INTRODUCTION TO DEEP-SEATED JOINT INFECTIONS
The operative management of deep-seated joint infections—particularly those involving the sacroiliac (SI) joint, the hip, and the axial skeleton—presents a formidable challenge to the orthopedic surgeon. Due to their deep anatomical locations and complex surrounding neurovascular structures, these infections often present with vague, non-specific symptoms that delay diagnosis. When conservative measures and targeted antibiotic therapies fail, or when chronic sepsis leads to extensive osteomyelitis and joint destruction, aggressive surgical intervention becomes mandatory.
This comprehensive guide details the evidence-based protocols for diagnosing and managing acute septic arthritis of the sacroiliac, sternoclavicular, and acromioclavicular joints. Furthermore, it provides an exhaustive, step-by-step technical breakdown of the Girdlestone resection arthroplasty—a critical salvage procedure for chronic, intractable hip sepsis.
SACROILIAC JOINT SEPTIC ARTHRITIS
Acute septic arthritis of the sacroiliac joint is an uncommon but clinically significant entity. It typically arises via hematogenous seeding of the anterior synovial portion of the joint. Because the posterior aspect of the SI joint is syndesmotic and heavily reinforced by interosseous ligaments, infections predominantly localize anteriorly, complicating both diagnosis and surgical access.
Clinical Presentation and Provocative Testing
Patients classically present with unilateral buttock pain. However, due to the complex innervation of the SI joint (L2-S3 nerve roots) and its proximity to the lumbosacral plexus, patients commonly exhibit referred pain patterns, including low back, thigh, and even abdominal pain. This can mimic acute abdominal pathology, lumbar radiculopathy, or septic hip arthritis.
Accurate clinical diagnosis relies heavily on provocative physical examination maneuvers designed to stress the SI joint:
* Iliac Compression Test: With the patient in the lateral decubitus position, downward pressure is applied to the superior iliac crest. This compresses the SI joint, eliciting sharp pain in the presence of inflammation.
* Patrick’s (FABER) Test: Flexion, Abduction, and External Rotation of the ipsilateral hip places stress on the SI joint. Posterior pain during this maneuver strongly suggests SI joint pathology.
* Gaenslen’s Test: The patient lies supine with the asymptomatic leg flexed to the chest. The symptomatic leg is allowed to drop off the edge of the examination table into extension, creating a rotational shear force across the SI joint that elicits pain.
Diagnostic Imaging
Routine anteroposterior and oblique radiographs of the pelvis are usually normal in the early stages of the disease, as visible bony destruction lags behind the clinical infection by 14 to 21 days.
Clinical Pearl: Do not rely on plain radiographs to rule out acute SI joint sepsis. Advanced imaging must be obtained if clinical suspicion remains high.
- Radionuclide Scans: Technetium-99m (bone turnover) and Gallium-67 (inflammation) scans usually demonstrate increased focal activity and are highly sensitive, though they lack specificity.
- Computed Tomography (CT): CT remains the most sensitive diagnostic study for evaluating the osseous architecture. It excels at identifying early cortical erosions, joint space widening, and adjacent osteomyelitis of the sacrum or ilium.
- Magnetic Resonance Imaging (MRI): MRI is highly beneficial for evaluating the soft tissue envelope, identifying joint effusions, and detecting adjacent intrapelvic or iliopsoas abscesses.
Fluoroscopically Guided Aspiration Technique
Isolation of the causative organism is paramount. Miskew, Block, and Witt described a highly effective, standardized technique for SI joint aspiration that successfully yields diagnostic material in the vast majority of patients.
Step-by-Step Aspiration Protocol:
1. Positioning: Place the patient prone on a radiolucent table.
2. Needle Selection: Utilize an 18-gauge spinal needle to ensure adequate stiffness and lumen size for aspirating potentially viscous purulent material.
3. Entry Point: Introduce the needle in the midline at the level of the sacroiliac joint.
4. Trajectory: Advance the needle at a 45-degree angle with the transverse plane and a 30-degree angle with the sagittal plane.
5. Advancement: Pass the needle laterally and distally along these specific angles.
6. Fluoroscopic Guidance: Utilize continuous or intermittent image intensification to guide the needle tip directly into the sacroiliac joint, targeting a point exactly 0.5 cm from its most inferior margin.
Most patients respond favorably to prompt, culture-directed intravenous antibiotic therapy following successful aspiration. However, patients who develop an organized abscess require formal open surgical drainage. Osteomyelitis of the adjacent sacrum or ilium is a common complication that may necessitate aggressive bone debridement.
CHRONIC SEPSIS OF THE HIP: THE GIRDLESTONE RESECTION
When deep-seated sepsis of the hip becomes chronic, persistent, and refractory to standard debridement and antibiotic therapy, a Girdlestone resection arthroplasty is indicated. Originally described by Gathorne Robert Girdlestone, this procedure is considered a definitive salvage operation—a "last resort" designed to eradicate infection by completely excising the infected joint and creating a saucerized cavity that heals by secondary intention.
Indications and Preoperative Planning
The Girdlestone resection is most frequently utilized in:
* Paraplegic or quadriplegic patients with chronic hip sepsis, often secondary to contiguous spread from massive ischial or trochanteric decubitus ulcers (as described by Klein et al.).
* Patients with failed, infected total hip arthroplasties where reimplantation is contraindicated due to severe bone loss, highly virulent organisms, or poor host medical status.
* Chronic, destructive septic arthritis leading to intractable osteomyelitis of the proximal femur and acetabulum.
Preoperative Optimization:
Before proceeding to the operating room, comprehensive planning is required. Sinograms should be obtained to map the extent of fistulous tracts and identify hidden abscess cavities. Appropriate broad-spectrum or culture-directed antibiotic therapy must be initiated. Because this procedure involves extensive resection of vascularized muscle and bone, significant intraoperative blood loss is anticipated; adequate amounts of cross-matched blood must be available.
Surgical Technique: Girdlestone Resection (Technique 17-18)
The primary objective of the Girdlestone resection is the complete removal of all necrotic bone and infected tissue, transforming a complex, deep, closed space into an open, saucerized cavity that allows for unimpeded dependent drainage.
Step 1: Incision and Superficial Exposure
* Position the patient in the lateral decubitus position.
* Begin a transverse incision approximately 2.5 cm posterior and distal to the anterior superior iliac spine (ASIS).
* Extend the incision laterally until the center of the incision is located about 2.5 cm proximal to the tip of the greater trochanter.
* Retract the skin edges and meticulously expose the thick fascia overlying the gluteus medius and the anterior portion of the gluteus maximus.
Step 2: Deep Dissection and Muscle Resection
* Make two deep incisions directly in line with the edges of the retracted skin incision.
* In the proximal incision, divide the gluteal musculature down to the outer table of the ilium, just proximal to the superior rim of the acetabulum.
* In the distal incision, expose the lateral aspect of the greater trochanter.
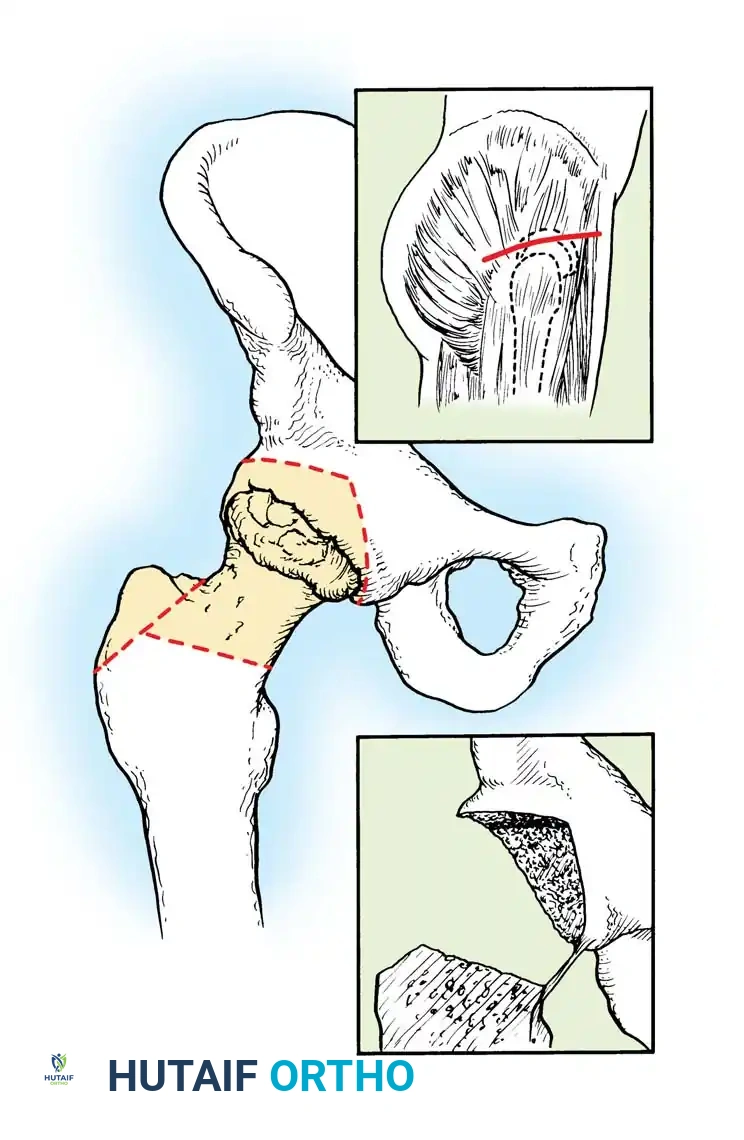
Step 3: Resection of the Greater Trochanter
* Utilize a broad osteotome. Direct it proximally and obliquely toward the superior aspect of the base of the femoral neck.
* Resect the greater trochanter in its entirety.
* Remove the resected trochanter en bloc with the previously incised mass of infected or necrotic gluteal muscles. This step is critical for achieving the necessary "saucerization" of the lateral hip.
Step 4: Capsulotomy and Femoral Head Resection
* Incise the thick, often fibrotic hip capsule to expose the femoral head, femoral neck, and the acetabular rim.
* Surgical Decision Making: Do not resect the femoral head if it is definitively not necrotic or if the hip is already solidly ankylosed (though in the context of chronic sepsis, the head is almost universally involved). Otherwise, use an oscillating saw or osteotome to divide the femoral neck and acetabular rim, and completely remove the femoral head and neck.
Step 5: Acetabular Debridement and Intrapelvic Drainage
* Aggressively curet all necrotic, sclerotic, and infected bone from the acetabulum and the adjacent ilium.
* Use a high-speed burr if necessary to reach bleeding, healthy bone. Leave only raw surfaces of highly vascular cancellous bone.
* Carefully probe the medial wall of the acetabulum. Ensure that any intrapelvic abscess communicating with the joint is drained adequately.
Surgical Warning: When debriding the medial wall of the acetabulum or draining intrapelvic abscesses, exercise extreme caution to avoid iatrogenic injury to the external iliac vessels and the obturator neurovascular bundle.
Step 6: Medial Extension for Adductor Abscesses
* If preoperative imaging or intraoperative exploration reveals an abscess extending from the lesser trochanter into the medial adductor compartment, a secondary incision is required.
* Make a longitudinal incision on the medial side of the proximal thigh.
* Resect sufficient portions of the pectineus, adductor longus, and adductor brevis muscles to unroof the abscess and provide free, dependent drainage.
Step 7: Closure and Packing
* Partially advance the skin flaps over the remaining healthy muscle at the time of closure to reduce the size of the defect, but do not close the wound tightly.
* Insert two or three large-bore drains into the deepest portions of the acetabulum and the medial thigh (if opened).
* Fill the remaining saucerized cavity loosely with petrolatum gauze to maintain the open space and promote healing by secondary intention from the base of the wound outward.
Postoperative Protocol and Aftertreatment
The postoperative management of a Girdlestone resection is as critical as the surgery itself. The primary goal is to maintain the saucerized space and prevent the proximal femur from migrating superiorly and obliterating the drainage cavity.
- Immobilization: The hip must be immobilized in a spica cast or placed in skeletal traction (via a distal femoral or proximal tibial pin) in 20 to 30 degrees of flexion.
- Prevention of Proximal Migration: According to Girdlestone’s original principles, it is absolutely imperative that proximal displacement of the femur be prevented. If the femur is allowed to migrate proximally, it will abut the acetabulum, effectively blocking drainage from the deep pelvic cavity and defeating the entire purpose of the saucerization operation.
- Wound Care: The petrolatum gauze packing is gradually advanced and removed over several weeks, allowing the massive cavity to granulate and heal by secondary intention.
INFECTIONS OF THE STERNOCLAVICULAR AND ACROMIOCLAVICULAR JOINTS
While axial infections frequently involve the SI joint and hip, the sternoclavicular (SC) and acromioclavicular (AC) joints are also susceptible to septic arthritis, albeit under specific clinical circumstances.
Pathogenesis and Microbiology
Usually, the SC and AC joints are affected only in the setting of overwhelming polyarticular acute septic arthritis, or, more commonly, in the intravenous drug user (IVDU) population.
Historically, Pseudomonas aeruginosa was a frequent culprit in injection drug users; however, the incidence of Pseudomonas infections in this demographic declined dramatically in the 1980s. Today, the causative organism is predominantly Staphylococcus aureus, including methicillin-resistant strains (MRSA). Isolated cases of SC and AC joint sepsis have also been described in otherwise healthy adults without a history of intravenous drug use, often secondary to transient bacteremia.
Operative Intervention
Because both the sternoclavicular and acromioclavicular joints are subcutaneous, they are highly accessible for both diagnostic and therapeutic interventions.
- Aspiration: Direct anterior aspiration is easily accomplished. For the SC joint, care must be taken not to advance the needle too deeply, as the brachiocephalic vein and other critical mediastinal structures lie immediately posterior to the joint capsule.
- Surgical Drainage: If an abscess forms or if the infection fails to clear with serial aspirations and antibiotics, formal open surgical drainage is indicated. The subcutaneous nature of these joints allows for straightforward anterior approaches.
- Bone Resection: In cases of delayed presentation or highly virulent organisms, the infection may progress to osteomyelitis of the clavicle. Occasionally, a portion of the medial clavicle (for SC joint infections) or the distal clavicle (for AC joint infections) needs to be excised to achieve clear margins and eradicate the infection.
