
Introduction & Epidemiology
Lateral elbow pain is a ubiquitous complaint encountered by orthopedic surgeons, with classic lateral epicondylitis (LEC) representing a significant proportion of these presentations. While the diagnosis and management of typical LEC, primarily involving the extensor carpi radialis brevis (ECRB) origin, are well-established, a subset of patients presents with "atypical" elbow pain. These cases often defy standard diagnostic algorithms, persist despite conventional non-operative and sometimes operative interventions for LEC, and necessitate a deeper exploration into the anatomical nuances of the extensor mechanism and related neurovascular structures. The extensor carpi radialis, particularly its brevis component, frequently emerges as a central figure in these enigmatic presentations, acting either as the primary pathological site or as an indicator of underlying, less obvious pathologies.
The epidemiology of lateral elbow pain is broad, affecting 1-3% of the general population, with peak incidence between 35 and 54 years of age. While the vast majority are successfully managed conservatively, a persistent subgroup requires surgical intervention. Within this surgical cohort, an appreciable percentage will present with atypical features, prompting suspicion for conditions beyond simple tendinosis. Such atypical presentations often include:
*
Deep-seated ECRB pathology:
Tendinosis or tears involving the deeper, articular-sided fibers of the ECRB, which may not respond to superficial debridement.
*
Radial Tunnel Syndrome (RTS):
Compression of the posterior interosseous nerve (PIN) within the radial tunnel, often presenting as diffuse, aching lateral forearm pain, exacerbated by resisted supination or wrist extension, sometimes mimicking or co-existing with LEC.
*
Posterolateral Rotatory Instability (PLRI):
Instability of the elbow joint, often subtle, which can lead to secondary overload and symptomatic irritation of the common extensor origin, including the ECRB.
*
Intra-articular pathology:
Synovitis, plica, or osteochondral lesions contributing to pain perceived in the lateral epicondyle region.
Distinguishing these entities from typical LEC requires a high index of suspicion, meticulous physical examination, and often advanced imaging. The ECRB’s intimate relationship with the radial nerve, its unique biomechanical role, and its propensity for both degenerative and compressive pathologies make it a critical structure to evaluate in the context of atypical lateral elbow pain. Understanding these less common presentations is paramount for orthopedic surgeons to optimize patient outcomes and avoid unnecessary or ineffective interventions.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and intricate biomechanics of the lateral elbow is foundational for diagnosing and managing atypical pain attributed to the extensor carpi radialis complex. The extensor carpi radialis group comprises two primary muscles: the Extensor Carpi Radialis Longus (ECRL) and the Extensor Carpi Radialis Brevis (ECRB).
Extensor Carpi Radialis Longus (ECRL)
- Origin: Arises from the distal third of the lateral supracondylar ridge of the humerus, the lateral intermuscular septum, and by a few fibers from the lateral epicondyle. It is more superficial and distinct from the common extensor origin.
- Insertion: Inserts onto the dorsal aspect of the base of the second metacarpal.
- Action: Primary wrist extensor and radial deviator.
- Innervation: Radial nerve (C6, C7).
Extensor Carpi Radialis Brevis (ECRB)
- Origin: Originates from the anterior aspect of the lateral epicondyle, deep to the ECRL and superficial to the radial collateral ligament. It is considered the major component of the common extensor origin, alongside the extensor digitorum communis (EDC). Its fibers blend with the annular ligament and the lateral collateral ligament complex, highlighting its role in elbow stability. The ECRB origin is the most common site of pathology in lateral epicondylitis.
- Insertion: Inserts onto the dorsal aspect of the base of the third metacarpal.
- Action: Primary wrist extensor (especially when the elbow is extended) and radial deviator. It is actively recruited during gripping and wrist extension, which puts significant strain on its origin during pronation and supination.
- Innervation: Posterior interosseous nerve (PIN), a deep motor branch of the radial nerve (C7, C8).
The distinction in innervation and, crucially, the ECRB's deep origin and close proximity to the radial head and annular ligament are critical. Pathological changes, such as tendinosis or microtears, often occur on the deep, articular surface of the ECRB, making them challenging to palpate or visualize with standard superficial techniques. This deep involvement can be a source of persistent, atypical pain, especially in activities involving combined wrist extension and forearm rotation.
Radial Nerve and Posterior Interosseous Nerve (PIN)
The radial nerve plays a critical role in atypical lateral elbow pain due to its anatomical course and susceptibility to compression, particularly its deep motor branch, the Posterior Interosseous Nerve (PIN).
*
Radial Nerve Course:
The radial nerve descends anterior to the lateral epicondyle, then divides into its superficial (sensory) and deep (motor, PIN) branches at the level of the radiocapitellar joint.
*
Posterior Interosseous Nerve (PIN):
The PIN dives anteriorly into the supinator muscle. Its entry point into the supinator is often constrained by a fibrous arch known as the
Arcade of Frohse
. This arcade is one of the most common sites of PIN compression.
*
Points of Compression within the Radial Tunnel:
The radial tunnel, extending from the radiocapitellar joint to the distal border of the supinator, encompasses five potential sites of PIN compression:
1.
Fibrous bands anterior to the radial head:
These can be found at the capitellum.
2.
Leash of Henry:
Recurrent radial vessels that cross the radial nerve.
3.
Extensor Carpi Radialis Brevis (ECRB) arcade:
The tendinous origin of the ECRB, particularly its deep surface, can be a compressive factor for the PIN, especially during forearm pronation and supination.
4.
Arcade of Frohse:
The fibrous proximal edge of the supinator muscle. This is considered the most common site of compression.
5.
Distal supinator fascia:
The distal edge of the supinator where the PIN exits.
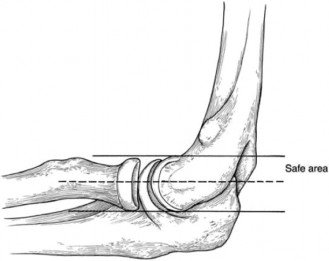
Figure 1: Illustration of the common extensor origin and the close relationship between the ECRB and the radial nerve/PIN pathway.
Compression of the PIN, known as radial tunnel syndrome, typically presents with diffuse aching pain in the lateral forearm, often without the specific tenderness over the lateral epicondyle seen in classic LEC. It is exacerbated by resisted forearm supination or repeated pronation/supination. Motor weakness is less common in RTS, differentiating it from true PIN palsy, where specific extensor deficits are evident. However, prolonged compression can lead to insidious weakness of wrist and finger extensors, sometimes with preserved ECRL function (radial nerve innervation).
Ligamentous Structures & Biomechanics
The lateral collateral ligament complex (LCLC) of the elbow, consisting of the radial collateral ligament, the annular ligament, and the lateral ulnar collateral ligament (LUCL), provides crucial posterolateral stability. The ECRB origin intimately blends with the annular ligament and contributes to the dynamic stability of the radial head. Subtleties in posterolateral rotatory instability (PLRI) can place increased stress on the common extensor origin, leading to secondary ECRB overload and pain that mimics tendinopathy. A comprehensive evaluation must consider the possibility of underlying instability, which, if untreated, can lead to persistent ECRB symptoms.
Biomechanically, the ECRB and ECRL are powerful wrist extensors and radial deviators. Activities involving repetitive grip with wrist extension (e.g., racquet sports, repetitive manual labor) or combined wrist extension and forearm pronation/supination impose significant tensile and shear forces on the ECRB origin. The "wringing out" effect on the PIN as it passes through the supinator, especially during dynamic forearm movements, can contribute to neural irritation, particularly when combined with inflammation or fibrosis around the ECRB origin. The deep location of the ECRB and its close association with the PIN make it a prime suspect in atypical lateral elbow pain.
Indications & Contraindications
The decision-making process for surgical intervention in atypical elbow pain centered on the extensor carpi radialis is complex, requiring careful consideration of conservative treatment failure, diagnostic certainty, and patient-specific factors.
Indications for Operative Intervention
Surgical intervention is generally reserved for patients with persistent, functionally limiting pain despite a thorough and prolonged course of non-operative management, typically lasting 6 to 12 months. Specific indications for surgery targeting the ECRB and/or radial nerve include:
-
Refractory Lateral Epicondylitis with Deep ECRB Pathology:
- Clinically localized tenderness specifically over the deep, articular aspect of the ECRB origin, distinct from superficial tenderness.
- Imaging (MRI or high-resolution ultrasound) demonstrating a significant tear, calcification, or severe tendinosis within the deep fibers of the ECRB, often extending towards the bone-tendon interface or into the substance of the tendon.
- Failure of conventional lateral epicondyle release and debridement in a prior surgery, necessitating exploration of deeper pathology.
- Positive diagnostic injection into the deep ECRB origin.
-
Clinically Diagnosed Radial Tunnel Syndrome (RTS):
- Characteristic diffuse, aching lateral forearm pain, often distal to the lateral epicondyle.
- Pain exacerbated by resisted forearm supination, resisted middle finger extension (Maudsley's test), or palpation of the radial tunnel.
- Absence of significant motor weakness (distinguishes it from PIN palsy).
- Failure of activity modification, physical therapy, NSAIDs, and targeted injections.
- While EMG/NCS are often normal in RTS, they may be useful to rule out other neuropathies or in cases with evolving motor deficits.
-
Concurrent Pathology Requiring Surgical Address:
- Confirmed posterolateral rotatory instability (PLRI) contributing to ECRB overload, necessitating lateral ulnar collateral ligament (LUCL) reconstruction in conjunction with ECRB treatment.
- Intra-articular loose bodies or synovitis causing secondary irritation of the common extensor origin.
- Cases where exploration is required to differentiate between ECRB pathology, radial tunnel syndrome, or other elusive sources of pain.
Contraindications for Operative Intervention
Contraindications, while not absolute in all cases, warrant careful consideration and discussion with the patient.
- Active Infection: Local or systemic infection must be controlled prior to elective surgery.
- Uncontrolled Systemic Inflammatory Conditions: Conditions such as rheumatoid arthritis or psoriatic arthritis may require optimization of medical management before surgical intervention, as healing can be impaired, and recurrence rates may be higher.
- Unrealistic Patient Expectations: Patients must have a clear understanding of the potential outcomes, risks, and the commitment required for post-operative rehabilitation.
- Significant Medical Comorbidities: Severe cardiac, pulmonary, or other systemic conditions that significantly increase anesthetic or surgical risk.
- Pain Primarily Attributable to Other Sources: If the elbow pain is predominantly secondary to cervical radiculopathy, shoulder pathology, or other distinct entities, these primary sources should be addressed first.
- Lack of Clear Surgical Target: Diffuse pain without a specific, anatomically identifiable pathological source on examination or imaging.
- Recent Onset of Symptoms: For tendinopathy or mild nerve compression, a prolonged trial of conservative management is always indicated prior to considering surgery.
Summary of Operative vs. Non-Operative Indications
| Feature | Non-Operative Management | Operative Management |
|---|---|---|
| Duration of Symptoms | Acute to subacute (< 6 months) | Chronic (> 6-12 months) and refractory to conservative treatment |
| Severity of Pain | Mild to moderate, manageable with activity modification | Severe, functionally disabling, impacting activities of daily living |
| Functional Limitation | Intermittent, allows most activities with some modification | Significant, prevents participation in work, sport, or ADLs |
| Response to Conservative Rx | Partial or complete improvement with PT, NSAIDs, bracing, injections | No significant or sustained improvement despite comprehensive Rx |
| Diagnostic Imaging | Mild tendinosis, no definitive tear, no nerve compression | Significant deep ECRB tear/calcification, clear signs of PIN compression, PLRI |
| Specific Clinical Tests | Classic LEC signs (e.g., Cozen's, Mill's) | Atypical pain distribution, positive Maudsley's, radial tunnel tenderness |
| Patient Factors | Realistic expectations, good compliance with PT | Realistic expectations, committed to rehabilitation, good general health |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for addressing atypical elbow pain related to the ECRB and radial nerve. It involves diagnostic refinement, detailed imaging review, patient education, and careful consideration of intra-operative logistics.
Diagnostic Refinement
- Clinical Re-evaluation: Before committing to surgery, a final comprehensive clinical assessment should confirm the diagnosis and rule out alternative pain generators (e.g., cervical spine, shoulder, other neuropathies). Special attention to radial tunnel specific tests (resisted supination, resisted middle finger extension, specific palpation) and stability tests (pivot shift for PLRI) is crucial.
-
Diagnostic Injections:
- ECRB Origin Injection: A precise injection of local anesthetic and corticosteroid (or platelet-rich plasma, PRP) into the deep ECRB origin can confirm its role as the pain source. Relief, even temporary, can be highly diagnostic.
- Radial Nerve Block: A diagnostic block of the radial nerve or specific radial tunnel injection can help delineate neural contribution to pain. However, caution is advised as a complete block can mimic PIN palsy.
-
Advanced Imaging Review:
- MRI: A high-resolution MRI of the elbow with specific sequences optimized for tendon and nerve visualization is paramount. Look for deep ECRB tears or degeneration, calcification, soft tissue edema, and anatomical variants. Crucially, scrutinize the course of the radial nerve and PIN for evidence of compression (e.g., nerve edema, narrowing of the radial tunnel).
- Dynamic Ultrasound: Can be helpful in experienced hands to assess tendon pathology and identify dynamic nerve compression during forearm rotation.
- Electromyography (EMG) and Nerve Conduction Studies (NCS): While often normal in pure radial tunnel syndrome, these studies are essential to rule out a true PIN palsy (with motor deficits) or other neuropathies that might mimic radial tunnel symptoms.
Pre-operative Counseling and Consent
- Thorough discussion regarding the likely pathology, the proposed surgical intervention (e.g., ECRB debridement, radial nerve decompression, or combined procedure), potential risks (nerve injury, recurrence, infection, stiffness), anticipated recovery timeline, and expected outcomes.
- Emphasize the importance of post-operative rehabilitation and patient compliance.
- Manage expectations, especially in chronic pain scenarios, where complete pain relief may not be achievable.
Patient Positioning and Preparation
The optimal patient position aims to provide unimpeded access to the lateral elbow and radial tunnel while ensuring patient safety and comfort.
-
Positioning:
- Supine with Arm on a Hand Table (preferred): The patient is positioned supine, with the affected arm abducted 90 degrees and the elbow flexed 90 degrees. The forearm is pronated and rested on a sterile hand table. This allows excellent access to the lateral epicondyle and the entire radial tunnel while maintaining a stable surgical field. The elbow joint can be easily manipulated for exposure.
- Lateral Decubitus: Less commonly used for this approach but can be an option if preferred by the surgeon. The patient lies on their contralateral side, with the affected arm draped over a sterile arm support or flexed across the chest.
- Tourniquet Application: A pneumatic tourniquet is routinely applied to the upper arm. This provides a bloodless field, crucial for identifying delicate neurovascular structures and delineating pathological tissue. The duration of tourniquet inflation should be monitored.
- Anesthesia: General anesthesia is typically employed. Regional anesthesia (e.g., interscalene block) can be combined with general anesthesia to provide excellent post-operative pain control, but care must be taken to not mask any immediate post-operative neurological deficits.
- Sterile Preparation and Draping: The arm is prepped and draped from the shoulder to the hand in a sterile fashion. The elbow joint should be freely movable under sterile conditions to allow for intraoperative assessment of stability and full range of motion.
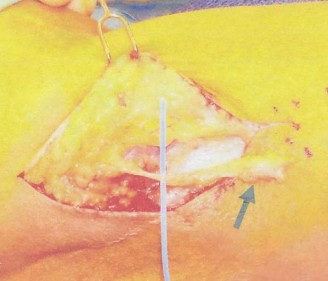
Figure 2: Typical patient positioning for lateral elbow surgery, showing the arm on a hand table, providing optimal access to the lateral epicondyle and radial tunnel region.
Detailed Surgical Approach / Technique
The surgical technique for atypical elbow pain focusing on the ECRB and radial nerve can involve a stand-alone ECRB debridement/repair, radial nerve decompression, or a combined approach. The objective is to address the specific pathology identified pre-operatively while minimizing iatrogenic injury.
1. Incision and Initial Dissection
- Skin Incision: A curvilinear or longitudinal incision, approximately 4-6 cm in length, is typically made over the lateral epicondyle, extending distally along the line of the radial head. This provides ample exposure for both ECRB pathology and the radial tunnel.
- Subcutaneous Dissection: The subcutaneous tissue is carefully dissected. The lateral antebrachial cutaneous nerve (LABCN) , a sensory nerve, lies subcutaneously on the anterolateral aspect of the elbow and should be identified and protected. It is often visualized superficial to the brachioradialis. Retract it anteriorly.
2. Exposure of the Common Extensor Origin and ECRB
- Fascial Incision: The deep fascia overlying the common extensor origin is incised longitudinally.
- Identification of ECRL and ECRB: The ECRL is more superficial and originates higher on the supracondylar ridge. The ECRB lies deep and anterior to the ECRL, originating from the lateral epicondyle. It is crucial to distinguish these.
- Exposure of ECRB Pathology: If deep ECRB pathology is suspected, the common extensor origin is incised longitudinally at the junction of the ECRL and ECRB, or through the ECRB itself, to allow reflection of its superficial fibers. This exposes the deep, articular surface of the ECRB tendon and its origin on the lateral epicondyle. Degenerated, discolored, or frayed tendon tissue, often with reactive hyperemia, will be evident. A careful search for tears, particularly on the undersurface of the tendon, is performed.
- Debridement and Decortication: The pathological ECRB tissue is sharply debrided. The underlying lateral epicondyle cortex is lightly decorticated using an osteotome or burr to promote a healing response. In cases of significant ECRB tear, sutures (e.g., non-absorbable, strong absorbable) may be used to repair the tendon back to the decorticated epicondyle or to its own healthy tissue (tendon-to-tendon repair).
- Assessment for PLRI: With the deep structures exposed, the elbow can be gently stressed into valgus and supination to assess for subtle posterolateral rotatory instability (pivot shift test). If instability is confirmed (e.g., during elbow flexion from full extension in supination, the radial head subluxates posteriorly), a lateral ulnar collateral ligament (LUCL) repair or reconstruction may be necessary.
3. Radial Nerve Exploration and Decompression (for Radial Tunnel Syndrome)
This step is performed if radial tunnel syndrome is suspected or confirmed.
*
Identification of Radial Nerve:
The radial nerve lies in the interval between the brachialis (medially) and the brachioradialis (laterally). Identify the radial nerve just proximal to the radiocapitellar joint.
*
Bifurcation:
The radial nerve typically bifurcates into the superficial radial nerve (SRN, sensory) and the posterior interosseous nerve (PIN, motor) at the level of the radial head. The SRN runs distally under the brachioradialis. The PIN dives anteriorly and distally into the supinator muscle.
*
Systematic Decompression:
The goal is to identify and release all five potential points of compression:
1.
Fibrous bands anterior to the radial head:
These are typically found at the entrance to the radial tunnel. Release any constricting bands.
2.
Leash of Henry:
Identify and ligate or coagulate any recurrent radial vessels that cross the nerve.
3.
ECRB Arcade:
The deep aspect of the ECRB origin can form a fibrous arch that compresses the PIN. This is often released during the ECRB debridement step. Ensure that the most proximal fibers of the ECRB, especially those originating from the anterior aspect of the lateral epicondyle and blending with the annular ligament, are sufficiently released from around the nerve.
4.
Arcade of Frohse:
This is the most common site of PIN compression. It is the fibrous proximal edge of the supinator muscle. With the forearm in supination, carefully incise the arcade of Frohse. As the arcade is released, the nerve should "pop out" and decompress. Exercise extreme caution as the PIN gives off motor branches immediately after exiting the supinator.
5.
Distal Supinator Fascia:
Continue to release the distal edge of the supinator and any other fascial bands until the PIN is completely free throughout its course within the supinator. The decompression should extend distally to the point where the PIN gives off its terminal branches.
*
Assessment of PIN:
After decompression, visually confirm the PIN is free from any constricting elements. The nerve should appear plump and move freely within its bed. The elbow and forearm can be taken through a full range of motion to ensure no dynamic compression.

Figure 3: Intraoperative view demonstrating the exposure of the radial nerve and PIN, with release of the Arcade of Frohse. Note the careful dissection required to protect the nerve branches.
4. Closure
- Tendon and Fascial Repair: If the ECRB origin was significantly incised or repaired, approximate the extensor fascia loosely to allow for gliding, or repair it if needed for structural integrity. Avoid overtightening.
- Subcutaneous Closure: Close the subcutaneous layer with absorbable sutures.
- Skin Closure: Close the skin with non-absorbable sutures or staples.
- Dressing: Apply a sterile dressing and a soft compressive bandage. Depending on the extent of pathology and stability, a temporary splint (e.g., posterior slab with the elbow at 90 degrees and neutral forearm) may be applied for 1-2 weeks.
Key Surgical Considerations:
- Magnification: Use of surgical loupes is highly recommended, especially during radial nerve dissection, to aid in the identification and protection of the nerve and its branches.
- Hemostasis: Meticulous hemostasis is crucial to prevent hematoma formation, which can compress the nerve post-operatively and complicate healing.
- Nerve Branches: Be acutely aware of the delicate motor branches of the PIN that supply the supinator and other forearm extensors. Any visible branches should be protected.
- Combined Procedures: When both deep ECRB pathology and radial tunnel syndrome are present, a combined approach is often necessary, ensuring comprehensive release and debridement.
Complications & Management
Despite meticulous surgical technique, complications can occur following surgery for atypical elbow pain involving the ECRB and radial nerve. Prompt recognition and appropriate management are crucial for optimal patient outcomes.
Table of Common Complications
| Complication | Incidence | Clinical Presentation | Management Strategy |
|---|---|---|---|
| Iatrogenic Nerve Injury (PIN) | Rare (<1-2%) | New or worsened wrist drop, finger drop, specific extensor weakness. | Immediate re-exploration if identified intra-op; observation with bracing, PT; neurolysis or nerve repair if no recovery at 3-6 months. |
| Iatrogenic Nerve Injury (SRN) | Rare (<1-2%) | Numbness, paresthesia on dorsoradial hand/thumb, positive Tinel's. | Conservative (observation, NSAIDs for neuritis); steroid injection; surgical neurolysis if persistent and debilitating. |
| Persistent or Recurrent Pain | 5-15% | Unresolved or returning elbow/forearm pain similar to pre-op. | Rule out misdiagnosis, inadequate decompression/debridement, scarring; revision surgery, targeted injections, PT, psychological support. |
| Infection (Superficial) | 2-5% | Erythema, warmth, tenderness, purulent discharge at incision site. | Oral antibiotics, local wound care; debridement if cellulitis progresses. |
| Infection (Deep) | <1% | Severe pain, fever, systemic signs, deep fluctuance. | Surgical irrigation and debridement, IV antibiotics, implant removal if applicable. |
| Hematoma | 2-5% | Swelling, ecchymosis, pain, potential nerve compression. | Conservative (compression, elevation, observation); surgical evacuation if large or symptomatic. |
| Elbow Stiffness / Decreased ROM | 5-10% | Loss of flexion/extension or pronation/supination. | Aggressive physical therapy, dynamic splinting; manipulation under anesthesia; capsular release in refractory cases. |
| Complex Regional Pain Syndrome (CRPS) | <1% | Disproportionate pain, autonomic dysfunction (swelling, color changes, temperature changes), trophic changes. | Early diagnosis, multidisciplinary approach (PT, pain management, stellate ganglion blocks, medication). |
| Scarring/Adhesions | Variable | Restricted soft tissue glide, cosmetic concerns. | Scar massage, desensitization, physical therapy. |
| Vascular Injury | Extremely Rare | Arterial bleeding, ischemia distal to injury. | Immediate surgical repair. |
Detailed Management Strategies
-
Iatrogenic Nerve Injury (PIN/SRN):
- Prevention is paramount. Meticulous dissection with loupes, clear identification, and protection of nerve structures are crucial.
- If a nerve injury (e.g., transection, severe traction) is recognized intraoperatively, immediate repair by a surgeon experienced in microsurgery (e.g., direct repair, nerve graft) is indicated.
- Post-operatively, if a PIN palsy (wrist/finger drop) is noted, immediate clinical assessment and often EMG/NCS are performed. If motor recovery does not begin by 3-6 months (typical window for neurapraxia to recover), surgical exploration, neurolysis, or nerve repair/reconstruction should be considered.
- SRN irritation/neuroma: Often managed conservatively with observation, desensitization, and nerve blocks. Surgical neurolysis or neurectomy with proximal nerve embedment into muscle may be considered for refractory cases.
-
Persistent or Recurrent Pain:
- This is often the most frustrating complication. Re-evaluate the initial diagnosis – was there a missed concomitant pathology (e.g., cervical radiculopathy, subtle PLRI, intra-articular pathology)?
- Assess for inadequate surgical decompression or debridement. Scarring around the nerve or an incomplete ECRB debridement can lead to persistent symptoms.
- Consider alternative pain generators or central sensitization.
- Management may involve further diagnostic injections, advanced imaging, revision surgery (e.g., more extensive nerve decompression, repeat ECRB debridement, or LUCL reconstruction), targeted physical therapy, and sometimes psychological counseling for chronic pain.
-
Infection:
- Superficial: Managed with oral antibiotics, local wound care, and close monitoring.
- Deep: Requires urgent surgical irrigation and debridement, often with hardware removal if applicable, followed by targeted intravenous antibiotics based on culture results. Prognosis depends on the extent of infection and host factors.
-
Hematoma:
- Small, non-expanding hematomas are managed conservatively with rest, ice, compression, and elevation.
- Large, rapidly expanding, or symptomatic hematomas (e.g., causing nerve compression) may require surgical evacuation.
-
Elbow Stiffness:
- Aggressive, early physical therapy focusing on regaining full range of motion is critical.
- Dynamic splinting can be employed.
- If persistent stiffness significantly impacts function, manipulation under anesthesia or an open/arthroscopic capsular release may be indicated.
-
Complex Regional Pain Syndrome (CRPS):
- A challenging complication requiring a multidisciplinary approach.
- Early diagnosis and aggressive treatment are crucial. This includes physical therapy, pain management specialists (nerve blocks, sympathetic blocks), and medication (gabapentin, tricyclic antidepressants).
Post-Operative Rehabilitation Protocols
Post-operative rehabilitation is a cornerstone of successful outcomes following surgical intervention for atypical elbow pain, particularly when addressing ECRB pathology and/or radial nerve decompression. The protocol must be tailored to the specific surgical procedure performed, the extent of pathology, and individual patient factors, balancing the need for protection with the goal of early, controlled motion.
General Principles
- Gradual Progression: Rehabilitation progresses through distinct phases, gradually increasing load and activity.
- Pain-Guided: Activities should not elicit significant pain.
- Patient Education and Compliance: Crucial for adherence to the protocol and understanding limitations.
- Emphasis on Proprioception and Neuromuscular Control: Especially important after nerve decompression.
Phase I: Protection & Early Motion (Weeks 0-2/3)
Goals:
* Pain and edema control.
* Protect surgical repair/decompression site.
* Maintain range of motion (ROM) in adjacent joints.
* Initiate gentle elbow ROM.
Interventions:
*
Immobilization:
* Soft dressing and posterior splint (elbow at 90 degrees flexion, forearm neutral or slight supination) for 1-2 weeks, especially if extensive ECRB repair or significant nerve decompression was performed.
* If minimal debridement, a simple soft dressing may suffice, allowing earlier motion.
*
Pain and Edema Management:
Ice, elevation, analgesics.
*
Active Range of Motion (AROM):
* Fingers, thumb, and shoulder AROM immediately.
* Gentle, pain-free wrist AROM (flexion/extension, radial/ulnar deviation), avoiding forceful wrist extension or supination, which can tension the ECRB and radial nerve.
* Passive forearm rotation (pronation/supination)
only if
Radial Tunnel Syndrome (RTS) was treated and the nerve needs gentle mobilization. Otherwise, avoid aggressive pronation/supination.
* Gentle, gravity-assisted elbow flexion and extension within protected range (e.g., 30-100 degrees initially) as tolerated and as per surgeon preference.
*
Precautions:
Avoid lifting, carrying, pushing, pulling. No forceful gripping. Avoid direct pressure on the incision site.
Phase II: Early Strengthening & Progressive Motion (Weeks 3-6/8)
Goals:
* Restore full, pain-free elbow and wrist ROM.
* Initiate gentle isometric strengthening.
* Improve neuromuscular control.
Interventions:
*
Range of Motion:
* Gradually increase active and passive elbow flexion/extension and forearm pronation/supination. Therapist-assisted stretching as tolerated.
* Continue wrist AROM.
*
Strengthening (Low Load, High Repetition):
* Begin with gentle isometric wrist extensors (ECRB/ECRL), wrist flexors, pronators, and supinators.
* Progress to very light isotonic exercises with minimal resistance (e.g., 1-2 lb weights, putty exercises).
* Begin grip strengthening with soft putty or stress ball.
*
Nerve Glides:
If RTS was treated, introduce gentle radial nerve gliding exercises to prevent adhesions.
*
Precautions:
Avoid heavy lifting. No forced terminal range stretching. Progress resistance cautiously.
Phase III: Progressive Strengthening & Functional Activities (Weeks 6/8-12)
Goals:
* Progressive strengthening of wrist and elbow musculature.
* Initiate sport-specific or work-specific simulation.
* Enhance endurance and power.
Interventions:
*
Strengthening:
* Increase resistance and volume for isotonic exercises (wrist extensors, flexors, pronators, supinators).
* Begin eccentric strengthening of wrist extensors.
* Incorporate shoulder girdle and core strengthening to optimize kinetic chain mechanics.
* Forearm isokinetic exercises.
*
Functional Progression:
* Introduce light functional activities simulating work or sport (e.g., typing, light tools, controlled tennis swings without impact).
* Focus on proper body mechanics and ergonomic modifications.
*
Proprioception:
Balance and coordination exercises for the upper extremity.
*
Precautions:
Avoid activities that cause pain or exacerbate symptoms. Ensure proper form with all exercises.
Phase IV: Return to Activity (Weeks 12+)
Goals:
* Gradual and safe return to full work, sport, and recreational activities.
* Maintain strength and flexibility.
* Prevent recurrence.
Interventions:
*
Advanced Strengthening:
Continue progressive resistance exercises, plyometrics if appropriate for sport.
*
Sport/Work-Specific Training:
Gradually increase intensity, duration, and frequency of activity. Simulate actual movements. Focus on technique modification to reduce stress on the elbow.
*
Endurance Training:
*
Maintenance Program:
Long-term home exercise program.
*
Monitoring:
Continued monitoring for any signs of recurrence.
*
Return to Play/Work Criteria:
Full pain-free ROM, full strength (comparable to contralateral side), absence of tenderness, completion of sport/work-specific drills without symptoms. This phase can extend for several months, particularly for overhead athletes or individuals with highly physical occupations.
Specific Considerations for Radial Nerve Decompression
- Avoid prolonged elbow extension with wrist flexion and pronation in the early phases, as this puts maximum stretch on the radial nerve.
- Gentle nerve gliding exercises are introduced early to encourage nerve mobility and prevent scar tissue adhesion around the decompression site.
- Neuropathic pain management may be necessary if persistent nerve irritation or dysesthesia occurs.
Summary of Key Literature / Guidelines
The literature on atypical elbow pain, particularly concerning the extensor carpi radialis and radial tunnel syndrome, highlights ongoing diagnostic challenges and evolving treatment strategies. While classic lateral epicondylitis (LEC) has a wealth of evidence, the rarer, atypical presentations often rely on smaller case series, expert opinion, and anatomical studies.
Extensor Carpi Radialis Brevis (ECRB) Pathology
- Pathoanatomy: Studies by Nirschl and others emphasized the angiofibroblastic hyperplasia (tendinosis) rather than inflammatory process in chronic LEC. More recent high-resolution imaging and arthroscopic findings have elucidated the role of deep-seated ECRB tears , often involving the attachment to the lateral epicondyle, which may be missed by superficial surgical approaches or routine imaging. These deep tears are a common finding in patients refractory to initial surgery.
- Diagnostic Tools: MRI is considered the gold standard for visualizing tendon integrity, specifically distinguishing deep ECRB tears from diffuse tendinosis. Dynamic ultrasound, in experienced hands, can also offer valuable real-time information. Diagnostic injections into the deep ECRB origin can confirm the pain source.
- Surgical Outcomes: Surgical debridement and reattachment of the ECRB, particularly for deep tears, have shown good to excellent results in up to 80-90% of appropriately selected patients refractory to conservative care. Arthroscopic approaches are increasingly used, offering improved visualization of the articular surface and the ability to address intra-articular pathologies simultaneously, while minimizing soft tissue disruption.
Radial Tunnel Syndrome (RTS)
- Controversy in Diagnosis: RTS remains a controversial diagnosis due to the absence of objective findings (EMG/NCS are typically normal) and its mimicry of LEC. The diagnosis is primarily clinical, based on characteristic pain patterns (diffuse aching lateral forearm pain, distal to the epicondyle) and specific provocative tests (e.g., resisted middle finger extension, resisted supination, palpation over the radial tunnel).
- Surgical Efficacy: The efficacy of surgical decompression for RTS is debated. Early series by Roles and Maudsley reported high success rates (70-90%), yet more recent rigorous studies suggest success rates may be lower, particularly in the absence of clear motor deficits or a definitive nerve entrapment visualized intraoperatively. A systematic review by Loos et al. (2019) highlighted the variability in diagnostic criteria and outcomes, underscoring the need for careful patient selection.
- Concomitant Pathology: It is well-recognized that RTS can co-exist with LEC. Some suggest that the inflamed ECRB origin itself can contribute to PIN compression. Therefore, a combined approach addressing both pathologies may be warranted if both are strongly suspected.
Posterolateral Rotatory Instability (PLRI)
- Subtle Presentation: PLRI, often due to injury of the lateral ulnar collateral ligament (LUCL), can manifest with subtle mechanical symptoms and lateral elbow pain that mimics tendinopathy. The dynamic nature of the instability can lead to secondary strain on the common extensor origin.
- Diagnosis: The pivot shift test (supination, valgus stress from full extension to flexion) is the classic clinical test, but it can be difficult to elicit under anesthesia. Imaging (stress radiographs, MRI) and arthroscopic evaluation are often necessary for definitive diagnosis.
- Management: Untreated PLRI can lead to recurrent ECRB symptoms. If confirmed, LUCL reconstruction is the definitive treatment, sometimes in conjunction with ECRB debridement.
Overall Guidelines and Future Directions
- Holistic Assessment: A comprehensive history, physical examination, and selective use of advanced imaging (MRI, dynamic ultrasound) and diagnostic injections are crucial for differentiating atypical elbow pathologies.
- Multidisciplinary Approach: Collaboration with physical therapists, pain management specialists, and neurologists can be beneficial, especially in complex or recalcitrant cases.
- Surgical Indications: Surgical intervention for atypical ECRB-related pain or RTS should be reserved for cases that have failed a well-structured, prolonged course of conservative management and have clear clinical and/or radiological evidence of a surgical target.
- Future Research: There is a continued need for high-quality, prospective studies with standardized diagnostic criteria and outcome measures for radial tunnel syndrome and deep ECRB pathology to establish clearer evidence-based guidelines for management. The role of biologics (e.g., PRP) in treating these specific entities also requires further investigation.
In conclusion, the extensor carpi radialis, particularly the ECRB, serves as a critical anatomical and biomechanical nexus in the differential diagnosis of atypical elbow pain. Its intricate relationship with the posterior interosseous nerve and its susceptibility to deep-seated pathology necessitate a sophisticated diagnostic approach and often a tailored surgical strategy to achieve successful patient outcomes.
