Patient Presentation & History
A 28-year-old male, a semi-professional rugby player, presents to the emergency department following a high-energy traumatic anterior shoulder dislocation. The mechanism of injury involved a direct tackle with his arm in an abducted and externally rotated position, resulting in immediate pain, loss of function, and a visibly deformed shoulder. This is his first documented shoulder dislocation. He reports a "clunk" sensation followed by excruciating pain. He was unable to move his arm and supported it with his contralateral limb.
His medical history is unremarkable. He denies any prior shoulder instability, pain, or significant trauma to the affected limb. He is a non-smoker and consumes alcohol socially. There are no known allergies, and he is not on any regular medications. His primary goal is to return to competitive rugby at his pre-injury level.
Clinical Examination
Upon initial inspection in the emergency department, the left shoulder exhibited the classic "shoulder pad" sign, indicative of an anterior glenohumeral dislocation, with prominence of the acromion and flattening of the deltoid contour anteriorly. The humeral head was palpable anteriorly and inferiorly, beneath the coracoid process. Ecchymosis was noted around the shoulder girdle, extending down the upper arm. There was no open wound or obvious skin compromise.
Palpation revealed significant tenderness globally around the glenohumeral joint. The patient guarded against any movement due to severe pain. Distal neurovascular status was assessed immediately. Radial, ulnar, and median pulses were 2+ bilaterally and symmetrically. Capillary refill was brisk in all digits.
Neurological assessment was crucial given the risk of axillary nerve injury. Sensation over the lateral deltoid patch was diminished (hypoesthesia) but not absent, suggesting a neuropraxia. Deltoid contraction was difficult to assess due to pain and guarding, but the patient could weakly abduct the arm against minimal resistance, indicating some axillary nerve sparing. Biceps, triceps, and wrist/finger flexor/extensor strength were intact and symmetric to the contralateral side.
Following initial reduction in the emergency department, which was performed under conscious sedation, the patient's pain significantly improved. Post-reduction examination:
*
Inspection:
Normal shoulder contour restored, but swelling and ecchymosis persisted.
*
Palpation:
Diffuse tenderness around the glenohumeral joint, particularly anteriorly and inferiorly. No crepitus with gentle motion.
*
Range of Motion (ROM):
*
Passive ROM:
Forward flexion to 90 degrees (pain-limited), abduction to 70 degrees (pain-limited), external rotation to 0 degrees (markedly limited by apprehension), internal rotation to T8 level (pain-limited).
*
Active ROM:
Significantly restricted across all planes due to pain and apprehension.
*
Special Tests for Instability (post-reduction, gently performed):
*
Apprehension Test:
Markedly positive with the arm in abduction and external rotation, reproducing the patient's fear of re-dislocation.
*
Relocation Test:
Relief of apprehension with posterior translation pressure on the humeral head.
*
Load and Shift Test:
Demonstrated increased anterior translation (Grade II, 50% translation without subluxation over glenoid rim) with a firm endpoint. Posterior and inferior translation were within normal limits.
*
Sulcus Sign:
Negative, ruling out significant inferior instability.
*
Neurological Assessment (post-reduction):
Hypoesthesia in the lateral deltoid patch persisted. Deltoid strength remained 3/5 against gravity, with subjective weakness. Remaining motor and sensory functions were normal. This indicated a persistent, likely neuropraxic, axillary nerve injury, warranting close monitoring.
Imaging & Diagnostics
Initial Radiographs (Post-reduction)
Immediate post-reduction radiographs (AP, Scapular Y, and Axillary views) were obtained.
*
AP View:
Demonstrated concentric reduction of the glenohumeral joint. A subtle osseous fragment was noted originating from the anteroinferior glenoid rim.
*
Scapular Y View:
Confirmed concentric reduction and provided a profile view of the glenoid.
*
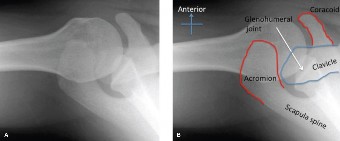
Axillary View:
This view was critical. It clearly revealed a
bony Bankart lesion
, an avulsion fracture of the anteroinferior glenoid rim, involving approximately 15% of the glenoid articular surface. It also showed a
Hill-Sachs lesion
, a compression fracture on the posterolateral aspect of the humeral head. The Hill-Sachs lesion appeared moderately sized.

Figure 1: Initial post-reduction X-ray demonstrating a bony Bankart lesion (arrow) and a Hill-Sachs lesion (arrowhead) on an Axillary view.
Computed Tomography (CT) Scan
Due to the suspicion of significant bony involvement from the plain radiographs, a dedicated CT scan of the left shoulder with 3D reconstructions was ordered. This was essential for accurate quantification of glenoid bone loss and precise characterization of the Hill-Sachs defect.
The CT scan findings were as follows:
*
Glenoid Bone Loss:
The bony Bankart lesion involved 22% of the anteroinferior glenoid articular surface. The fragment was displaced approximately 4mm and slightly rotated. The measurement was performed using the "best-fit circle" method on axial cuts, comparing the affected glenoid with the contralateral healthy glenoid, or using the glenoid track method.
*
Hill-Sachs Lesion:
A large, crescent-shaped compression fracture was confirmed on the posterolateral humeral head. The defect measured 2.5 cm in length and 0.8 cm in depth.
*
Glenoid Track Assessment:
Using 3D reconstructions and specific algorithms, the Hill-Sachs lesion was determined to be "off-track" relative to the bony Bankart defect and glenoid bone loss. This implied a high risk of engagement and recurrent instability if not addressed.
*
Associated Fractures:
No other significant fractures were identified.
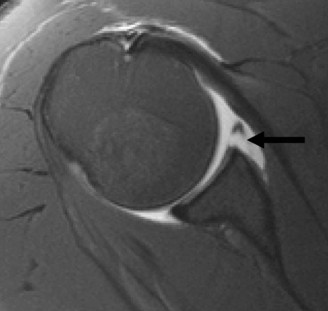
Figure 2: 3D CT reconstruction showcasing significant anteroinferior glenoid bone loss (bony Bankart) and a large posterolateral Hill-Sachs lesion on the humeral head.
Magnetic Resonance Imaging (MRI) Scan with Arthrogram
An MRI with arthrogram was performed to assess the integrity of the soft tissue structures, including the labrum, capsule, and rotator cuff, and to further delineate any articular cartilage damage.
The MRI findings confirmed:
*
Bony Bankart:
Consistent with CT findings, an avulsed fragment of the anteroinferior glenoid rim with associated capsulolabral detachment.
*
Hill-Sachs:
Confirmed the large posterolateral humeral head defect.
*
Labral Injury:
Complete detachment of the anterior and inferior labrum from the glenoid rim (soft tissue Bankart component) in conjunction with the bony fragment.
*
Capsular Injury:
Significant anterior capsular laxity and tearing.
*
Rotator Cuff:
Intact rotator cuff tendons (supraspinatus, infraspinatus, subscapularis, teres minor). No evidence of full-thickness or significant partial-thickness tears.
*
Articular Cartilage:
Mild chondral damage on the inferior aspect of the glenoid and opposing humeral head, consistent with the dislocation event.
*
Axillary Nerve:
The MRI did not show overt signs of nerve avulsion or significant structural damage, supporting the clinical diagnosis of neuropraxia.

Figure 3: Coronal MRI arthrogram depicting a detached anteroinferior labrum and bony Bankart fragment (arrow), along with contrast extravasation into the joint space.
Differential Diagnosis
The primary diagnosis for this patient is acute traumatic anterior glenohumeral instability with bony Bankart and engaging Hill-Sachs lesions . However, it is crucial to consider other potential shoulder pathologies in the differential, especially when managing acute trauma. The following table compares three relevant differentials:
| Feature | Bony Bankart/Hill-Sachs Instability (Present Case) | Soft Tissue Anterior Glenohumeral Instability (Pure Bankart) | Multidirectional Instability (MDI) | Rotator Cuff Tear (Post-Traumatic) |
|---|---|---|---|---|
| Mechanism of Injury | High-energy, traumatic abduction/external rotation. Often first episode. | Traumatic, abduction/external rotation. Can be recurrent. | Atraumatic, repetitive microtrauma, or generalized ligamentous laxity. Rarely acute trauma. | Acute trauma, fall on outstretched arm, heavy lifting, or chronic degeneration with acute exacerbation. |
| Clinical Presentation | Acute pain, deformity (if dislocated), apprehension, positive apprehension/relocation tests. | Acute pain, deformity (if dislocated), apprehension, positive apprehension/relocation tests. | Vague pain, instability in multiple directions (anterior, posterior, inferior), subtle subluxations. | Pain, weakness (especially abduction/external rotation), limited active ROM, positive cuff tests. |
| Palpation | Tenderness anteriorly/inferiorly, possible humeral head prominence. | Tenderness anteriorly/inferiorly. | Diffuse, less specific tenderness. | Tenderness over greater tuberosity/subacromial space. |
| ROM | Painful, guarded, apprehension at end-range ER/Abd. | Painful, guarded, apprehension at end-range ER/Abd. | Often full but apprehensive ROM, or generalized hypermobility. | Limited active ROM (especially abduction/ER), usually full passive ROM (unless chronic). |
| Special Tests | Positive Apprehension, Relocation, Surprise. Load and Shift (increased anterior). | Positive Apprehension, Relocation, Surprise. Load and Shift (increased anterior). | Positive Sulcus sign, generalized ligamentous laxity (Beighton score), often negative apprehension. | Positive Empty Can, External Rotation Lag, Lift-Off, Painful Arc. |
| X-ray Findings | Bony Bankart fragment , Hill-Sachs lesion . Possible glenoid bone loss. | Concentric reduction, but no osseous defects. | Concentric reduction, no osseous defects. | May show superior migration of humeral head (if massive tear), no osseous defects related to instability. |
| CT Scan | Quantifies glenoid bone loss, Hill-Sachs size, and glenoid track. | Normal glenoid/humeral head bony morphology. | Normal glenoid/humeral head bony morphology. | Normal bony morphology (unless associated fracture). |
| MRI Findings | Labral avulsion, capsular tear, bony fragment , Hill-Sachs lesion . | Labral avulsion (pure Bankart), capsular tear, no bony involvement. | Redundant inferior capsule, capsular laxity, no discrete labral tear (unless secondary). | Full or partial-thickness tear of one or more rotator cuff tendons. May have bursitis. |
| Treatment Considerations | High recurrence risk. Often surgical: Latarjet, bony Bankart repair, remplissage. | High recurrence risk. Often surgical: Arthroscopic Bankart repair. | Non-operative (PT, strengthening) first-line. If surgery, capsular plication/shift. | Non-operative (PT, NSAIDs) for partial/small tears. Surgical repair for larger, symptomatic tears. |
Surgical Decision Making & Classification
Given the patient's age (28 years), high activity level (semi-professional rugby player), first-time traumatic dislocation, and, most importantly, the significant bony pathology (22% glenoid bone loss with an "off-track" Hill-Sachs lesion), the decision for surgical intervention was unequivocal. Non-operative management, typically involving immobilization and rehabilitation, would result in an exceedingly high rate of recurrence (likely >80-90%) in this patient demographic and injury pattern.
The critical factors driving the surgical decision and choice of procedure were:
- Glenoid Bone Loss: The measured 22% glenoid bone loss is considered significant. While some literature suggests a threshold of 20-25% for open procedures like Latarjet, a pure arthroscopic Bankart repair in the presence of >20% bone loss carries a significantly higher failure rate, especially in overhead athletes or high-demand individuals. The presence of a bony fragment, even if it could be reattached, still meant loss of articular surface integrity and potential for glenoid wear.
- Hill-Sachs Lesion: The large, "off-track" Hill-Sachs lesion indicated that the humeral head defect would engage with the anterior glenoid rim during abduction and external rotation, acting as a fulcrum for re-dislocation. Ignoring an engaging Hill-Sachs lesion is a major cause of recurrent instability even after successful Bankart repair.
- Patient's Activity Level and Goals: As a semi-professional rugby player, the patient demands a robust, low-recurrence stabilization procedure to allow him to return to contact sports. Standard arthroscopic soft tissue repair alone would not provide the necessary stability.
- First-time Dislocation with Bony Injury: While some first-time dislocations can be managed non-operatively, the presence of substantial bony pathology (bony Bankart and engaging Hill-Sachs) shifts the indication strongly towards surgery, even for the initial event.
Classification Systems Used in Decision Making:
- Glenoid Bone Loss Classification: Assessed quantitatively via CT using the "best-fit circle" method. The 22% bone loss placed it above the typical threshold for arthroscopic soft tissue repair alone.
- Hill-Sachs Classification (On-Track/Off-Track): The critical determination that the Hill-Sachs lesion was "off-track" was paramount. This "glenoid track" concept compares the Hill-Sachs defect to the glenoid bone loss. An "off-track" lesion implies that the defect will engage the glenoid rim when the arm is in the apprehension position, thus requiring specific management (e.g., Latarjet or remplissage).
- Instability Severity Index Score (ISIS): Although primarily designed to predict recurrence after arthroscopic Bankart repair, this score reinforces the decision. Factors like age <20, hyperlaxity, participation in competitive sports, engaging Hill-Sachs, and significant glenoid bone loss contribute points. This patient would score high, further justifying a more robust stabilization.
Considering the cumulative factors, particularly the significant glenoid bone loss (22%) and the "off-track" engaging Hill-Sachs lesion in a high-demand athlete, an arthroscopic Latarjet procedure combined with arthroscopic remplissage was chosen. This combined approach would address both the glenoid bone deficiency and the engaging Hill-Sachs lesion, providing superior mechanical stability and minimizing the risk of recurrence. The bony Bankart fragment itself would be incorporated into the glenoid augmentation or excised if too comminuted.
Surgical Technique / Intervention
The chosen surgical intervention was a modified Arthroscopic Latarjet procedure with concomitant Arthroscopic Remplissage . This combined approach provides the "double barrier" effect, addressing both the anterior glenoid bone loss and the engaging posterolateral Hill-Sachs lesion.
Patient Positioning and Setup:
The patient was positioned in the
beach chair position
on a standard operating table. This position allows for easier access to both the anterior glenoid for the Latarjet and the posterior humeral head for the remplissage, while facilitating conversion to an open approach if necessary.
* The torso was tilted back approximately 45-60 degrees.
* The head was secured in a headrest, ensuring careful cervical spine alignment.
* The operative arm was draped free to allow for full range of motion.
* Standard arthroscopic tower and camera setup were prepared.
Diagnostic Arthroscopy:
Prior to commencing the Latarjet, a thorough diagnostic arthroscopy was performed through standard posterior and anterior portals.
* Assessment of the glenohumeral joint confirmed the significant anteroinferior labral detachment (soft tissue Bankart) with the avulsed bony Bankart fragment.
* The Hill-Sachs lesion on the posterolateral humeral head was clearly visualized.
* The articular cartilage surfaces of both the humeral head and glenoid were inspected for any further damage.
* The rotator cuff tendons, biceps tendon, and capsule were examined to rule out any missed injuries.
* The "off-track" nature of the Hill-Sachs lesion was re-confirmed arthroscopically by dynamically subluxing the humeral head anteriorly and observing the engagement of the Hill-Sachs defect with the glenoid rim.
Arthroscopic Latarjet Procedure:
The goal of the Latarjet procedure is to transfer the coracoid process, with its attached conjoined tendon (coracobrachialis and short head of biceps), to the anteroinferior glenoid rim. This provides a "bony block" to anterior translation and a "sling effect" from the conjoined tendon, enhancing dynamic stability.
- Portal Placement: An additional anterosuperior working portal ("5 o'clock portal") and a specific anterior-inferior portal were established for the Latarjet instruments.
-
Coracoid Preparation:
- The deltopectoral interval was identified and opened.
- The cephalic vein was retracted laterally.
- The conjoined tendon was dissected from the pectoralis minor.
- The tip of the coracoid process was carefully identified and prepared for osteotomy, ensuring preservation of the musculocutaneous nerve which lies medial to the conjoined tendon.
- Using an oscillating saw or osteotome, the coracoid was osteotomized at its base, approximately 1.5-2 cm from its tip, ensuring the conjoined tendon remained attached.
- The transferred coracoid block was then shaped to fit flush against the anteroinferior glenoid.
-
Glenoid Preparation:
- The bony Bankart fragment was identified. If it was large and well-vascularized, it could be re-attached or incorporated into the Latarjet graft. In this case, due to its comminuted nature and the planned Latarjet, the comminuted bony fragment was excised, and the glenoid neck was decorticated to create a bleeding surface for graft incorporation.
- Two pilot holes were drilled on the anteroinferior glenoid neck to match the drill holes in the coracoid graft.
-
Coracoid Transfer and Fixation:
- The coracoid graft, with the attached conjoined tendon, was passed through the subscapularis tendon (either splitting it or, as in this modified approach, passing beneath it).
- The graft was positioned flush against the prepared anteroinferior glenoid neck, ensuring it was level with the articular surface.
- Two 3.5 mm fully threaded cannulated screws were passed through the coracoid graft and into the glenoid neck, providing rigid compression and fixation. Proper screw trajectory was confirmed under fluoroscopic guidance to avoid intra-articular penetration.
- Capsulolabral Repair: The remaining redundant anterior capsule was meticulously repaired and tightened to the newly positioned coracoid block using absorbable sutures, creating a solid anterior bumper.
Arthroscopic Remplissage Procedure:
The remplissage (filling in) procedure addresses the "off-track" Hill-Sachs lesion by tenodesing the posterior capsule and infraspinatus tendon into the bone defect, effectively converting an "off-track" lesion to an "on-track" one by obliterating the engaging portion.
- Portal Placement: A standard posterior portal and a posterolateral portal (just distal to the posteromedial acromial corner) were used.
-
Hill-Sachs Visualization and Preparation:
- The Hill-Sachs lesion on the posterolateral aspect of the humeral head was clearly visualized.
- The bone within the Hill-Sachs defect was decorticated using a burr to promote bone-to-tendon healing.
-
Suture Anchor Placement:
- Two to three absorbable suture anchors were placed into the base of the Hill-Sachs defect.
- The sutures were then retrieved and passed through the posterior capsule and infraspinatus tendon.
-
Capsulotenodesis:
- The sutures were tied, securing the posterior capsule and infraspinatus tendon directly into the Hill-Sachs defect. This effectively "fills" the defect, preventing it from engaging the glenoid rim during abduction and external rotation. Care was taken to avoid over-tensioning, which could restrict external rotation.
Wound Closure:
All portals were closed with subcuticular sutures. Sterile dressings were applied. The patient was placed in a sling for immediate post-operative immobilization.
Post-Operative Protocol & Rehabilitation
The rehabilitation protocol following a combined Latarjet and Remplissage procedure is stringent, balancing protection of the bony and soft tissue repairs with early controlled motion to prevent stiffness.
Phase I: Protection and Early Controlled Motion (Weeks 0-6)
-
Immobilization:
- Shoulder immobilizer sling with a small abduction pillow (10-15 degrees) worn continuously for 4-6 weeks, removing only for hygiene and exercises.
- No external rotation beyond neutral for the first 6 weeks.
-
Pain and Swelling Management:
- Cryotherapy (ice packs) applied frequently.
- Analgesics as prescribed.
-
Exercises:
- Pendulum exercises: Gentle, gravity-assisted swings of the arm, 3-4 times daily.
-
Passive Range of Motion (PROM):
- Forward flexion to 90 degrees (supine position, therapist-assisted).
- Abduction to 45-60 degrees (therapist-assisted, limiting external rotation).
- Internal rotation to neutral (hand-to-belly, therapist-assisted).
- NO active motion of the shoulder joint.
- Elbow, wrist, hand ROM: Active exercises to prevent stiffness in uninvolved joints.
- Scapular setting exercises: Gentle isometric contractions of periscapular muscles (e.g., retraction, depression) to promote stability without glenohumeral motion.
- Weight Bearing: Non-weight bearing on the affected arm.
- Activities of Daily Living (ADLs): Avoidance of lifting, pushing, pulling. Emphasis on single-handed activities.
Phase II: Gradual Increase in Range of Motion (Weeks 6-12)
- Sling Use: Wean from sling, typically discontinued by week 6-8, depending on comfort and healing progression.
-
Range of Motion:
- Active-Assisted Range of Motion (AAROM): Begin with pulley exercises and cane-assisted movements.
- Active Range of Motion (AROM): Gradually progress AROM for forward flexion and abduction.
- External Rotation: Initiate gentle PROM external rotation, limited to 30-45 degrees, progressing cautiously to avoid stress on the anterior capsule and Latarjet graft. Avoid apprehension.
- Internal Rotation: Continue progression of internal rotation behind the back.
-
Strengthening (Isometric):
- Begin isometric exercises for rotator cuff and deltoid, with the arm in neutral.
- Focus on gentle co-contraction exercises for glenohumeral stability.
- Scapular Stabilization: Progress scapular strengthening exercises (e.g., rows, scaption with light resistance) with proper form.
- Neuromuscular Control: Introduction of proprioceptive exercises (e.g., rhythmic stabilization in protected ranges).
Phase III: Strengthening and Endurance (Weeks 12-24)
- Full ROM Attainment: Aim for full pain-free AROM in all planes, including external rotation, by the end of this phase.
-
Strengthening (Isotonic):
- Progress to isotonic exercises with resistance bands, light dumbbells.
- Focus on rotator cuff strengthening (internal/external rotation), deltoid (abduction, flexion), and periscapular muscles (serratus anterior, trapezius).
- Begin closed kinetic chain exercises (e.g., wall push-ups, planks) to enhance dynamic stability.
-
Power and Endurance:
- Introduce plyometric exercises for the upper extremity, gradually increasing intensity.
- Focus on endurance training relevant to sport.
- Axillary Nerve Recovery: Continue monitoring for axillary nerve recovery. If still significantly impaired, specific neuromuscular re-education may be needed.
Phase IV: Return to Activity / Sport-Specific Training (Weeks 24+)
- Advanced Strengthening: Continue with high-level strengthening, power, and endurance exercises.
-
Sport-Specific Drills:
- Gradual reintroduction of sport-specific movements and drills relevant to rugby (e.g., tackling, throwing, pushing, pulling).
- Progress from non-contact to contact drills under supervision.
-
Return to Play Criteria:
- Full, pain-free range of motion.
- Strength restored to >90% of the contralateral side, or functional equivalency.
- Excellent dynamic stability and neuromuscular control.
- Absence of apprehension during functional movements.
- Clearance from the surgeon and physical therapist.
- Timeline for Return to Contact Sports: Typically 6-9 months post-operatively for a Latarjet procedure, given the need for bone integration and capsule-tendon healing. The remplissage adds to the complexity and requires diligent adherence to restrictions.
Pearls & Pitfalls (Crucial for FRCS/Board Exams)
Pearls:
-
Comprehensive Pre-operative Imaging:
- Always obtain dedicated CT scans with 3D reconstructions for any suspected bony instability. This is crucial for accurate quantification of glenoid bone loss and precise characterization of the Hill-Sachs lesion.
- MRI is essential for soft tissue assessment, rotator cuff integrity, and associated injuries, but CT is paramount for bone.
-
Accurate Assessment of Bone Loss:
- Use validated methods (e.g., best-fit circle, PICO method) for glenoid bone loss measurement. The 20-25% threshold is a critical determinant for choosing augmentation (Latarjet, ICBG/DTA) over soft tissue repair.
- Don't just measure the fragment; assess the total glenoid bone deficiency.
-
Understanding the "Glenoid Track" Concept:
- Determine if the Hill-Sachs lesion is "on-track" or "off-track." An "off-track" lesion requires specific management (remplissage or humeral head resurfacing/allograft) to prevent engagement and recurrence, even if glenoid bone loss is addressed.
- The glenoid track is approximately 84% of the glenoid width. If the medial margin of the Hill-Sachs lesion lies medial to the glenoid track when the arm is in the apprehension position, it is "off-track."
-
Individualized Treatment Plan:
- Tailor the surgical approach to the patient's demographics (age, activity level), demands (contact sport, overhead athlete), and specific pathology (type and extent of bony lesions, ligamentous laxity). The ISIS score is a useful tool.
-
Robust Fixation of Bony Bankart/Graft:
- For bony Bankart repair, ensure anatomical reduction and rigid fixation (e.g., cannulated screws, suture anchors with compression).
- For Latarjet, ensure the coracoid graft is flush with the glenoid surface and rigidly fixed with bicortical screws. Avoid articular penetration.
-
Addressing the Engaging Hill-Sachs Lesion:
- If the Hill-Sachs lesion is "off-track," it must be addressed. Remplissage is an excellent arthroscopic solution for smaller to moderate defects. For very large defects, allograft reconstruction of the humeral head may be considered.
-
Concomitant Injuries:
- Always rule out rotator cuff tears, biceps pathology, or nerve injuries (especially axillary nerve) during diagnostic arthroscopy and clinical evaluation. Address them if present.
Pitfalls:
- Underestimating Bone Loss: The most common cause of failure after arthroscopic soft tissue Bankart repair. Relying solely on X-rays or inexperienced assessment can lead to misdiagnosis and inadequate treatment.
- Ignoring an Engaging Hill-Sachs Lesion: Failing to identify or adequately address an "off-track" Hill-Sachs lesion will lead to early recurrence, even after a technically perfect glenoid repair. This is a common pitfall.
- Inadequate Glenoid Preparation for Bony Bankart/Latarjet: Poor decortication or improper seating of the bony Bankart fragment or coracoid graft can lead to non-union or pseudoarthrosis, compromising stability.
- Over-Tensioning in Remplissage: Excessive tension during remplissage can lead to a significant loss of external rotation, which can be detrimental to an athlete. Balance stability with range of motion.
- Aggressive Early Rehabilitation: Premature or overly aggressive rehabilitation, especially with external rotation or active shoulder motion, can compromise the healing of the capsulolabral repair, bony Bankart fragment, or Latarjet graft, leading to re-dislocation. Adherence to a structured, protected protocol is critical.
- Failure to Recognize Neurological Deficits: Missing an axillary nerve neuropraxia or more severe injury can have long-term functional consequences. Thorough pre- and post-operative neurological assessment is mandatory.
- Inaccurate Graft Positioning in Latarjet: Placing the coracoid graft too medially can lead to non-union or impingement, while placing it too laterally can make it less effective as a bony block. Correct positioning, flush with the articular surface, is key.
Clinical & Radiographic Imaging