Introduction & Epidemiology
Acute rotator cuff tears represent a distinct clinical entity within the spectrum of rotator cuff pathology, characterized by a sudden, often traumatic, onset of symptoms following a specific inciting event. Differentiating acute from chronic tears is paramount, as the former typically presents with greater reparability and potentially superior outcomes with timely intervention. While the exact definition can vary, an acute tear is generally considered one occurring within 6 weeks to 3 months of symptom onset, often associated with a identifiable traumatic event such as a fall onto an outstretched arm, heavy lifting, or a sudden forceful contraction against resistance.
The epidemiology of acute rotator cuff tears is influenced by several factors. While age is a significant risk factor for chronic degenerative tears, acute tears can occur across a broader age range, particularly in younger, more active individuals involved in sports or physically demanding occupations. The incidence of full-thickness rotator cuff tears in the general population is estimated to be approximately 20-30% in individuals over 60 years of age, but a substantial proportion of these are asymptomatic or chronic. Traumatic tears, specifically, constitute a smaller but clinically significant subset. Studies suggest that acute tears account for 10-20% of all symptomatic rotator cuff tears. Risk factors include male gender, participation in overhead activities, and pre-existing cuff tendinopathy, which may predispose the tendon to failure under acute stress. The size and location of acute tears are variable, with the supraspinatus tendon being the most frequently affected, either in isolation or in combination with the infraspinatus. Less commonly, the subscapularis or teres minor may be involved, often in high-energy trauma. The critical zone of the supraspinatus, an area of relative hypovascularity located 10-15 mm proximal to its insertion on the greater tuberosity, is particularly susceptible to both acute traumatic and chronic degenerative processes. Early and accurate diagnosis of acute tears is crucial, as delayed treatment can lead to tendon retraction, muscle atrophy, fatty infiltration, and subsequently, diminished reparability and poorer functional outcomes.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy and biomechanics of the shoulder girdle is foundational to the successful diagnosis and treatment of acute rotator cuff tears. The rotator cuff comprises four muscles: the supraspinatus, infraspinatus, teres minor, and subscapularis.
Rotator Cuff Muscles and Tendons
- Supraspinatus : Originates from the supraspinous fossa and inserts onto the superior facet of the greater tuberosity. Innervated by the suprascapular nerve (C5, C6). Primarily responsible for initiation of abduction and superior humeral head depression.
- Infraspinatus : Originates from the infraspinous fossa and inserts onto the middle facet of the greater tuberosity. Innervated by the suprascapular nerve (C5, C6). Primarily responsible for external rotation and posterior humeral head depression.
- Teres Minor : Originates from the lateral border of the scapula and inserts onto the inferior facet of the greater tuberosity. Innervated by the axillary nerve (C5, C6). Primarily responsible for external rotation and posterior humeral head depression.
- Subscapularis : Originates from the subscapular fossa and inserts onto the lesser tuberosity. Innervated by the upper and lower subscapular nerves (C5, C6, C7). Primarily responsible for internal rotation and anterior humeral head depression.
These tendons coalesce to form a confluent cuff that envelopes the humeral head, contributing significantly to glenohumeral joint stability through concavity compression and dynamic centralization of the humeral head within the glenoid fossa.
Critical Anatomical Structures
- Rotator Cuff Footprint : The insertion site of the rotator cuff tendons on the greater and lesser tuberosities of the humerus. This area is crucial for repair, and its integrity and preparation are essential for tendon-to-bone healing. The average footprint of the supraspinatus and infraspinatus collectively spans approximately 25-30 mm in the anteroposterior direction and 12-15 mm in the mediolateral direction on the greater tuberosity.
- Coracoacromial Arch : Formed by the coracoid process, the coracoacromial ligament, and the acromion. This arch provides superior stability but can also impinge upon the rotator cuff, particularly in subacromial impingement syndrome. Acromial morphology (Type I: flat, Type II: curved, Type III: hooked) plays a role in chronic impingement and potential tear propagation.
- Biceps Tendon : The long head of the biceps brachii tendon originates from the supraglenoid tubercle and glenoid labrum and traverses the bicipital groove. Its pathology (tendinopathy, instability, tears) often coexists with rotator cuff tears and may require concomitant tenodesis or tenotomy.
- Neurovascular Structures : The suprascapular nerve courses through the suprascapular notch and then the spinoglenoid notch, innervating the supraspinatus and infraspinatus muscles. It is vulnerable during posterior portal placement or extensive posterior capsular release. The axillary nerve wraps around the surgical neck of the humerus and is at risk during inferior glenohumeral capsule work or excessive traction.
Biomechanics of Rotator Cuff Tears
The rotator cuff functions as a force couple, balancing the deltoid’s superior migration force during abduction and flexion, while simultaneously compressing the humeral head into the glenoid. Acute tears disrupt this intricate balance, leading to pain, weakness, and altered kinematics.
*
Loss of Force Couple
: A torn supraspinatus compromises the superior depressor function, leading to unopposed deltoid contraction and superior migration of the humeral head, especially with large or massive tears. This can result in impingement, erosion of the undersurface of the acromion, and glenoid wear (rotator cuff arthropathy).
*
Tendon Retraction
: Acute tears, particularly traumatic ones, often result in significant tendon retraction due to the elastic recoil of the musculotendinous unit. The degree of retraction (Patte classification) and the extent of fatty infiltration (Goutallier classification) are critical prognostic indicators for reparability and healing potential.
*
Healing Biology
: Tendon-to-bone healing at the footprint relies on fibrovascular scar formation, which mimics Sharpey's fibers but often lacks the organized collagen structure of native enthesis. Biologic augmentation strategies aim to enhance this healing process.
Indications & Contraindications
The decision to proceed with operative or non-operative management for acute rotator cuff tears is multifactorial, requiring careful consideration of patient factors, tear characteristics, and functional goals.
Operative Indications
- Acute, Symptomatic, Full-Thickness Tears : Especially in younger, active patients (<60-65 years) who desire to maintain a high level of function. This includes tears occurring within 3-6 months of onset.
- Traumatic Tears : High-energy injury resulting in a full-thickness tear, regardless of patient age, particularly if there is significant functional deficit or retraction.
-
Partial-Thickness Tears
:
- Greater than 50% tendon thickness involved.
- Symptomatic PASTA (Partial Articular-Sided Tendon Avulsion) lesions.
- Failed non-operative management over 3-6 months with persistent pain and functional limitation.
- Significant Functional Deficit : Marked weakness, loss of active range of motion, or inability to perform activities of daily living.
- Associated Pathology : Concomitant pathologies that necessitate surgical intervention, such as significant biceps pathology (instability, tendinopathy, tears) or acute labral tears.
- Subscapularis Tears : Especially if traumatic or involving the superior 2/3 of the tendon, as these often lead to significant dysfunction and can destabilize the biceps.
Non-Operative Indications
- Small, Asymptomatic Tears : Incidental findings on imaging without significant pain or functional impairment.
- Partial-Thickness Tears : Less than 50% tendon thickness, especially if asymptomatic or minimally symptomatic.
- Degenerative Tears : Atraumatic, chronic tears, particularly in low-demand, elderly patients, where pain is the primary symptom and conservative measures have not been exhausted.
- Significant Medical Comorbidities : Patients with high surgical risk (e.g., severe cardiopulmonary disease, uncontrolled diabetes, active infection) where the risks of surgery outweigh the potential benefits.
- Non-compliance : Patients who are unwilling or unable to participate in a rigorous post-operative rehabilitation protocol.
- Irreparable Tears : In cases of massive, retracted tears with severe fatty infiltration and muscle atrophy, where repair is not feasible, and the patient is not a candidate for reconstructive options like reverse shoulder arthroplasty or superior capsule reconstruction.
Contraindications to Repair
-
Absolute Contraindications
:
- Active local or systemic infection.
- Severe, uncontrolled medical comorbidities precluding safe anesthesia and surgery.
- Neuropathic arthropathy.
-
Relative Contraindications
:
- Severe glenohumeral osteoarthritis (often warrants arthroplasty).
- Massive, chronic, irreparable tears with severe fatty infiltration and atrophy (Goutallier stage 3 or 4) that are not amenable to any reconstructive options.
- Extremely elderly, low-demand patients with minimal symptoms.
- Non-compliance with post-operative rehabilitation.
- Inadequate tissue quality for durable repair.
| Indication Category | Operative Management (Repair) | Non-Operative Management |
|---|---|---|
| Tear Type | Acute, symptomatic, full-thickness (especially traumatic) | Small, asymptomatic, full-thickness (incidental) |
| Partial-thickness >50% or symptomatic PASTA | Partial-thickness <50% | |
| Full-thickness subscapularis tears | Atraumatic, degenerative tears (low demand) | |
| Patient Age | Younger, active (<60-65 years) | Elderly, low-demand |
| Symptom Duration | Acute (within 3-6 months of onset) | Chronic (>6 months) with minimal symptoms |
| Functional Deficit | Significant weakness, loss of active ROM, functional impairment | Mild symptoms, preserved function, or acceptable impairment |
| Prior Treatment | Failed non-operative management (for partial tears) | Initial management for most atraumatic partial/small full tears |
| Comorbidities | Good general health, manageable comorbidities | Significant medical comorbidities precluding surgery |
| Compliance | Patient compliant with rehabilitation | Unwilling/unable to comply with rehabilitation |
| Tear Characteristics | Minimal retraction, good tissue quality, minimal fatty infiltration | Severe retraction, poor tissue quality, severe fatty infiltration (irreparable) |
| Associated Pathology | Significant biceps pathology requiring intervention | Minimal associated pathology |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is critical for optimizing outcomes in acute rotator cuff repair. This involves comprehensive patient evaluation, detailed imaging review, and precise surgical setup.
Patient Evaluation
A thorough history should focus on the mechanism of injury, onset of symptoms, pre-existing shoulder conditions, and the patient's functional demands. Physical examination assesses active and passive range of motion, strength of the rotator cuff muscles (Jobe's, external rotation lag sign, lift-off, belly-press), impingement signs, and biceps and labral integrity. Neurovascular status must be documented.
Imaging Review
- Plain Radiographs : Standard anteroposterior, scapular Y, and axillary views are essential to assess glenohumeral arthritis, acromial morphology, acromioclavicular joint pathology, and rule out fractures or dislocations. AP stress views can indicate superior humeral head migration.
-
Magnetic Resonance Imaging (MRI)
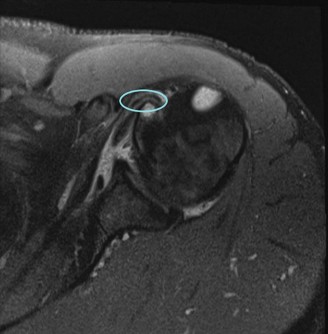
: This is the gold standard for diagnosing rotator cuff tears. MRI accurately delineates tear size, morphology (full-thickness vs. partial, articular vs. bursal), tendon retraction (Patte classification), muscle atrophy, and fatty infiltration (Goutallier classification). It also helps identify associated pathologies such as labral tears, biceps pathology, and bone bruising. The presence of acute hemorrhage or edema in the musculotendinous unit helps differentiate acute from chronic tears.

Figure 1: Pre-operative MRI depicting a full-thickness acute rotator cuff tear with mild retraction. - Ultrasound : Can be a useful dynamic imaging modality, especially in experienced hands, for detecting full-thickness tears and assessing muscle contractility. It is operator-dependent and less reliable for partial tears or assessing fatty infiltration.
- CT Arthrogram : Less commonly used for rotator cuff tears but can be helpful in cases where MRI is contraindicated or inconclusive, especially for delineating articular-sided partial tears.
Anesthesia and Analgesia
General anesthesia is typically employed. A regional interscalene nerve block administered pre-operatively by an anesthesiologist provides excellent post-operative pain control, reducing opioid requirements and facilitating early rehabilitation. Local anesthetic infiltration during surgery also contributes to pain management.
Patient Positioning
Two primary positions are utilized for arthroscopic shoulder surgery:
1.
Beach Chair Position
:
*
Advantages
: Easier transition to open procedure if necessary, maintenance of standard anatomical orientation, easier airway management.
*
Setup
: Patient is semi-recumbent at 60-70 degrees, head secured, arm draped free. The head should be maintained in a neutral position to avoid brachial plexus stretch.
*
Considerations
: Risk of hypotension (cerebral hypoperfusion) if not managed appropriately. Care must be taken to pad all bony prominences.
2.
Lateral Decubitus Position
:
*
Advantages
: Allows for aggressive traction and gravitational assistance for visualization, particularly useful for larger patients or extensive procedures. Potentially lower risk of cerebral hypoperfusion.
*
Setup
: Patient lies on the contralateral side, secured with beanbag or vacuum mattress. The operative arm is placed in a traction tower with 10-15 pounds of weight and 30-45 degrees of abduction and flexion. A lateral support is placed to maintain the patient's position.
*
Considerations
: Potential for traction-related nerve injury (brachial plexus), particularly the suprascapular nerve, if excessive weight or duration is used.
For acute rotator cuff repair, both positions are viable. The choice often depends on surgeon preference, specific tear characteristics, and patient body habitus. Regardless of position, careful padding, securing of the patient, and monitoring of neurovascular status are paramount.
Detailed Surgical Approach / Technique
The detailed surgical approach for acute rotator cuff repair typically involves an arthroscopic technique, offering superior visualization, reduced morbidity, and faster recovery compared to traditional open repairs. The goal is to achieve a tension-free, anatomically reduced repair with robust fixation to promote tendon-to-bone healing.
Portal Placement and Diagnostic Arthroscopy
- Posterior Portal : Established first, 1 cm inferior and 1 cm medial to the posterior angle of the acromion. Used for initial diagnostic arthroscopy of the glenohumeral joint.
- Anterior Portal : Typically anterosuperior, just lateral to the coracoid process, for working access to the anterior glenohumeral joint and subscapularis.
- Lateral Portal (Working) : Standard lateral portal, 2-3 cm lateral to the acromial border, used for shaver, burr, and anchor insertion in the subacromial space.
- Anterolateral Portal : Often used for anchor placement and suture management, providing an optimal angle for repair of the posterior cuff.
- Posterolateral Portal (Accessory) : May be used for specific pathologies or to improve working angles for posteromedial tears.
Diagnostic arthroscopy begins in the glenohumeral joint, systematically evaluating the glenoid, labrum, biceps tendon, humeral head, articular cartilage, and articular-sided rotator cuff. Any articular-sided partial tears are noted. The scope is then moved to the subacromial space after bursectomy.
Bursectomy and Debridement
The subacromial bursa, often inflamed and hypertrophic, is resected using an arthroscopic shaver. This allows for clear visualization of the entire rotator cuff, the greater tuberosity footprint, and the undersurface of the acromion. The tear margins are debrided back to healthy, bleeding tissue to optimize healing potential. Any associated subacromial spurs or osteophytes are debrided from the acromion to prevent impingement after repair, though an aggressive acromioplasty may not be necessary for acute tears without significant chronic impingement features.
Footprint Preparation
Preparation of the greater tuberosity footprint is crucial for robust tendon-to-bone healing. The insertion site is decorticated using an arthroscopic burr until punctate bleeding is observed, exposing cancellous bone. This provides a vascularized bed for tendon reattachment. Care is taken to avoid over-resection, which could compromise bone stock for anchor placement.
Tear Mobilization and Margin Convergence
Acute tears often have significant retraction due to muscle elasticity. The goal is to mobilize the tendon sufficiently to achieve a tension-free repair.
*
Adhesiolysis
: Release of adhesions from the undersurface of the cuff and the underlying capsule.
*
Interval Slide
: May be performed by releasing the posterior capsule and/or the rotator interval capsule, providing medialization of the cuff.
*
Margin Convergence
: For U-shaped or L-shaped tears, margin convergence sutures are placed perpendicular to the tear to close the defect medially, converting a larger tear into a smaller, more reparable tear prior to footprint fixation.
Reduction and Fixation
The technique of fixation aims to restore the anatomical footprint and achieve a strong, durable repair. The choice between single-row, double-row, or suture bridge techniques depends on tear size, morphology, tissue quality, and surgeon preference.
- Single-Row Repair : Involves placing anchors along the lateral aspect of the greater tuberosity, with sutures passed through the tendon and tied. Biomechanically less robust than double-row but simpler for small, well-mobilized tears.
- Double-Row Repair : Utilizes a medial row of anchors (e.g., in the footprint) and a lateral row of anchors (e.g., on the bone bridge or far lateral tuberosity). This creates a broader repair construct, restoring the anatomical footprint and providing a larger area of tendon-to-bone contact, which biomechanically has demonstrated higher load-to-failure strength and reduced gap formation.
-
Suture Bridge (Transosseous Equivalent) Repair
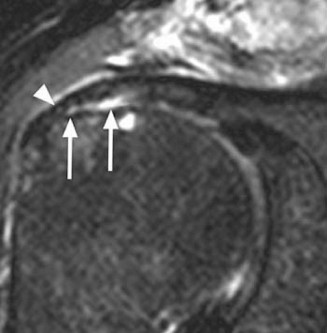
: A variation of double-row repair where a medial row of anchors secures the tendon, and the sutures are then passed through the tendon and tensioned over a bone bridge by fixation to a lateral row of anchors. This creates a "suture bridge" that compresses the tendon against the decorticated footprint, maximizing footprint coverage and contact pressure. It is considered biomechanically superior in many studies.

Figure 2: Arthroscopic view of a suture bridge rotator cuff repair construct, demonstrating broad tendon-to-bone contact at the footprint.
Steps for Fixation (Suture Bridge Example):
1.
Medial Anchor Placement
: Two or three medial anchors are placed approximately 8-10 mm medial to the lateral edge of the greater tuberosity, typically along the articular margin or slightly medial.
2.
Suture Passage
: Using suture passers (e.g., curved suture lasso, birdbeak), sutures from the medial anchors are retrieved and passed through the most medial portion of the rotator cuff tendon in a mattress or simple configuration.
3.
Knot Tying (Medial Row)
: The medial sutures are then tied using arthroscopic knot-tying techniques, securing the medial aspect of the tendon to the footprint. Non-absorbable sutures are standard.
4.
Lateral Anchor Placement & Tensioning
: The remaining free limbs of the medial sutures are then passed through the more lateral aspect of the tendon. A second row of anchors is placed more laterally on the greater tuberosity. The free suture limbs are then incorporated into these lateral anchors, tensioning the tendon down onto the entire prepared footprint, creating the "bridge." Knotless anchors are frequently used for the lateral row to simplify tensioning.
5.
Tear Assessment
: The repair is palpated with a probe to ensure a tension-free, anatomical reduction and adequate compression.
Concomitant Procedures
- Biceps Tenodesis/Tenotomy : Often performed for symptomatic biceps pathology (e.g., tendinopathy, instability, partial tears, fraying). Tenodesis aims to preserve biceps function and cosmesis by reattaching the tendon to the humerus (supra- or subpectoral), while tenotomy is a simpler division of the tendon, often preferred in elderly, low-demand patients.
- Superior Labral Repair : If a labral tear (SLAP lesion) is identified, it may be repaired, especially in younger patients.
- Debridement/Microfracture : For localized cartilage lesions.
Closure
After ensuring hemostasis, portals are closed with sutures or adhesive strips. A sterile dressing is applied, and the arm is immobilized in an abduction sling or pillow for post-operative protection.
Complications & Management
Despite advancements in surgical technique, complications can arise following arthroscopic rotator cuff repair. A proactive approach to identification and management is crucial for salvage and optimizing patient outcomes.
Common Complications and Management Strategies
| Complication | Incidence (approx.) | Etiology | Clinical Presentation | Salvage / Management Strategies |
|---|---|---|---|---|
| Re-Tear | 5-25% | Poor tissue quality, large tear, fatty infiltration, early motion, infection, non-healing. | Persistent pain, weakness, functional decline, loss of motion. | Conservative : PT, injections if asymptomatic. Surgical : Revision repair (if reparable), superior capsule reconstruction (SCR), allograft/autograft augmentation, latissimus dorsi transfer (LDT), reverse total shoulder arthroplasty (rTSA) for cuff tear arthropathy. |
| Stiffness / Arthrofibrosis | 5-20% | Inadequate rehabilitation, aggressive early motion in specific cases, underlying inflammatory conditions. | Decreased active and passive ROM, pain with motion. | Conservative : Intensive PT, judicious corticosteroid injections, MUA (Manipulation Under Anesthesia). Surgical : Arthroscopic capsular release. |
| Infection | <1% | Contamination during surgery, immunocompromised state. | Pain, redness, swelling, warmth, fever, purulent discharge. | Conservative : IV antibiotics for superficial infections. Surgical : Debridement, irrigation, retention of hardware if stable, removal of hardware if persistent/deep infection. |
| Nerve Injury | <1% (Suprascapular, Axillary, Musculocutaneous) | Traction injury, direct iatrogenic injury during portal placement or anchor insertion. | Weakness/paralysis of specific muscles, sensory deficits. | Conservative : Observation (most traction neuropraxias resolve), pain management, PT. Surgical : Neurolysis or nerve repair in specific cases (rare). |
| Deltoid Dehiscence | Rare | Aggressive lateral portal placement, inadvertent deltoid splitting, early aggressive deltoid activation. | Loss of deltoid contour, weakness in abduction, pain. | Surgical : Reattachment of deltoid origin to acromion. |
| Anchor Failure / Pullout | <1% | Poor bone quality (osteoporosis), inadequate purchase, excessive tension on repair. | Audible click/pop, acute pain, loss of repair integrity. | Surgical : Revision anchor placement, alternative fixation, conversion to open repair if necessary. |
| Post-operative Bleeding / Hematoma | <1% | Inadequate hemostasis, coagulopathy. | Swelling, bruising, pain, sometimes compartment-like symptoms. | Conservative : Compression, ice. Surgical : Drainage if large and symptomatic, identification and control of bleeding source. |
| Complex Regional Pain Syndrome (CRPS) | Rare | Idiopathic, post-traumatic or post-surgical, multifactorial. | Severe disproportionate pain, allodynia, hyperalgesia, swelling, vasomotor changes. | Conservative : Multidisciplinary approach: PT, occupational therapy, pain management (nerve blocks, medications), psychological support. |
Salvage Strategies for Failed Rotator Cuff Repair
When a primary rotator cuff repair fails, particularly in younger, active patients, salvage options must be carefully considered based on the specific failure mode, patient expectations, and remaining tissue quality.
- Revision Rotator Cuff Repair : If the re-tear is amenable to repair (good tissue quality, minimal retraction, acceptable fatty infiltration), a revision arthroscopic or open repair can be performed. This may involve different fixation techniques, additional mobilization, or augmentation.
- Superior Capsule Reconstruction (SCR) : For irreparable superior cuff tears, SCR using an allograft (e.g., dermal allograft) or autograft (e.g., fascia lata) aims to restore superior stability and prevent humeral head migration. It acts as a spacer, improving glenohumeral kinematics and pain, often without restoring full strength.
- Latissimus Dorsi Transfer (LDT) : Indicated for irreparable posterosuperior rotator cuff tears (infraspinatus, supraspinatus) in younger, active patients with intact subscapularis function and no significant glenohumeral arthritis. The LDT provides external rotation and abduction force.
- Pectoralis Major Transfer : Less common, primarily for irreparable subscapularis tears in younger, active patients.
- Reverse Total Shoulder Arthroplasty (rTSA) : The gold standard for symptomatic irreparable rotator cuff tears with associated cuff tear arthropathy. It bypasses the need for a functional rotator cuff by medializing the center of rotation and utilizing the deltoid to power elevation. It can also be considered in older patients with irreparable tears without significant arthritis but with persistent pain and loss of active elevation.
- Debridement/Partial Repair : For older, low-demand patients with irreparable tears, sometimes debridement of unstable tissue or a partial repair to achieve coverage can provide pain relief.
- Non-Operative Management : For asymptomatic re-tears or patients with significant comorbidities, a course of physical therapy, activity modification, and pain management remains a viable option.
Post-Operative Rehabilitation Protocols
A structured and progressive post-operative rehabilitation protocol is critical for optimizing outcomes following rotator cuff repair. The protocol is typically divided into phases, with progression based on biological healing timeframes and clinical milestones. Individual patient factors, tear size, and repair integrity influence the rate of progression.
Phase I: Protection and Passive Range of Motion (Weeks 0-6)
- Goals : Protect the repair, reduce pain and inflammation, prevent stiffness, maintain passive range of motion (PROM).
- Immobilization : Arm maintained in an abduction sling (often with a pillow or abduction wedge) continuously, except for hygiene and exercises. Sling removal duration is physician-dependent, typically for 4-6 weeks for most repairs, longer for massive or at-risk repairs.
-
Exercises (Daily)
:
- Pendulum exercises : Performed several times daily to encourage gentle motion and blood flow.
-
Passive Range of Motion (PROM)
: Performed by a therapist or with the unaffected arm.
- Forward flexion: To 90-120 degrees (depending on tear size/repair).
- External rotation: To 0-30 degrees (gradual progression).
- Internal rotation: To chest/abdomen.
- Scapular stabilization exercises : Isometric scapular squeezes (while in sling).
- Elbow, wrist, hand AROM : To prevent stiffness in uninvolved joints.
- Restrictions : No active range of motion (AROM) of the shoulder, no lifting, pushing, or pulling. Avoidance of external rotation beyond specified limits. No weight-bearing through the operative arm. No reaching behind the back.
Phase II: Early Active Motion and Light Strengthening (Weeks 6-12)
- Goals : Gradually increase AROM, initiate gentle strengthening, improve neuromuscular control.
- Sling Use : Typically weaned off the sling by 6 weeks, depending on pain and surgeon preference.
-
Exercises
:
- Active-Assisted Range of Motion (AAROM) : Pulleys, cane/stick exercises for forward flexion, external rotation, internal rotation.
- Active Range of Motion (AROM) : Gradually progress to full active range of motion as tolerated.
- Light Isometric Strengthening : Gentle isometric contractions for rotator cuff and deltoid, with arm at side.
- Scapular Stabilization : Wall slides, rows, prone extension.
- Biceps/Triceps Strengthening : Light weights or resistance bands for elbow flexion/extension.
- Restrictions : No heavy lifting or overhead activities. Avoid painful movements. No sudden movements or impact activities. External rotation beyond 45 degrees may still be restricted.
Phase III: Progressive Strengthening (Weeks 12-24)
- Goals : Restore full range of motion, significantly increase strength, improve endurance, prepare for higher-level activities.
-
Exercises
:
- Progressive Resistance Exercises (PREs) : Using resistance bands, light weights, and eventually machines. Focus on rotator cuff (internal/external rotation), deltoid (flexion, abduction), and scapular stabilizers.
- Proprioceptive Training : Rhythmic stabilization exercises, perturbation training.
- Functional Training : Incorporate movements related to daily activities and work requirements.
- Cardiovascular Endurance : Continue with non-impact activities.
- Restrictions : Gradual return to activities, emphasizing proper form and avoiding overexertion. Avoidance of high-impact or overhead sports until cleared.
Phase IV: Return to Activity / Sport-Specific Training (Months 6+)
- Goals : Maximize strength, power, and endurance. Return to full activity, including overhead sports or heavy labor.
-
Exercises
:
- Advanced Strengthening : Heavier weights, plyometrics (if appropriate), sport-specific drills.
- Interval Training : Gradually increase intensity and duration of activity.
- Maintenance Program : Lifelong home exercise program for strength and flexibility.
- Return to Sport/Work : Typically 6-12 months post-surgery, depending on the demands of the activity and successful achievement of functional milestones (e.g., 90-100% strength compared to contralateral side).
Key Considerations
- Individualization : Protocols must be tailored to the patient's tear size, tissue quality, age, activity level, and comorbidities. Massive tears or revision surgeries often require more conservative progression.
- Pain as a Guide : While pushing boundaries is necessary, pain should not be ignored. Progress within pain-free limits.
- Patient Education : Thoroughly educate patients on the rehabilitation process, expected timelines, and potential pitfalls. Compliance is paramount.
- Communication : Regular communication between the surgeon and physical therapist is essential to guide safe and effective progression.
Summary of Key Literature / Guidelines
The management of acute rotator cuff tears continues to evolve, with ongoing research refining surgical techniques, understanding healing biology, and optimizing rehabilitation protocols. Key literature and guidelines provide evidence-based recommendations for contemporary practice.
Early vs. Delayed Repair
There is a growing consensus that early surgical intervention for acute, symptomatic, full-thickness rotator cuff tears, particularly traumatic ones, yields superior outcomes compared to delayed repair or non-operative management. Several studies have demonstrated that delaying repair leads to increased tear retraction, muscle atrophy, fatty infiltration, and subsequent difficulty in achieving a tension-free repair, resulting in higher re-tear rates and poorer functional results. Maman et al. (2018) published a meta-analysis supporting early surgical repair for acute traumatic rotator cuff tears.
Single-Row vs. Double-Row vs. Suture Bridge Repair
The debate regarding the optimal fixation technique has been a cornerstone of rotator cuff research.
*
Biomechanically
,
double-row and suture bridge (transosseous equivalent) repairs consistently demonstrate superior load-to-failure strength, increased footprint contact area, and reduced gap formation
compared to single-row repairs. This has been shown in numerous cadaveric and in-vivo studies (e.g., Park et al., 2007; Meier et al., 2008).
*
Clinically
, systematic reviews and meta-analyses have shown a
trend towards lower re-tear rates with double-row and suture bridge techniques
, especially for larger tears. However, for small-to-medium tears, some studies have shown no significant clinical difference in functional outcomes or pain scores between single-row and double-row repairs (DeHaan et al., 2012; Ma et al., 2018). The decision often hinges on tear size, tissue quality, and surgeon preference. For acute tears, optimizing the biomechanical environment for healing is crucial, favoring constructs that maximize footprint coverage and compression.
Biologic Augmentation
The use of biologic augmentation (e.g., platelet-rich plasma (PRP), mesenchymal stem cells (MSCs), extracellular matrices/scaffolds) is an active area of research to improve tendon-to-bone healing and reduce re-tear rates. While promising, current evidence for the routine use of PRP or MSCs in primary rotator cuff repair is mixed and not universally supported by high-level evidence (Kwong et al., 2017; Hurley et al., 2019). Some studies suggest potential benefits in specific patient populations or tear types, but more robust, large-scale randomized controlled trials are needed. Acellular dermal matrices or synthetic scaffolds are typically reserved for revision cases or repair of massive, irreparable tears.
Rehabilitation Protocols
Evidence-based rehabilitation protocols emphasize initial protection followed by a gradual, progressive increase in motion and strengthening . While the duration of immobilization remains a point of contention, particularly for smaller tears, the principle of allowing adequate biological healing time (typically 6-12 weeks for soft tissue-to-bone integration) is paramount. Recent studies have explored accelerated rehabilitation protocols for smaller tears, demonstrating comparable outcomes to more traditional protocols, but careful patient selection is essential to avoid re-tear (Koh et al., 2016). Guidelines from organizations like the American Academy of Orthopaedic Surgeons (AAOS) provide general recommendations, but emphasize the need for individualization based on surgical findings and patient factors.
Management of Irreparable Tears
For massive, irreparable rotator cuff tears, particularly in younger, active patients without significant glenohumeral arthritis, superior capsule reconstruction (SCR) and tendon transfers (e.g., latissimus dorsi transfer) have emerged as viable salvage options. SCR has demonstrated good early and mid-term results in pain relief and improved function, especially in preventing superior humeral head migration (Mihata et al., 2013). For older patients with irreparable tears and cuff tear arthropathy, reverse total shoulder arthroplasty (rTSA) remains the gold standard, providing reliable pain relief and restoration of active elevation (Boileau et al., 2005).
In conclusion, the contemporary management of acute rotator cuff tears emphasizes accurate and timely diagnosis, followed by a carefully planned surgical repair strategy utilizing advanced arthroscopic techniques, robust fixation constructs, and a structured, individualized rehabilitation program. Continued research will undoubtedly further refine our understanding and treatment algorithms for this common and challenging condition.
Clinical & Radiographic Imaging