Comprehensive Management of Hallux Sesamoid Injuries: Diagnosis and Surgical Techniques
Key Takeaway
Hallux sesamoid injuries encompass a spectrum of pathologies, including sesamoiditis, fractures, and osteochondritis dissecans. The tibial sesamoid is most frequently affected due to its central weight-bearing position. Accurate diagnosis relies on localized palpation and specialized axial and oblique radiographs. While conservative management with orthoses and activity modification is the first-line approach, refractory cases may require meticulous surgical excision, carefully preserving the flexor hallucis longus and proper digital nerves to optimize functional outcomes.
INTRODUCTION TO HALLUX SESAMOID PATHOLOGY
The clinical recognition of hallux sesamoid pathology has expanded significantly, particularly within the realms of sports medicine and advanced foot and ankle surgery. While acute injuries to the sesamoids—such as those sustained during high-impact sports activities or falls from heights—are typically recognized quickly, more subtle, insidious pathological conditions frequently escape initial diagnosis.
Chronic inflammatory conditions of a traumatic, infectious, or arthritic origin are broadly grouped under the umbrella diagnosis of sesamoiditis. However, this term often oversimplifies a complex array of underlying issues. Inflamed bursae, intractable plantar keratoses (IPK), or diffuse callus formation beneath the tibial sesamoid may herald severe underlying structural or biomechanical sesamoid pathology. Furthermore, the sesamoids are susceptible to a myriad of specific conditions, including chondromalacia, flexor hallucis brevis (FHB) tendinitis, osteochondritis dissecans (OCD), and acute or stress fractures.
Anatomy and Biomechanics
The hallucal sesamoids are embedded within the tendons of the flexor hallucis brevis. They serve several critical biomechanical functions:
* Mechanical Advantage: They act as a fulcrum, increasing the mechanical advantage and flexion moment of the FHB.
* Friction Reduction: They protect the flexor hallucis longus (FHL) tendon as it glides between them.
* Load Distribution: They absorb and dissipate weight-bearing forces transmitted through the first ray during the push-off phase of gait.
The tibial (medial) sesamoid is the most commonly injured of the two. This vulnerability is due to its central location directly beneath the first metatarsal head, subjecting it to immense axial loading. Hyperextension of the first metatarsophalangeal (MTP) joint combined with axial loading is the most common mechanism of injury, frequently resulting in a fracture or a severe sprain of the capsuloligamentous complex.
Clinical Pearl: Repetitive stress through a syndesmotic union of a bipartite sesamoid can weaken the fibrocartilaginous junction. Over time, this microtrauma can culminate in a displaced "fracture" through the synchondrosis, a condition that is notoriously resistant to conservative healing.
CLINICAL EVALUATION AND DIAGNOSTIC IMAGING
Physical Examination
On physical examination, patients often present with diffuse tenderness around the first MTP joint, which can mimic other conditions such as gout, hallux rigidus, or turf toe. However, with meticulous, targeted palpation of each individual sesamoid, the tenderness usually becomes highly localized.
Any patient complaining of pain around the plantar aspect of the first MTP joint must undergo a thorough, systematic evaluation of the sesamoids. Assess for pain with passive dorsiflexion of the hallux (which stretches the FHB complex) and evaluate the plantar skin for hyperkeratotic lesions or bursal thickening.
Radiographic Evaluation
Routine radiographs, including standard anteroposterior (AP) and oblique views, are the initial steps in imaging.


Fig. 78-95 A, Standing anteroposterior view of both feet on the same cassette allows comparison of the sesamoids. This is especially helpful if a fracture is suspected but a bipartite sesamoid is present. Accessory sesamoids (arrows) are a normal, although uncommon, finding. B, Oblique view profiles the fibular sesamoid. Note the cystic fibular sesamoid on the right foot. This probably represents an old fracture through the syndesmotic union of a bipartite sesamoid.
The standard lateral view of the foot is usually obscured by the lesser metatarsals and is rarely revealing for sesamoid pathology. Therefore, specialized views are mandatory:
1. The Medial Oblique (Sesamoid) View: Highly effective for evaluating the tibial sesamoid in profile.
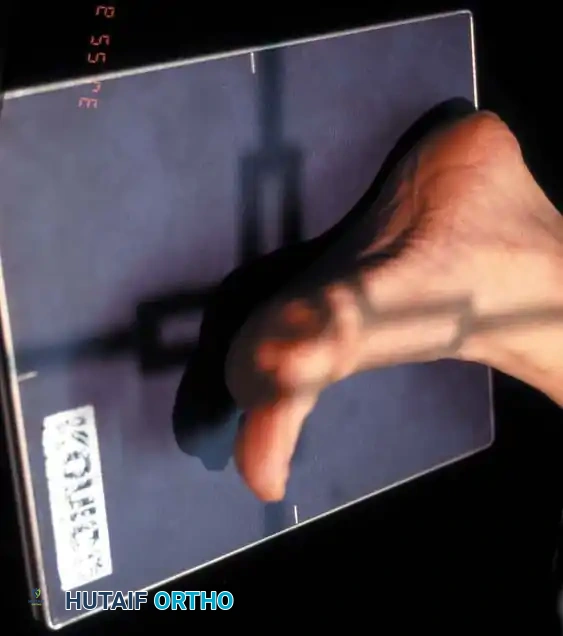

Fig. 78-96 Tibial sesamoid is profiled on the medial oblique view. A, Position of the foot. B, Sesamoid in profile.
2. The Axial Sesamoid View: This view should always be obtained if a sesamoid pathological condition is suspected. It provides a tangential view of the sesamoid-metatarsal articulation, revealing joint space narrowing, subluxation, or fractures.
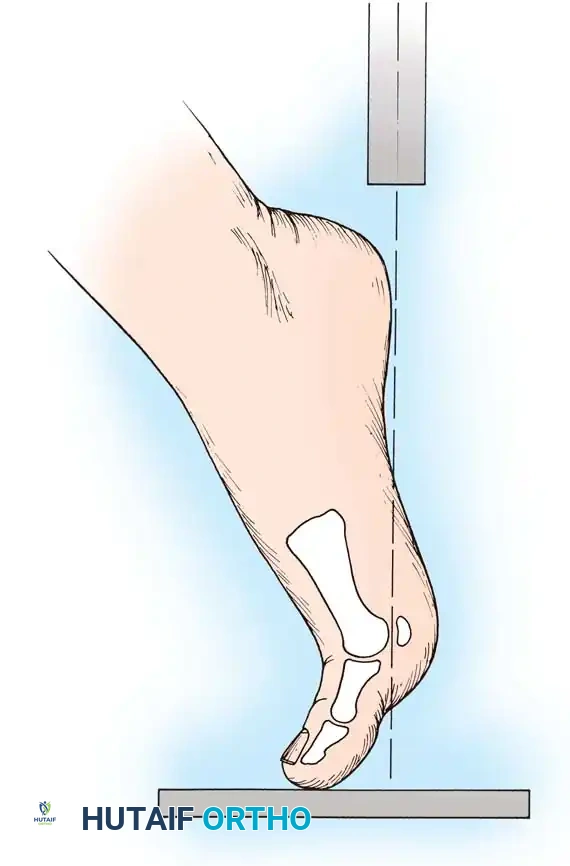
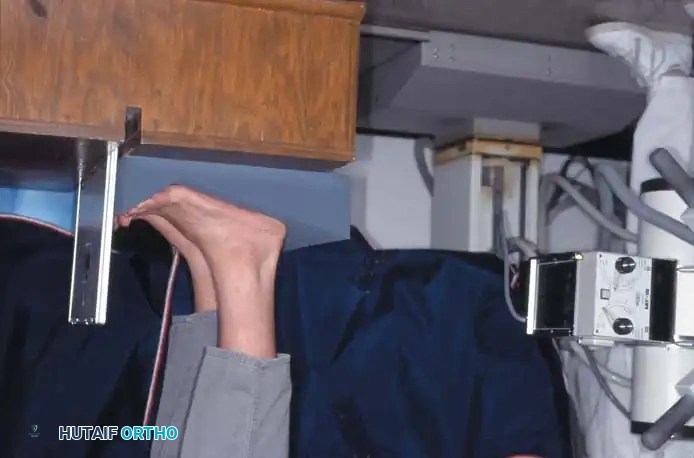
Fig. 78-97 Hallux valgus (A), and on axial sesamoid view (B), degenerative changes present with subluxation of the sesamoids.

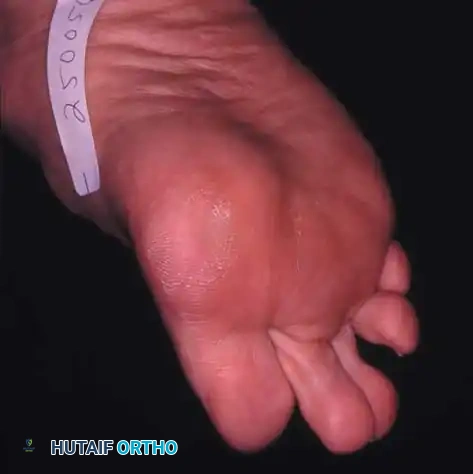
Fig. 78-98 Techniques for obtaining axial sesamoid views. A and B, View may be taken with the patient up on toes (A) or standing on an inclined plane (B). C and D, Axial sesamoid view taken from the front while the patient stands on an inclined plane.
Advanced Imaging and the Bipartite Sesamoid Dilemma
If radiographic views are normal but clinical suspicion remains high, a technetium-99m bone scan or Magnetic Resonance Imaging (MRI) is indicated. When ordering a bone scan, the nuclear medicine department must be explicitly informed that the sesamoids are the area of interest so projections can be modified accordingly. MRI is particularly useful for identifying bone marrow edema, osteonecrosis, or soft tissue pathology (e.g., FHB tears).
Surgical Warning - Bipartite vs. Fracture: A bipartite tibial sesamoid is present in approximately 10% of the population, and in 25% of these individuals, the condition is bilateral. The surgeon must definitively differentiate a tender sesamoid with a radiolucent division from a true fracture. Bipartite sesamoids typically have smooth, sclerotic margins, whereas acute fractures exhibit sharp, irregular, non-sclerotic edges.
The fibular sesamoid is rarely bipartite. If clinical symptoms and routine radiographs suggest a fracture of the fibular sesamoid, one is almost certainly present.


Fig. 78-100 Oblique radiography is helpful for evaluating the fibular sesamoid that rests between the first and second metatarsals; note the irregular lucency, indicating a traumatic etiology.

Fig. 78-101 Axial sesamoid view showing a fracture of the tibial sesamoid.
CONSERVATIVE MANAGEMENT
The initial treatment algorithm depends entirely on the severity of the clinical and radiographic findings.
Conditions such as uncomplicated sesamoiditis, osteochondritis, acute calcific tendinitis (usually affecting the lateral head of the FHB), chronic FHB tendinitis, and localized bursitis should undergo an exhaustive trial of nonoperative management.
Conservative Modalities Include:
* Nonsteroidal anti-inflammatory drugs (NSAIDs).
* Strict modification of weight-bearing activities (cessation of running/jumping).
* Full-length custom shoe orthoses featuring a metatarsal pad and a specific relief (offloading well) beneath the first metatarsal head.
* Footwear modifications, such as a rigid Morton's extension or a metatarsal bar on the sole.
* Cast immobilization or a controlled ankle motion (CAM) boot for 4 to 6 weeks in acute, highly symptomatic cases.
This conservative regimen must be continued for several months (typically a minimum of 6 months) before declaring failure.

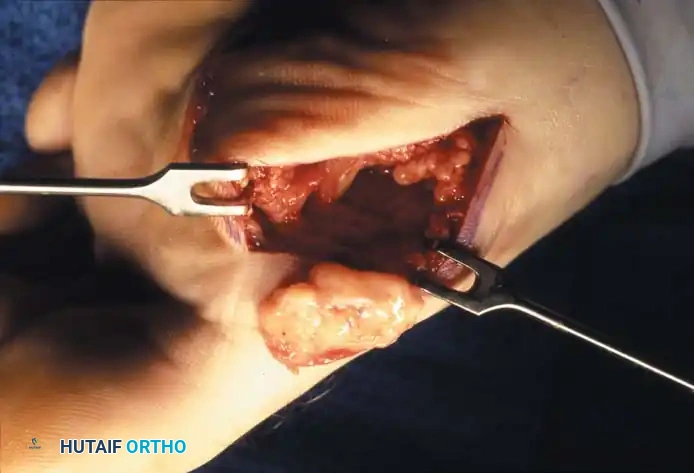
Fig. 78-99 A and B, Plantar flexed first ray with callus beneath the tibial sesamoid. C, On a Harris pressure mat, note the increased pressure beneath the tibial sesamoid. D, The tibial sesamoid has been removed, and the articular surface and corresponding facet of the metatarsal head show degenerative changes.
SURGICAL MANAGEMENT: SESAMOIDECTOMY
If conservative measures fail to provide relief, excision of the offending sesamoid is indicated. Surgical intervention is most frequently required for nonunions of fractures, painful exostoses, persistent bursitis, and intractable painful keratoses.
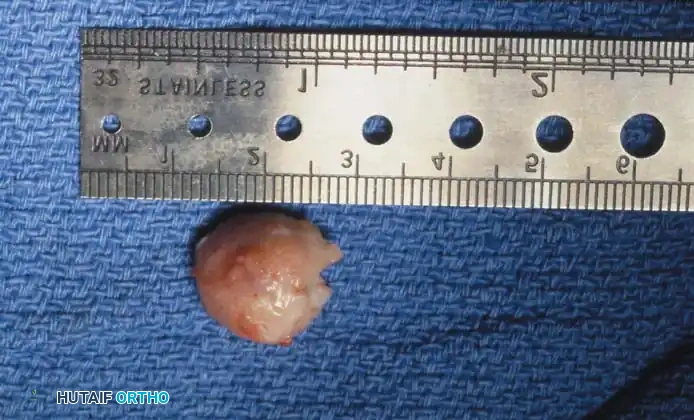

Fig. 78-102 A, Exostosis on the plantar surface of the tibial sesamoid. B, Patient had a keratotic lesion with intermittent ulceration. Excision of the sesamoid is indicated.
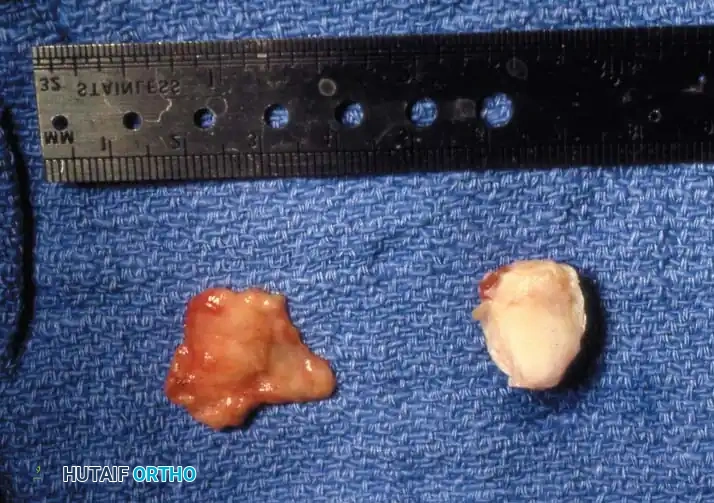


Fig. 78-103 A and B, Persistent keratotic lesion and bursa beneath the tibial sesamoid. C, Sesamoid and overlying bursa removed. Radiographs, including the axial sesamoid view, were normal.

Fig. 78-104 Diffuse keratosis that persisted over a protracted period and was unresponsive to nonoperative management.
Athletic Considerations and Outcomes
Sesamoidectomy is frequently performed in athletically active patients who demand a rapid return to high-level sports. However, surgeons must counsel patients that postoperative complications can significantly delay this return.
In a landmark study by Saxena and Krisdakumtorn, it was reported that 11 professional or varsity athletes returned to sports at an average of 7.5 weeks following sesamoidectomy, whereas 13 recreational athletes returned in an average of 12 weeks.
Potential Complications Include:
* Iatrogenic Deformity: Development of hallux varus (following fibular sesamoidectomy) or hallux valgus (following tibial sesamoidectomy) due to intrinsic muscle imbalance.
* Neuroma: Postoperative scarring entrapping the proper digital nerve, leading to severe neuroma-like symptoms.
* Stiffness: Arthrofibrosis of the first MTP joint.
Operative Technique: Excision of the Tibial Sesamoid (Technique 78-34)
Meticulous surgical technique is paramount to preserve the FHL tendon and prevent postoperative coronal plane deformities of the hallux.
Step 1: Incision and Approach
* Make a 3-cm longitudinal incision along the medial aspect of the first MTP joint (Fig. 78-105A).
* Alternative: A plantar midline incision can be utilized if the capsule is to be opened and turned plantarward, allowing the sesamoid to be removed from the inside out.
* Pitfall: The proper digital branch of the medial plantar nerve (supplying the medial side of the hallux pulp) is highly vulnerable with the plantar incision. The straight medial incision utilizes a safer internervous plane (Fig. 78-105B). However, the plantar approach requires less capsular disruption.
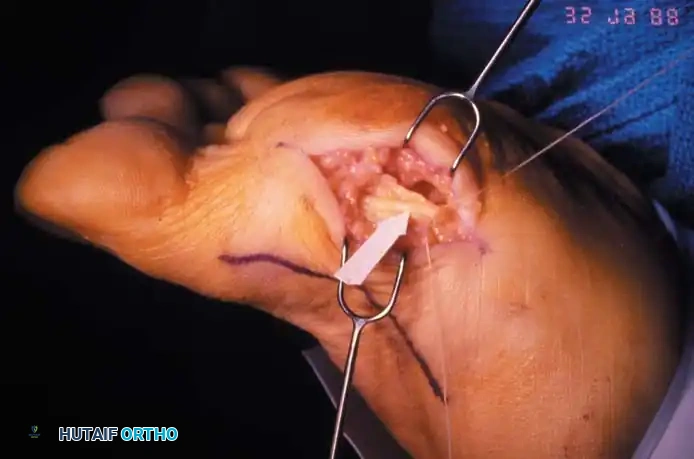

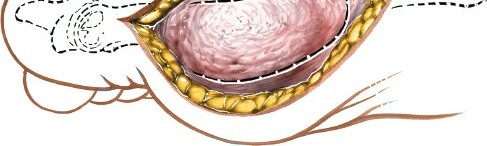
Fig. 78-105 Removal of tibial sesamoid. A, Optional incision. B, Arrow and suture delineate the proper digital nerve to the medial side of the hallux. The nerve blends with the capsule and subcutaneous tissue, making it vulnerable by position and appearance.
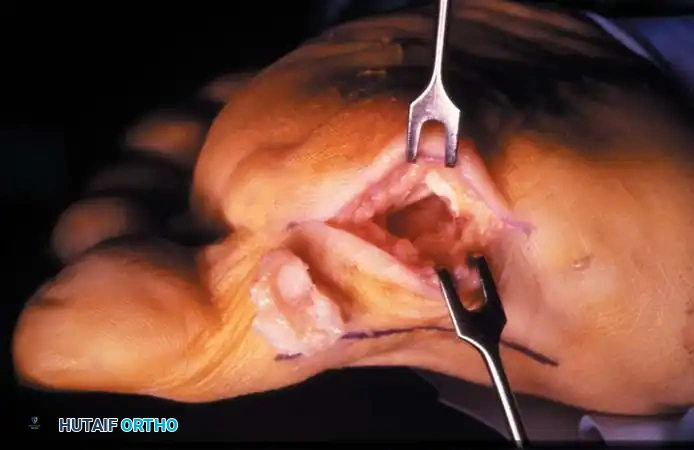
Step 2: Identification and Enucleation
* Locate the tibial sesamoid via direct palpation, carefully differentiating its contours from the first metatarsal head.
* Begin to "shell" the sesamoid out of the capsule and plantar plate by sharply incising across its plantar and articular surfaces.
* Critical Step: Remain constantly aware of the flexor hallucis longus (FHL) tendon, which lies immediately adjacent in the intersesamoid groove. Iatrogenic laceration of the FHL is a devastating complication.
Step 3: Excision and Soft Tissue Management
* Once the FHL is definitively identified and protected, keep the great toe flexed at
Associated Surgical & Radiographic Imaging
You Might Also Like