INTRODUCTION TO FEMORAL SHAFT FRACTURES
Fractures of the shaft of the femur are among the most common and biomechanically demanding injuries encountered in acute orthopaedic trauma practice. As the largest and strongest bone in the human body, the femur serves as the principal load-bearing strut of the lower extremity. Consequently, diaphyseal fractures of the femur typically result from high-energy mechanisms—such as motor vehicle collisions, motorcycle accidents, or falls from significant heights—and are frequently associated with multisystem polytrauma.
Without prompt and biomechanically sound intervention, these fractures can lead to prolonged morbidity, extensive disability, and life-threatening systemic complications, including fat embolism syndrome and acute respiratory distress syndrome (ARDS).
The modern orthopaedic surgeon must possess a comprehensive armamentarium of fixation techniques. The selection of the optimal treatment modality is multifactorial, dictated by the fracture morphology, location, degree of comminution, soft-tissue envelope integrity, patient age, and the presence of concomitant systemic injuries.
Core Principles of Management
Regardless of the specific fixation modality selected, the definitive management of femoral shaft fractures must adhere to three universally accepted orthopaedic principles:
1. Restoration of Anatomy: Precise restoration of axial alignment, rotation, and limb length.
2. Biological Preservation: Meticulous handling of the soft-tissue envelope to preserve the periosteal and endosteal blood supply, thereby optimizing the biological environment for fracture union and minimizing infection risk.
3. Early Rehabilitation: Achieving construct stability that permits early mobilization of the patient and the affected extremity, mitigating the complications of prolonged recumbency.
EVOLUTION OF TREATMENT MODALITIES
Historically, the management of femoral shaft fractures relied heavily on non-operative techniques. Today, these methods are largely relegated to temporizing roles or highly specific pediatric populations.
Traction and Cast Immobilization
Skeletal traction (e.g., balanced skeletal traction or roller traction) and spica cast immobilization are rarely, if ever, utilized as definitive treatment in the adult population. Currently, skeletal traction via a proximal tibial or distal femoral pin serves primarily as a preliminary, damage-control phase. It maintains length and alignment temporarily before definitive surgical intervention, such as closed intramedullary nailing or plate osteosynthesis.
Clinical Pearl: The historical reliance on prolonged bed rest and skeletal traction carried unacceptably high rates of deep vein thrombosis (DVT), pulmonary embolism, decubitus ulcers, and pulmonary compromise. The economic and physiological consequences of weeks of hospital confinement make non-operative management obsolete for adult femoral diaphyseal fractures.
External Fixation
External fixation is a critical tool in the context of "Damage Control Orthopaedics" (DCO). For the hemodynamically unstable polytrauma patient, or in the presence of severe Type III open fractures with massive soft-tissue stripping and contamination, rapid application of a spanning external fixator provides immediate skeletal stability. This minimizes ongoing soft-tissue trauma and blood loss while allowing for aggressive resuscitation. Once the patient's physiological parameters normalize, the external fixator is typically converted to a definitive internal construct (usually an intramedullary nail) within 2 to 3 weeks to minimize the risk of pin-tract infections seeding the medullary canal.
INTRAMEDULLARY NAILING: THE GOLD STANDARD
Locked intramedullary (IM) nailing is currently universally recognized as the treatment of choice for the vast majority of closed, and many open, femoral shaft fractures.
Biomechanics of Intramedullary Fixation
IM nails function as load-sharing devices. By residing within the neutral axis of the bone, they are subjected to significantly lower bending moments compared to eccentrically placed plates. This biomechanical advantage allows for early weight-bearing. Furthermore, closed IM nailing preserves the fracture hematoma and the periosteal blood supply, providing an optimal osteogenic environment for secondary bone healing via callus formation.
Options include:
* Antegrade Interlocking Nailing: Inserted via the piriformis fossa or greater trochanter. It is the most common approach but carries a risk of heterotopic ossification and abductor weakness.
* Retrograde Interlocking Nailing: Inserted via the intercondylar notch of the distal femur. Highly advantageous in ipsilateral femoral neck/shaft fractures, floating knee injuries, or morbidly obese patients.
* Reamed vs. Unreamed: Reaming generates autologous bone graft within the canal and allows for the insertion of a larger diameter, biomechanically stiffer nail.
PLATE OSTEOSYNTHESIS OF THE FEMUR
While IM nailing is the gold standard, Open Reduction and Internal Fixation (ORIF) utilizing plate osteosynthesis remains an indispensable technique for specific indications.
Indications for Plating
- The Polytraumatized Patient with Pulmonary Compromise: Reaming and inserting an IM nail pressurizes the medullary canal, releasing marrow fat and inflammatory mediators into the venous circulation. In patients with severe chest trauma or impending ARDS, this "second hit" can be fatal. Plating avoids canal pressurization.
- Narrow Medullary Canal: Patients with congenital anomalies or excessively narrow canals that cannot accommodate an IM nail.
- Peri-prosthetic Fractures: Fractures occurring around existing hip or knee arthroplasty stems.
- Vascular Injury: Fractures requiring simultaneous extensile exposure for arterial repair.
Surgical Warning: Seligson et al. demonstrated that while femoral plating in polytrauma patients significantly reduces the postoperative morbidity associated with ARDS compared to IM nailing, it carries a higher rate of fracture healing complications (30% for plating vs. 12% for nailing). Meticulous surgical technique is paramount to mitigate nonunion risks.

FIGURE 54-79: Polytraumatized patient with extensive pulmonary injuries and a femoral diaphyseal fracture treated with ORIF using large fragment compression plating to avoid medullary pressurization.
Biomechanics and Plate Selection
When plate and screw fixation is indicated, the 4.5-mm broad Dynamic Compression Plate (DCP) or Low-Contact Dynamic Compression Plate (LC-DCP) is preferred.
Unlike IM nails, plates are load-bearing devices (until the fracture heals) and are placed eccentrically on the tension band surface (the lateral cortex of the femur).
* Working Length: The plate must be sufficiently long to distribute stress. The general rule is to achieve a minimum of eight cortices (four bicortical screws) of purchase on either side of a transverse or short oblique fracture.
* Biological Plating: Traditional rigid AO plating devitalizes the underlying cortical bone due to periosteal compression. The advent of the LC-DCP, featuring scalloped recesses on its undersurface, permits less iatrogenic insult to the periosteal blood supply, thereby reducing the risk of deep infection and nonunion.
Surgical Approach: The Anterolateral Exposure
Plating of the femoral shaft is typically performed via an anterolateral approach, which provides safe, extensile access to the diaphysis.
- Positioning: The patient is positioned supine on a radiolucent flat table. A bump is placed under the ipsilateral hip to internally rotate the leg to a neutral position. Unlike closed IM nailing, plating does not require an unwieldy fracture table, though a fluoroscopic image intensifier remains highly beneficial.
- Incision: A longitudinal incision is made along the line connecting the anterior superior iliac spine (ASIS) to the lateral border of the patella.
- Superficial Dissection: The subcutaneous tissue is divided to expose the iliotibial tract, which is incised longitudinally.
- Deep Dissection: The vastus lateralis is identified. The approach exploits the plane between the rectus femoris and the vastus lateralis. The vastus lateralis is elevated from the linea aspera posteriorly.
- Vascular Management: Crucial Step. As the vastus lateralis is elevated, the surgeon will encounter multiple perforating branches of the profunda femoris artery. These must be meticulously isolated, ligated, or coagulated to prevent massive postoperative hematoma.
Technique of Plate Fixation
- Fracture Reduction: The fracture is exposed, and the hematoma is carefully evacuated. Anatomical reduction is achieved using bone reduction forceps.
- Interfragmentary Compression: For oblique or spiral fracture patterns, absolute stability is achieved by placing independent interfragmentary lag screws across the fracture plane before plate application.
- Plate Application: A pre-contoured 4.5-mm broad DCP or LC-DCP is applied to the lateral cortex.
- Screw Insertion: A minimum of four, preferably five, bicortical screws are placed proximal and distal to the fracture zone. If the distal bone is osteoporotic, 6.5-mm cancellous screws may be utilized in the distal metaphyseal segment to improve purchase.
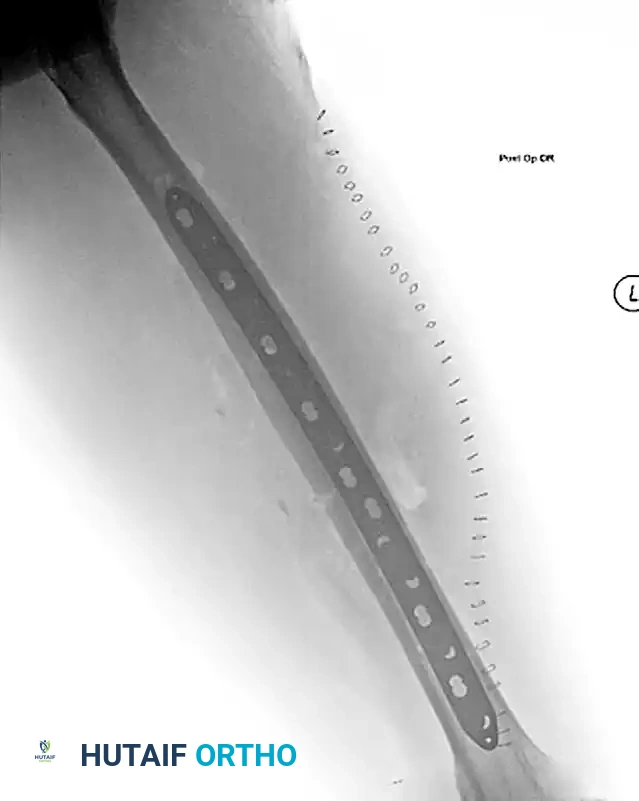
FIGURE 54-80A: Lateral radiographic view demonstrating a femoral shaft fracture stabilized with a broad plate and interfragmentary lag screws.

FIGURE 54-80B: Anteroposterior radiographic view of the same femoral shaft fracture, highlighting the restoration of axial alignment and the utilization of the 8-cortex rule proximal and distal to the fracture site.
COMPLICATIONS AND HARDWARE MANAGEMENT
Infection and Nonunion
While plating preserves the endosteal blood supply, the extensive soft-tissue stripping required for exposure increases the risk of infection and nonunion compared to closed nailing. In historical cohorts, deep infection rates hovered around 2% for severe open fractures (Type IIIC) treated with plates, though deep infections in closed fractures remain exceedingly rare with modern sterile techniques and prophylactic antibiotics.
Stress Shielding and Plate Removal
A significant biomechanical consequence of rigid plate fixation is "stress shielding." According to Wolff's Law, bone remodels in response to the mechanical stresses placed upon it. A rigid AO plate absorbs the majority of the physiological load, causing the underlying cortical bone to remodel and become osteopenic, resembling cancellous bone in its structural integrity.
Guidelines for Plate Removal:
* Timing: Plates can be safely removed 2 to 3 years post-injury, provided that radiographic and clinical union is absolute. However, routine plate removal is not recommended unless the patient is highly symptomatic (e.g., hardware irritation, cold intolerance).
* Rehabilitation Post-Removal: Because the underlying cortex is mechanically weakened, stress must be gradually reapplied. The bone must be protected from excessive torsional or bending stresses for at least 6 weeks following hardware removal to prevent catastrophic refracture.
* Orthogonal Plating Considerations: In complex distal diaphyseal/metaphyseal fractures where two plates have been placed at 90 degrees to each other (orthogonal plating), never remove both plates simultaneously. The bone is doubly weakened by the stress shielding and the empty screw holes, making refracture highly likely. The recommended protocol is staggered removal: the second plate should be removed a minimum of 6 months after the first.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative rehabilitation trajectory differs significantly depending on the fixation modality utilized.
Following Intramedullary Nailing:
Because the IM nail is a load-sharing device located at the mechanical axis, patients are typically allowed immediate weight-bearing as tolerated (WBAT), assuming no concomitant injuries preclude it. Early mobilization accelerates callus formation via micromotion at the fracture site.
Following Plate Osteosynthesis:
Plates are load-bearing devices placed eccentrically. Immediate unprotected weight-bearing is generally contraindicated, as it risks catastrophic hardware failure (plate bending or screw pullout) before biological union occurs.
* 0-6 Weeks: Toe-touch weight-bearing (TTWB) or partial weight-bearing (PWB) with crutches or a walker. Aggressive early range of motion (ROM) of the hip and knee is instituted to prevent arthrofibrosis and quadriceps tethering.
* 6-12 Weeks: Progression to full weight-bearing is permitted only after radiographic evidence of bridging callus is observed.
CONCLUSION
The management of femoral shaft fractures requires a nuanced understanding of biomechanics, systemic physiology, and surgical anatomy. While locked intramedullary nailing represents the pinnacle of treatment for the majority of these injuries, plate osteosynthesis remains a vital, life-saving technique in the polytraumatized patient. By adhering to strict biomechanical principles—ensuring adequate working length, respecting the soft-tissue envelope, and implementing appropriate postoperative rehabilitation—the orthopaedic surgeon can consistently achieve excellent functional outcomes and minimize the profound morbidity historically associated with these severe injuries.
