PATHOPHYSIOLOGY AND PRINCIPLES OF UPPER EXTREMITY SEPTIC ARTHRITIS
Septic arthritis of the upper extremity is an orthopedic emergency characterized by the rapid, destructive invasion of the synovial joint space by pyogenic organisms. The presence of purulent exudate within a closed joint cavity initiates a catastrophic cascade of cartilage degradation, driven by bacterial toxins and host-derived proteolytic enzymes (metalloproteinases). If left untreated, this results in irreversible chondrolysis, joint subluxation, and profound functional impairment.
The epidemiology and etiology of shoulder and elbow sepsis exhibit a distinct bimodal distribution. In pediatric populations, acute septic arthritis of the shoulder is frequently a direct complication of hematogenous osteomyelitis of the proximal humeral metaphysis. Because the proximal humeral metaphysis is intra-articular, cortical breakthrough of a metaphyseal abscess rapidly contaminates the glenohumeral joint. Conversely, in adult populations, septic arthritis of the shoulder or elbow rarely occurs in young, healthy individuals. It is predominantly associated with debilitating systemic diseases, immunosuppression, intravenous drug abuse, or end-stage renal disease, and it notoriously demonstrates a recalcitrant response to conservative treatment.
Early diagnostic arthrocentesis (aspiration) is mandatory whenever an intra-articular infection is suspected. If frank purulence is obtained, or if synovial fluid analysis reveals a white blood cell (WBC) count exceeding 50,000 cells/mm³ with a polymorphonuclear (PMN) predominance (>90%), emergent surgical drainage is indicated. Advanced imaging, such as Computed Tomography (CT) or Magnetic Resonance Imaging (MRI), serves as a critical adjunct to delineate the extent of osseous involvement, identify loculated periarticular abscesses, and guide surgical planning.
THE SHOULDER JOINT: DIAGNOSIS AND ASPIRATION
The glenohumeral joint is a deeply situated, highly mobile articulation. Clinical signs of sepsis may be masked by the robust muscular envelope of the deltoid and rotator cuff. Patients typically present with severe, unrelenting pain exacerbated by micromotion, and the limb is often held in a position of adduction and internal rotation to maximize capsular volume and minimize intra-articular pressure.
Aspiration of the Shoulder
The shoulder may be aspirated via anterior, posterior, or lateral approaches. However, the anterior approach is overwhelmingly preferred. The anterior capsule is often the site of maximal fluctuance, and the anterior bony landmarks are more readily palpable, even in obese or muscular patients.
Technique for Anterior Shoulder Aspiration:
1. Position the patient supine or in a semi-Fowler position.
2. Identify the coracoid process medially and the anterolateral edge of the acromion laterally.
3. The optimal aspiration site is located exactly half the distance between these two bony landmarks.
4. After meticulous sterile skin preparation and local anesthesia, introduce an 18-gauge needle at this midpoint.
5. Direct the needle strictly posteriorly through the deltoid musculature and the anterior joint capsule.
6. Aspirate the joint while applying gentle negative pressure.
Clinical Pearl: If bone is encountered prematurely during anterior aspiration, the needle has likely struck the lesser tuberosity or the humeral head. Withdraw the needle slightly, redirect it slightly medially toward the glenoid articular surface, and advance again.
SURGICAL DRAINAGE OF THE SHOULDER
The shoulder may be drained through an open anterior incision, an open posterior incision, or via arthroscopy. Historically, Leslie et al. demonstrated that formal arthrotomy yields vastly superior clinical outcomes compared to serial needle aspirations, particularly in adult patients with established purulence. Today, the anterior approach remains the workhorse for open drainage due to its direct access to the dependent recesses of the joint and the biceps tendon sheath.
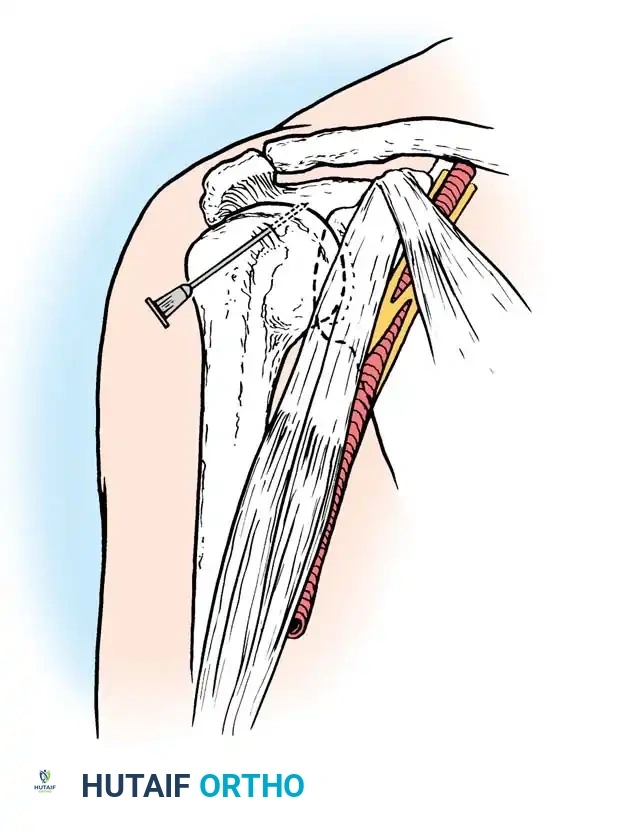
Anterior Drainage Technique (Open Arthrotomy)
The anterior approach utilizes a deltoid-splitting technique to gain rapid access to the anterior capsule.
- Incision: Begin an anterior longitudinal incision at the anterior border of the acromion. Extend the incision 5 to 7.5 cm distally over the center of the humeral head, following the orientation of the anterior deltoid fibers.
- Superficial Dissection: Split the fibers of the deltoid muscle bluntly.
- Deep Dissection: Identify the subscapularis tendon. Divide the subscapularis tendon transversely or split it in line with its fibers to expose the underlying underlying joint capsule. Open the capsule under direct vision.
- Evacuation and Debridement: Evacuate the purulent fluid. Crucially, open the synovial sheath of the long head of the biceps tendon, as this is a frequent site of bacterial loculation. Irrigate the joint copiously with several liters of sterile saline.
- Pediatric Consideration: In children, if concomitant osteomyelitis is suspected, drill the proximal humeral metaphysis to decompress any intraosseous abscess.
- Closure: Leave the capsule open. Close the subcutaneous tissue and skin loosely over large-bore suction drains to prevent reaccumulation of fluid.
Surgical Warning: When splitting the deltoid muscle, never extend the split further than 5 cm distal to the lateral edge of the acromion. Extending beyond this safe zone risks transecting the terminal branches of the axillary nerve, resulting in catastrophic denervation of the anterior deltoid. Furthermore, when drilling the pediatric metaphysis, meticulous care must be taken to avoid violating the proximal humeral physis to prevent future growth arrest.
Posterior Drainage Technique
The posterior approach is less commonly utilized but is indicated when preoperative imaging demonstrates a predominantly posterior abscess or when posterior capsular loculations cannot be adequately addressed anteriorly.
- Incision: Begin the incision at the base of the spine of the scapula. Extend it distally and laterally for 7.5 cm, perfectly in line with the fibers of the posterior deltoid muscle.
- Superficial Dissection: Split the fibers of the posterior deltoid to expose the underlying external rotators of the shoulder (infraspinatus and teres minor).
- Deep Dissection: Develop the internervous plane between the infraspinatus (suprascapular nerve) and the teres minor (axillary nerve) just medial to the greater tuberosity of the humerus.
- Evacuation: Incise the posterior capsule and evacuate the pus.
- Closure: Irrigate the joint with copious amounts of saline, and close the skin loosely over drains.
Arthroscopic Drainage of the Shoulder
Arthroscopic drainage has rapidly become the gold standard for the treatment of acute septic arthritis of the shoulder in institutions with appropriate expertise. Arthroscopy offers several distinct biomechanical and physiological advantages over open arthrotomy.
With arthroscopy, thorough washout is performed under direct, magnified vision, ensuring the complete removal of purulent material from all joint recesses (including the axillary pouch and subscapularis recess). Fibrinous loculations and adhesions can be mechanically debrided, and a comprehensive synovectomy can be performed with motorized shavers.
Standard anterior and posterior portals are utilized. Drains can be seamlessly placed through these portal sites at the conclusion of the procedure. Because the rotator cuff and deltoid insertions are preserved, early active mobilization can be initiated much sooner than with an open technique, significantly reducing the risk of postoperative adhesive capsulitis.
Postoperative Rehabilitation Protocol (Shoulder)
Following open drainage, the shoulder is supported in a specialized splint or orthosis at 45 degrees of abduction until the surgical wound has adequately healed. This position prevents contracture of the inferior capsule (axillary fold). Once the wound is stable and clinical signs of infection are resolving, active and active-assisted range-of-motion exercises are aggressively initiated to restore glenohumeral kinematics.
THE ELBOW JOINT: DIAGNOSIS AND ASPIRATION
Septic arthritis of the elbow presents with a swollen, erythematous, and exquisitely tender joint. The elbow is typically held in 70 to 80 degrees of flexion, as this is the position of maximum capsular capacity, accommodating the highest volume of purulent effusion with the least intra-articular pressure.
Aspiration of the Elbow
The elbow joint is most safely and effectively aspirated via a direct lateral or posterolateral approach, utilizing the anconeus triangle (the "triangle of safety").
Technique for Elbow Aspiration:
1. Flex the patient's elbow to 90 degrees.
2. Identify the lateral epicondyle, the radial head, and the tip of the olecranon. These three landmarks form the anconeus triangle.
3. Insert the needle on the posterior aspect of the joint, just lateral to the olecranon and proximal to the radial head.
4. Advance the needle medially and slightly anteriorly through the skin and joint capsule until synovial fluid is obtained.
SURGICAL DRAINAGE OF THE ELBOW
The elbow is a complex, highly constrained hinge joint with multiple distinct compartments. It is best drained through a medial approach, a lateral approach, or a combination of both, depending on the extent of the infection. Posterior drainage is also an excellent option for global joint decompression.
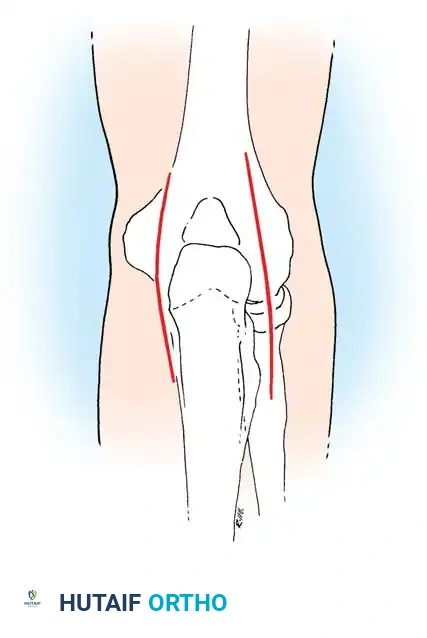
Medial Drainage Technique
The medial approach provides excellent access to the medial joint capsule but requires meticulous neurovascular dissection.
- Incision: Make a longitudinal incision centered over the medial humeral epicondyle. Extend it 5 cm proximally along the medial supracondylar ridge and 2.5 cm distally.
- Superficial Dissection: Develop the interval between the triceps muscle posteriorly (radial nerve) and the brachialis muscle anteriorly (musculocutaneous nerve).
- Deep Dissection: Elevate the periosteum laterally and distally off the anterior humerus until the medial joint capsule is fully exposed.
- Evacuation: Incise the capsule longitudinally and evacuate the purulence.
- Closure: Irrigate the joint with saline, and close the skin loosely over drains.
Surgical Warning: The ulnar nerve is at extreme risk during the medial approach. It must be identified early as it courses posterior to the medial epicondyle in the cubital tunnel. It should be gently retracted and protected throughout the entirety of the procedure.
Lateral Drainage Technique
The lateral approach is often preferred for its relative safety and direct access to the radiocapitellar joint.
- Incision: Make a longitudinal incision centered over the lateral humeral epicondyle, extending 5 cm proximally and 2.5 cm distally.
- Superficial Dissection: Separate the triceps muscle posteriorly from the extensor carpi radialis longus (ECRL) anteriorly to expose the joint capsule.
- Deep Dissection: Dissect strictly subperiosteally, remaining close to the bone. Incise the capsule, evacuate the pus, and irrigate the joint.
- Posterior Extension: The posterior compartment of the joint may also be drained through this single lateral incision by dissecting posteriorly along the humerus and elevating the lateral attachment of the triceps from the bone.
- Closure: Close the skin loosely over drains.
Pitfall: Straying anteriorly from the subperiosteal plane during the lateral approach places the radial nerve at significant risk as it pierces the lateral intermuscular septum and courses anterior to the lateral epicondyle.
Posterior Drainage Technique
The posterior approach allows for bilateral access to the posterior compartment and the olecranon fossa, which is highly effective for severe, global elbow sepsis.
- Incision: Begin parallel longitudinal incisions on each side of the olecranon, and continue them proximally for 7.5 cm along the medial and lateral borders of the triceps.
- Deep Dissection: Deepen the incisions directly through the medial and lateral borders of the triceps aponeurosis, entering the posterior compartment of the joint.
- Evacuation: Decompress the olecranon fossa, evacuate all fibrinous debris, and irrigate copiously. Avoid injuring the ulnar nerve as it crosses the posterior aspect of the medial humeral epicondyle during the medial-sided dissection.
Postoperative Rehabilitation Protocol (Elbow)
Postoperatively, the elbow is splinted at 90 degrees of flexion with the forearm in neutral rotation. This position balances capsular tension and provides optimal stability. The splint is maintained until the surgical wound has healed and the acute inflammatory phase has subsided. Subsequently, active range-of-motion exercises are initiated to prevent the rapid onset of elbow stiffness, which is a notorious complication of elbow joint infections.
THE WRIST JOINT: ASPIRATION AND DECOMPRESSION
While less common than shoulder or elbow sepsis, septic arthritis of the wrist requires equally aggressive management. The radiocarpal joint is a complex, multi-articulating space that can rapidly undergo chondrolysis if decompression is delayed.
Aspiration of the Wrist
The wrist is most safely and effectively aspirated via a dorsal approach, avoiding the complex neurovascular structures of the volar wrist (median nerve, ulnar nerve, radial and ulnar arteries).
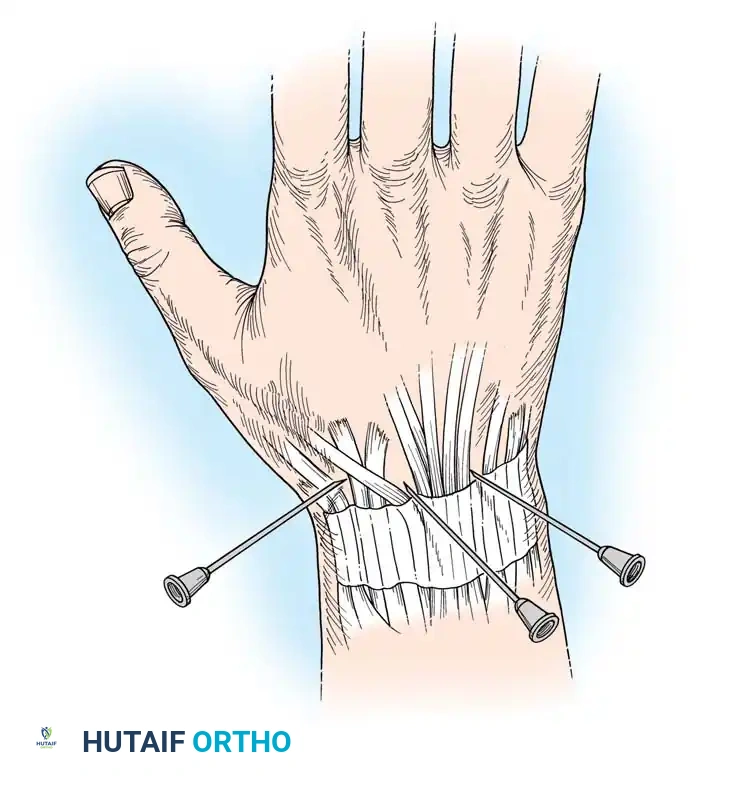
Technique for Dorsal Wrist Aspiration:
1. Palpate Lister's tubercle on the dorsal aspect of the distal radius.
2. Identify the extensor pollicis longus (EPL) tendon, which angles radially around Lister's tubercle.
3. Identify the extensor digitorum communis (EDC) tendons slightly ulnar to the EPL.
4. The optimal aspiration site is the palpable depression between the EPL and the EDC, just distal to the radiocarpal joint line.
5. Insert the needle dorsally, directing it slightly volarward and proximally to enter the radiocarpal articulation.
If purulence is confirmed upon aspiration, the patient must be taken emergently to the operating room for formal dorsal arthrotomy or wrist arthroscopy. Open drainage typically utilizes a dorsal longitudinal incision centered over Lister's tubercle, opening the third extensor compartment, retracting the EPL radially, and performing a longitudinal capsulotomy to thoroughly evacuate the radiocarpal and midcarpal joints. Postoperatively, the wrist is splinted in slight extension to preserve functional grip strength during the healing phase.
