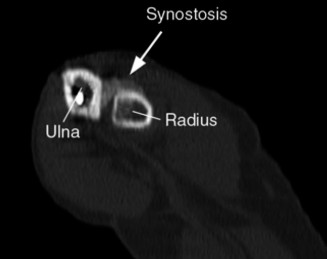
| Heterotopic Ossification (HO) | 1 - 20 | Prevention: Minimizing dissection, single-incision approach, post-op NSAIDs (e.g., Indomethacin for 3-6 weeks), consider low-dose radiation for high-risk patients (e.g., prior HO, extensive trauma). Management: Observation for asymptomatic HO. For symptomatic HO causing pain or severely restricted ROM, surgical excision after maturation (usually 6-12 months post-op) may be indicated. |
| Re-rupture | 1 - 5 | Prevention: Robust fixation, appropriate rehabilitation protocol avoiding early aggressive strain. Management: If symptomatic, revise surgically. May require autograft (e.g., hamstring) or allograft augmentation, especially if significant tendon loss or poor tissue quality. |
| Infection | 1 - 5 | Prevention: Standard aseptic technique, pre-operative antibiotics. Management: Superficial infections (cellulitis) typically respond to oral antibiotics. Deep infections may require surgical irrigation and debridement, IV antibiotics, and possibly hardware removal. |
| Loss of Motion/Stiffness | 5 - 15 | Prevention: Early controlled range of motion (post-op protocol), proper rehabilitation. Management: Aggressive physical therapy, dynamic splinting. If conservative measures fail, consider arthroscopic or open capsular release. |
| Painful Hardware | < 5 | Prevention: Proper placement of fixation devices. Management: Hardware removal after tendon healing (usually 6-12 months post-op), if symptoms persist. |
| Cosmetic Deformity ("Popeye" Sign) | Persistent if untreated. Can occur with re-rupture. | Prevention: Successful primary repair. Management: If present after rupture, surgical repair or reconstruction. If muscle belly migration causes concern after successful repair, typically observed. |
| Compartment Syndrome | Rare | Prevention: Careful hemostasis, judicious use of tourniquet time, avoid tight dressings. Management: Prompt fasciotomy if suspected. |
Detailed Management Considerations
- Neurological Injury: Most radial nerve and LACN palsies are transient neuropraxias. Close observation for 3-6 months is usually warranted. If no improvement, nerve conduction studies and EMG can help localize the injury and assess prognosis. Persistent deficits may necessitate neurolysis, nerve grafting, or tendon transfers (e.g., extensor carpi radialis longus to supinator for PIN palsy) to restore function. Patient education about potential sensory changes is critical pre-operatively.
- Heterotopic Ossification (HO): The two-incision approach has historically been associated with a higher incidence of HO. With the single-incision approach, the risk is reduced but still present. Prophylactic NSAIDs (e.g., Indomethacin 25 mg TID for 3-6 weeks) are commonly used. Radiation therapy (e.g., 700 cGy single dose) can be considered for high-risk patients. If HO causes severe pain or significantly restricts elbow motion after maturation (typically 6-12 months, when it appears stable on X-ray), surgical excision may be performed, often combined with aggressive post-operative physical therapy and repeat HO prophylaxis.
- Re-rupture: This is often due to inadequate fixation strength, premature aggressive loading, or poor tendon quality. Revision surgery is indicated for symptomatic re-ruptures. Depending on the remaining tendon length and tissue quality, this may involve direct repair, tendon lengthening procedures, or augmentation with allograft (e.g., Achilles, anterior tibialis) or autograft (e.g., semitendinosus, gracilis).
- Stiffness: Early, controlled range of motion post-operatively, as per a structured rehabilitation protocol, is vital to prevent stiffness. If stiffness develops, intensive physical therapy, serial casting, or dynamic splinting may be employed. Surgical options, such as arthroscopic or open capsular release, are reserved for refractory cases.
Post-Operative Rehabilitation Protocols
A structured and progressive rehabilitation protocol is paramount for optimizing outcomes after distal biceps tendon repair. The overarching goals are to protect the repair, restore full range of motion, regain strength, and facilitate a safe return to functional activities. The protocol typically involves three phases, with timelines that can be adjusted based on the specific fixation method, surgeon preference, patient compliance, and progress.
Phase I: Protection & Early Motion (Weeks 0-4)
- Goals: Protect the repair, reduce pain and swelling, initiate passive range of motion (ROM) without stressing the repair.
-
Immobilization:
- Sling or hinged elbow brace (locked or set to specific ROM) for 0-2 weeks. Elbow typically held at 90 degrees flexion with forearm neutral or slight supination.
- Transition to a hinged elbow brace by week 2, if not already in one. The brace provides controlled motion and prevents sudden extension or supination.
-
Range of Motion:
- Passive Elbow Flexion/Extension: 30-90 degrees for the first 2 weeks, progressing to 15-115 degrees by week 4. Therapist-assisted, non-weight-bearing.
- Passive Forearm Pronation/Supination: Initiate gentle passive pronation/supination within a pain-free range, avoiding resisted or active motion. Often restricted to neutral to full pronation, with limited supination (e.g., 0-30 degrees) to protect the repair.
- Wrist and Hand: Full active ROM for wrist and hand to prevent stiffness and maintain circulation.
-
Exercises:
- Gentle isometric contractions of the biceps (submaximal, in the brace), triceps, and forearm muscles. Avoid resisted supination.
- Scapular stabilization exercises.
- Weight Bearing: No weight bearing through the affected arm. Avoid lifting anything heavier than a cup of coffee.
- Patient Education: Emphasize strict adherence to restrictions, particularly avoiding active supination and sudden forceful elbow extension.
Phase II: Controlled Motion & Early Strengthening (Weeks 4-8)
- Goals: Gradually increase elbow and forearm ROM, initiate light strengthening, protect the healing tendon.
- Immobilization: Continue hinged elbow brace, typically unlocked for active ROM, but may be used during high-risk activities or sleep.
-
Range of Motion:
- Active-Assistive & Active Elbow Flexion/Extension: Progress to full elbow flexion and near-full extension (e.g., 0-130 degrees) by week 6-8.
- Active-Assistive & Active Forearm Pronation/Supination: Gradually increase active supination ROM as tolerated, aiming for full range by week 8. Avoid resisted supination.
-
Strengthening:
- Elbow Flexion: Gentle isometric exercises and light active flexion against gravity (e.g., with a therapist's hand or very light resistance bands).
- Forearm: Progressive isometric and light isotonic exercises for pronation and supination (avoiding resistance with supination initially).
- Wrist and Hand: Continue strengthening.
- Scapular Stabilizers & Rotator Cuff: Continue strengthening.
- Activities: Light activities of daily living. Avoid heavy lifting, pushing, or pulling.
- Pain Management: Continue with ice and NSAIDs as needed.
Phase III: Advanced Strengthening & Return to Activity (Weeks 8-16+)
- Goals: Restore full strength, power, and endurance; prepare for return to sport or demanding occupational activities.
- Immobilization: Discontinue brace when full ROM is achieved and strength is improving.
- Range of Motion: Full pain-free elbow and forearm ROM.
-
Strengthening:
- Progressive Resistive Exercises (PREs): Gradually increase resistance for all muscle groups, including elbow flexion, extension, pronation, and supination. Use dumbbells, resistance bands, and machines.
- Eccentric Loading: Incorporate eccentric exercises for the biceps.
- Functional & Sport-Specific Training: Begin activities that mimic work or sport demands. For instance, throwing drills for athletes, lifting specific objects for manual laborers.
- Core and Trunk Strengthening: Essential for overall upper extremity performance.
-
Return to Activity:
- Light work/Sedentary activities: Often possible by 8-12 weeks.
- Heavy lifting/Manual labor/Sport-specific training: Gradual return around 12-16 weeks, depending on strength, pain, and functional assessment. Full return to competitive sports or heavy labor may take 4-6 months, or even longer (up to 9-12 months for full strength recovery).
-
Criteria for Return to Play/Work:
- Full pain-free ROM.
- Strength of the injured arm is at least 80-90% of the contralateral, uninjured arm.
- Satisfactory performance on functional tests (e.g., throwing mechanics, lifting specific weights).
- No pain or instability during activity.
Throughout all phases, patient compliance and regular communication between the surgeon and physical therapist are crucial to ensure safe and effective progression. The protocol should be individualized, recognizing that healing rates and progress can vary significantly among patients.
Summary of Key Literature / Guidelines
The management of distal biceps tendon ruptures has evolved significantly over the past decades, transitioning from a predominantly non-operative approach to surgical repair as the gold standard for active individuals. Several key principles and findings from the literature guide current practice.
-
Superiority of Surgical Repair: Numerous studies, including systematic reviews and meta-analyses, consistently demonstrate that surgical repair of complete distal biceps ruptures provides superior outcomes in terms of strength recovery (especially supination strength), endurance, and objective functional scores compared to non-operative management. Patients treated non-operatively typically experience 30-50% loss of supination strength and 20-30% loss of flexion strength.
- Cain et al. (JBJS Am, 2007) : Highlighted the significant functional deficit with non-operative management.
- Ramirez et al. (Am J Sports Med, 2011) : Meta-analysis supporting superior strength and endurance after surgical repair.
-
Timing of Surgery: Acute repair (ideally within 2-3 weeks of injury) is strongly advocated. Delayed repairs (beyond 4-6 weeks) are technically more challenging due to tendon retraction, scarring, and muscle atrophy, often requiring extensive dissection, tendon lengthening procedures (V-Y plasties), or allograft/autograft augmentation. While good results can still be achieved in delayed cases with graft, the complication rate tends to be higher, and outcomes may be less predictable.
- Kelly et al. (J Shoulder Elbow Surg, 2000) : Discussed the challenges and outcomes of delayed repairs.
-
Surgical Approaches:
- Two-Incision Approach (Boyes-O'Brien): Historically popular, it provided excellent exposure of the radial tuberosity and protected the PIN by separating the anterior and posterior dissections. However, it is associated with a higher incidence of heterotopic ossification (up to 20%), a major complication limiting range of motion.
- Single-Incision Anterior Approach: This approach has gained widespread acceptance due to lower rates of heterotopic ossification and comparable functional outcomes. However, it necessitates meticulous technique for radial nerve protection (primarily the PIN) by ensuring full forearm pronation during drilling and careful retractor placement.
- Darlis et al. (J Shoulder Elbow Surg, 2007) and Amin et al. (J Bone Joint Surg Am, 2007) : Both studies compared the two approaches and found the single-incision technique associated with lower HO rates while maintaining good clinical outcomes.
-
Fixation Methods: Modern fixation techniques aim for strong, anatomically precise, and reproducible repairs.
- Cortical Button (e.g., EndoButton®): This method has demonstrated robust biomechanical strength, allowing for early rehabilitation. It provides a secure cortical fixation point and is a widely accepted standard.
- Suture Anchors: Offer a less invasive bony preparation (no posterior cortical exit) but may be biomechanically less strong than cortical buttons, especially against avulsion forces.
- Interference Screws: Provide good initial fixation but require precise tunnel sizing and may be prone to pull-out if the tendon-to-bone interface is not optimized.
- Most studies show comparable clinical outcomes across modern fixation techniques when performed correctly, with slight biomechanical advantages often cited for cortical button repairs in cadaveric studies. The choice often comes down to surgeon preference and familiarity.
- Mazzocca et al. (Am J Sports Med, 2007) : Biomechanical comparison of various fixation techniques.
-
Complications: Neurological injury (PIN and LACN) and heterotopic ossification remain the most common complications. Prophylactic measures, such as careful surgical technique (forearm pronation, diligent retraction), prophylactic NSAIDs, and selective radiation for HO, are critical for minimizing these risks.
- Schein et al. (J Shoulder Elbow Surg, 2018) : Review of complications and outcomes in distal biceps tendon repair.
-
Rehabilitation: Early controlled motion protocols, starting immediately post-operatively, are favored to prevent stiffness, promote tendon healing, and optimize functional recovery. Aggressive resisted supination and sudden forceful extension are avoided in the early phases to protect the repair. Gradual progression to strengthening and return to activity is key.
In conclusion, the prevailing evidence strongly supports acute surgical repair of complete distal biceps tendon ruptures in active patients using a single-incision anterior approach with robust cortical button fixation, followed by a structured rehabilitation protocol. While complications can occur, meticulous surgical technique and vigilant post-operative management can significantly mitigate these risks and lead to predictable, excellent functional outcomes. Continued research focuses on optimal management of chronic ruptures, refined surgical techniques, and advanced rehabilitation strategies.
Clinical & Radiographic Imaging